
Abstract
Editor:
We recently read with interest an article by Loynachan et al describing equine mixed hepatoblastoma with teratoid features in 2 neonates and a fetus. 5 The authors reviewed the veterinary literature and noted that hepatoblastomas had been reported in mice, horses (n = 4), sheep, pigs, a dog, a bull, and an alpaca. The authors suggested that their cases are the first reported showing “teratoid features.” It is with this last statement that we disagree—not simply with the claim of priority but rather the accuracy of the diagnoses.
Hepatoblastoma, a malignant hepatic neoplasm primarily occurring in children under the age of 5 years, is typically divided into two broad categories: pure epithelial or mixed epithelial–mesenchymal. The former is subcategorized as fetal, embryonal, mixed fetal–embryonal (most common), and a few other, rarer types not relevant to the present discussion; the latter contain immature mesenchymal components, and a small subset of these cases is further subclassified as being mixed with teratoid features.
The authors cited a source containing a 1.24-page description of hepatoblastomas and the following 2 sentences: “Other elements, namely cartilage, bone, striated muscle and neural tissue, are rarely seen; the term ‘teratoid’ is attached to these elements.” 1 Although it would intuitively seem that any of the above should be enough to demonstrate teratoid features, this is not true. The overwhelming majority of pediatric pathologists and authors of human pediatric, liver, and oncologic pathology textbooks consider the presence of osteoid, bone, and cartilage—the “teratoid” elements in the 3 reported equine cases—to fall within the diagnostic realm of mesenchymal components. The authors noted the presence of extramedullary hematopoiesis as further evidence; 5 however, many pure epithelial hepatoblastomas have significant extramedullary hematopoiesis. 1
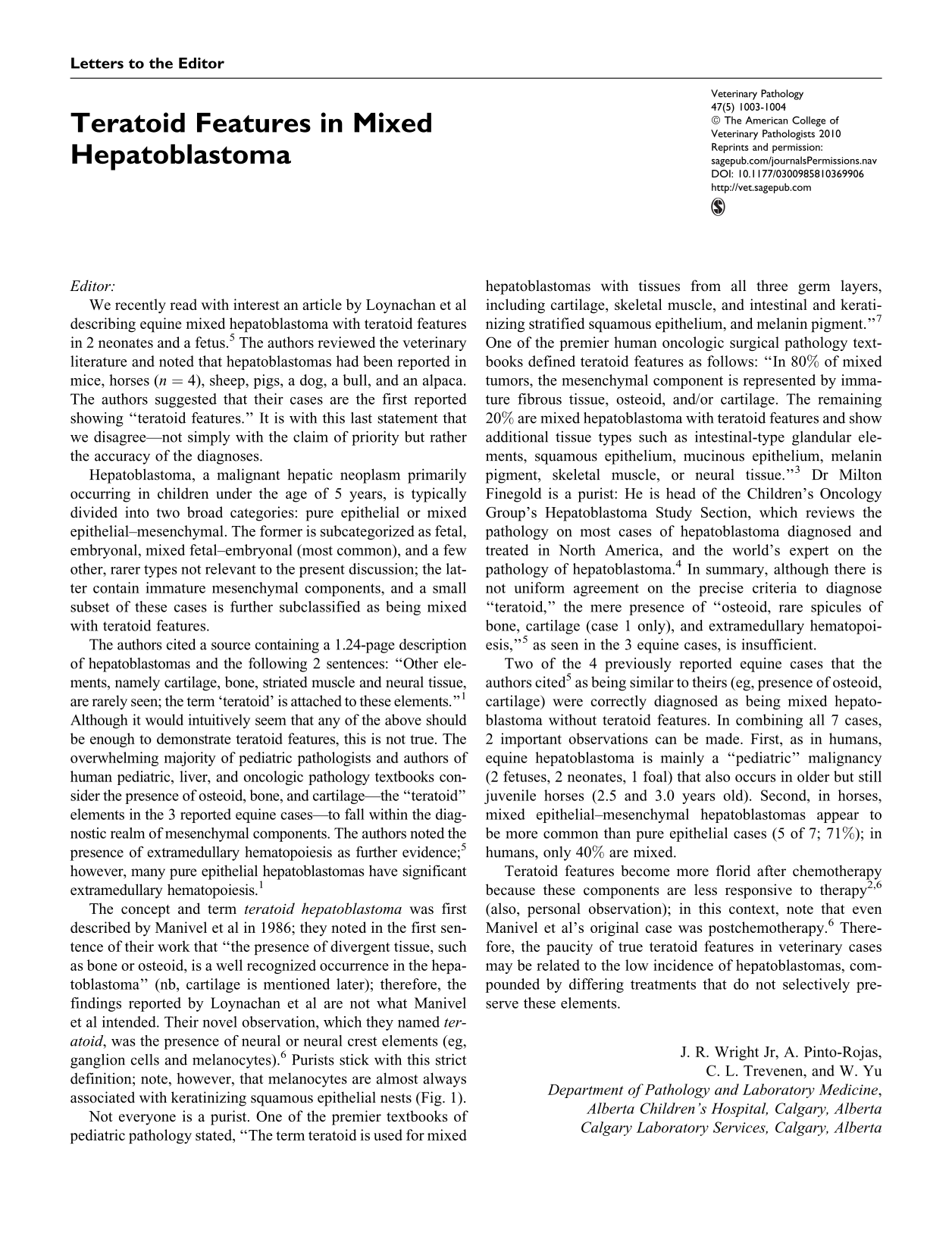
The concept and term teratoid hepatoblastoma was first described by Manivel et al in 1986; they noted in the first sentence of their work that “the presence of divergent tissue, such as bone or osteoid, is a well recognized occurrence in the hepatoblastoma” (nb, cartilage is mentioned later); therefore, the findings reported by Loynachan et al are not what Manivel et al intended. Their novel observation, which they named teratoid, was the presence of neural or neural crest elements (eg, ganglion cells and melanocytes). 6 Purists stick with this strict definition; note, however, that melanocytes are almost always associated with keratinizing squamous epithelial nests (Fig. 1 ).
