
Abstract
A 17-year-old, Thoroughbred mare was presented for necropsy with a large, invasive oral mass determined via immunohistochemistry to be a soft tissue sarcoma of neural origin. Oral sarcomas are rare in veterinary medicine, and to the authors' knowledge, this is the first oral sarcoma of neural tissue origin reported in a horse.
Tumors of the oral cavity are diagnosed only sporadically in horses. The most common tumor is squamous cell carcinoma, occurring most commonly on the gingiva but also occurring throughout the oral cavity including the hard palate, pharynx, tongue, soft palate, and guttural pouches. 3 Additional oral tumors or proliferative disorders that have been reported in the mouths of horses include ameloblastic carcinoma, 1 dental cementomas, 5 atypical perineurial cell proliferative disorder, 11 and congenital hemangiosarcoma. 2
Differential Diagnoses
Grossly, the differentials for this oral mass are dental cementoma, squamous cell carcinoma, ameloblastic carcinoma, and congenital hemangiosarcoma.
History and Gross Findings
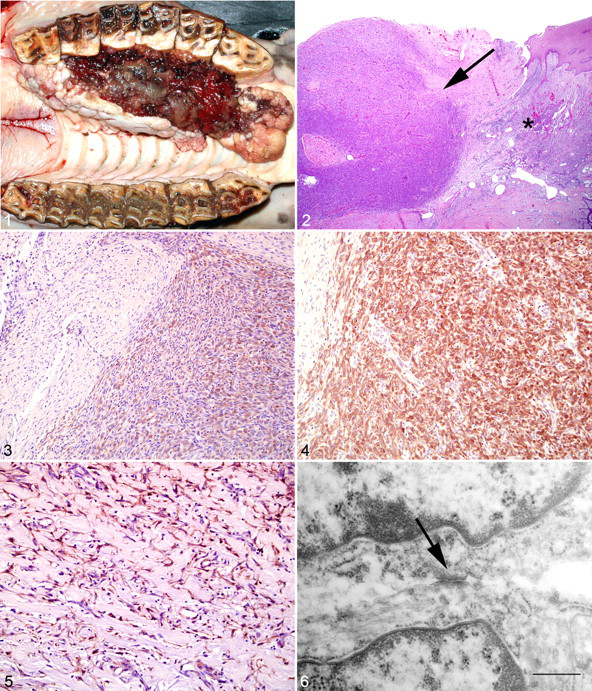
A 17-year-old Thoroughbred mare was initially presented for oral mass of approximately 7 months duration. After clinical examination, the owner elected euthanasia due to a poor prognosis. At necropsy, a 19 × 6 × 5 cm, multinodular, expansile, and ulcerated mass with pedunculations at the cranial aspect was noted on the right side of the hard palate. The mass displaced the maxillary cheek teeth laterally approximately 2 to 3 cm (Fig. 1 ). The mass effaced the hard palate and was firm and tan on cut surface.
Microscopic Findings
The mass was fixed by immersion in 10% neutral buffered formalin, embedded in paraffin, sectioned at 3 to 5 μm, processed routinely, and stained with hematoxylin and eosin. Histologically, the deep submucosa contained large, multifocal to coalescing, unencapsulated, well-circumscribed, densely cellular nodules of neoplastic spindle cells (Fig. 2 ). The spindle cells were arranged in streams and packets within a fine fibrovascular stroma. The cells had a small amount of vacuolated eosinophilic cytoplasm with indistinct cell borders. The nuclei were large and ovoid to cigar shaped with finely stippled chromatin. Mitotic figures were less than 1 per 10 high-power fields and anisocytosis was mild, whereas anisokaryosis was moderate to marked. The superficial submucosa was sparsely cellular and had scattered individual stellate cells within an edematous fibrovascular stroma. The stellate cells had a moderate amount of basophilic cytoplasm and round to ovoid nuclei with finely stippled chromatin. The overlying mucosal epithelium was moderately hyperplastic with large, anastomosing rete pegs of variable thickness and thick parakeratotic layers of hyperkeratosis. Multifocally, the oral mucosal surface was ulcerated. Large numbers of neutrophils admixed with fewer lymphocytes, histiocytes, and plasma cells infiltrated the subjacent stroma. Metastasis was not seen in the remainder of the mouth or in any thoracic or abdominal viscera.