Liver; human child. Postchemotherapy teratoid hepatoblastoma with extensive melanocytic differentiation in the context of florid nests of keratinizing squamous epithelium, glandular epithelium, and osteoid. Inset: multiple mature ganglion cells. Other elements, not depicted, include bone and cartilage. HE.
Not everyone is a purist. One of the premier textbooks of pediatric pathology stated, “The term teratoid is used for mixed hepatoblastomas with tissues from all three germ layers, including cartilage, skeletal muscle, and intestinal and keratinizing stratified squamous epithelium, and melanin pigment.” 7 One of the premier human oncologic surgical pathology textbooks defined teratoid features as follows: “In 80% of mixed tumors, the mesenchymal component is represented by immature fibrous tissue, osteoid, and/or cartilage. The remaining 20% are mixed hepatoblastoma with teratoid features and show additional tissue types such as intestinal-type glandular elements, squamous epithelium, mucinous epithelium, melanin pigment, skeletal muscle, or neural tissue.” 3 Dr Milton Finegold is a purist: He is head of the Children’s Oncology Group’s Hepatoblastoma Study Section, which reviews the pathology on most cases of hepatoblastoma diagnosed and treated in North America, and the world’s expert on the pathology of hepatoblastoma. 4 In summary, although there is not uniform agreement on the precise criteria to diagnose “teratoid,” the mere presence of “osteoid, rare spicules of bone, cartilage (case 1 only), and extramedullary hematopoiesis,” 5 as seen in the 3 equine cases, is insufficient.
Two of the 4 previously reported equine cases that the authors cited 5 as being similar to theirs (eg, presence of osteoid, cartilage) were correctly diagnosed as being mixed hepatoblastoma without teratoid features. In combining all 7 cases, 2 important observations can be made. First, as in humans, equine hepatoblastoma is mainly a “pediatric” malignancy (2 fetuses, 2 neonates, 1 foal) that also occurs in older but still juvenile horses (2.5 and 3.0 years old). Second, in horses, mixed epithelial–mesenchymal hepatoblastomas appear to be more common than pure epithelial cases (5 of 7; 71%); in humans, only 40% are mixed.
Teratoid features become more florid after chemotherapy because these components are less responsive to therapy 2,6 (also, personal observation); in this context, note that even Manivel et al’s original case was postchemotherapy. 6 Therefore, the paucity of true teratoid features in veterinary cases may be related to the low incidence of hepatoblastomas, compounded by differing treatments that do not selectively preserve these elements.