For immunohistochemical evaluation, the formalin-fixed, paraffin-embedded mass was sectioned at 3 to 5 μm and placed on positively charged slides. The neoplastic spindle cells stained negatively for cytokeratin (AE1/AE3) (1:50), desmin (1:50), sarcomeric actin (1:125), glial fibrillary acidic protein (GFAP) (1:500), smooth muscle actin (1:100) (all from DakoCytomation Inc., Carpinteria, CA), and melan-A (1:40) (Vector Laboratories, Inc., Burlingame, CA). The cytoplasm was densely positive for S-100 (1:400) (Fig. 3 ) and vimentin (1:50) (both from DakoCytomation Inc.), and the cytoplasm and occasional nuclei were strongly positive for neuron-specific enolase (NSE) (1:150) (DakoCytomation Inc.) (Fig. 4 ). The submucosal stellate cells had dense cytoplasmic staining with smooth muscle actin (Fig. 5 ) and vimentin and moderate cytoplasmic staining with S-100 and neuron-specific enolase but were negative for cytokeratin (AE1/AE3), melan-A, desmin, sarcomeric actin, and GFAP.
Portions of the formalin-fixed mass were processed for transmission electron microscopy. Ultrastructurally, the neoplastic spindle cells had moderate numbers of mitochondria within the cytoplasm and frequently had intercellular junctions, consistent with the morphology of desmosomes (Fig. 6 ), between neoplastic cells. The submucosal stellate cells in the stroma were elongate with bundles of cytoplasmic actin filaments running parallel to the long axis of the cells.
Diagnosis
Based on the staining characteristics of this tumor, this is a sarcoma of neural tissue origin, possibly a peripheral nerve sheath tumor.
Discussion
S-100 protein is typically associated with melanocytes or cells of neural origin such as glial cells, neural cells, and Schwann cells. Less frequently, S-100 protein is associated with some mesenchymal cells such as adipocytes or chondrocytes. 8 Desmosomes are most frequently associated with epithelial cells, but meninges and cardiomyocytes and perineurial cells (such as Schwann cells) are known to have desmosomes as well. 9 Based on the results of S-100 positivity, NSE positivity, and the presence of desmosomes, the neoplastic cells are considered to be most likely of neural tissue origin. Common neural tissue tumors of peripheral nervous origin are perineuriomas, neurofibromas, and peripheral nerve sheath tumors. Usually only Schwann cells are S-100 positive, whereas the remaining peripheral nerve sheath cells are S-100 negative. 10 Additionally, perineuriomas are generally well demarcated and composed of whorling spindloid mesenchymal cells.
The possible diagnoses of melanoma, muscle tumors, salivary gland myoepithelioma, and fibrosarcoma are considered unlikely given the immunohistochemical and ultrastructural properties noted. The remaining possible tissue is neural, making peripheral nerve sheath tumor or related neoplasm the most likely neoplasm.
This case also had a large population of stellate cells in the submucosa between the mucosal epithelium and the deeper neoplastic tissue. The stellate cells were determined to be myofibroblasts based upon immunopositivity with smooth muscle actin and the presence of actin filaments within the cytoplasm identified with electron microscopy. 4,6,7 This myofibroblastic cell population is considered to be reactive to chronic inflammation from chronic irritation and friction in the mouth. Myofibroblasts are commonly found in granulation tissue and are responsible for contraction of granulation tissue to create a scar.
This is a unique case because neural tissue neoplasms are relatively uncommon in the oral cavity of domestic animals. Humans tend to develop neural tissue neoplasms with relative frequency, consisting of perineuriomas, peripheral nerve sheath tumors, and neurofibromas. To the authors' knowledge, this is only the second time a neural tissue proliferative disorder has been reported in the equine oral cavity and the first time a soft tissue sarcoma of neural origin has been reported.
Footnotes
Acknowledgements
We thank Cheryl Crowder, Hal Holloway, Kendra Shultz, and Julie Millard for their tireless assistance in preparing the slides and performing immunohistochemistry. We would also like to thank Olga Borkhsenious for her help with the electron microscopy images.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Financial Disclosure/Funding
The authors declared that they received no financial support for their research and/or authorship of this article.