
Abstract
Background:
Non–clear cell renal cell carcinoma (nccRCC) represents a heterogeneous group of rare malignancies with limited evidence guiding systemic therapy. The recent introduction of immune checkpoint inhibitors (ICIs) and their combinations with tyrosine kinase inhibitors (TKIs) has shown promising results, but real-world data remain scarce.
Methods:
We retrospectively collected clinical and pathological data from patients with metastatic nccRCC included in the Italian Meet-URO-23/I-RARE database and from Vall d’Hebron Institute of Oncology (VHIO). Prognostic factors for overall survival (OS) were analyzed using univariate and multivariate Cox regression. Treatment outcomes were assessed by histology and therapeutic regimen.
Results:
A total of 156 patients were included: papillary (56.4%), chromophobe (22.4%), translocated (10.9%), and unclassified (10.3%) RCC. Median OS was 17.5 months (95%CI 14.7–27.6) and median progression free survival (PFS) 10.2 months (95%CI 7.6–13.7). Patients treated with ICI-combinations (ICI plus ICI or ICI plus VEGF-TKI) showed significantly improved survival (median OS not reached vs 14.7 months for other regimens, p = 0.0053). The overall objective response rate (ORR) and disease free survival (DFS) for ICI+TKI was 53.3% (16/30 evaluable) and 93.3% (28/30), with ORR of 55.5% (10/18) in papillary and 46.1% (6/13) in chromophobe subtypes. In the overall ICI-combination group, ORR was 48%. In multivariate analysis, International Metastatic RCC Database Consortium (IMDC) score, presence of bone metastases, and type of first-line therapy were independently associated with OS.
Conclusions:
In this large international real-world cohort, ICI-based combinations demonstrated superior outcomes compared to other regimens in metastatic nccRCC. These results reinforce the role of immunotherapy combinations as a preferred first-line approach and confirm the IMDC score as a reliable prognostic tool in this population.
Introduction
Renal cell carcinoma (RCC) represents 4.1% of new diagnoses of cancer and 2.4% of death for cancer in the US. 1 Among the RCC, while the most frequent clear cell RCC represents the 75-80% of all renal carcinomas, the heterogeneous group of non-clear cell carcinomas accounts for 20-25%, according to WHO2022 classification. 2 It consists of various subtypes, characterized by different histology, biology and clinical behavior, with a diverse prognosis ranging from 11 to 28 months, for the metastatic disease.3,4 Due to the rarity of these tumors, there is a lack of large studies conducted on a single pathology, resulting in a scarcity of proper therapeutic standards for most of these histologies.
Over the last decade, several trials have evaluated vascular endothelial growth factor tyrosine kinase inhibitors (VEGF-TKIs) in non–clear cell renal cell carcinoma (nccRCC), demonstrating modest activity. The ESPN, ASPEN, and RECORD-3 trials assessed sunitinib in this setting, reporting objective response rates (ORR) ranging from 9% to 18%.5–7 More recently, the PAPMET trial showed higher activity of cabozantinib compared with sunitinib in papillary RCC, with an ORR of 23% versus 4%, 8 with a numerical but not statistically significant benefit in terms of overall survival (OS) for the cabozantinib group in the final analysis, 9 suggesting cabozantinib as the most active TKI in this subgroup.
Given the heterogeneity of nccRCC and the limited efficacy of VEGF-TKIs, 10 increasing attention has been directed toward immune checkpoint inhibitors (ICIs). Phase II studies evaluating single agent nivolumab or pembrolizumab showed evidence of antitumor activity, although clinical benefit appeared limited.11–14 Dual immune checkpoint blockade with nivolumab plus ipilimumab further showed activity in non–clear cell histologies, as reported in the CheckMate 920 15 and SUNNIFORECAST trials. 16
In addition, combinations of ICIs with VEGF-targeted agents have yielded encouraging results in nccRCC. Phase I–II studies investigating bevacizumab plus atezolizumab, 17 cabozantinib plus atezolizumab 18 or nivolumab, 19 and lenvatinib plus pembrolizumab 20 reported ORRs ranging from approximately 25% to 50%. Real-world data, including an Italian multicenter observational study of pembrolizumab plus axitinib, 21 further support the activity of ICI–VEGF combinations in papillary and chromophobe RCC.
Due to the challenge of conducting large comparative studies among these regimens given the rarity of these diseases, it is difficult to determine which may perform better. We collected an international retrospective cohort of patients with metastatic nccRCC from the Italian Meet-URO-23/I-RARE database and from Vall d’Hebron Institute of Oncology (VHIO) of Barcelona (Spain) with the aim of conducting a descriptive analysis of the sample, assessing prognostic factors, and examining therapeutic outcomes based on the regimen used.
Materials and methods
We collected data of patients with nccRCC from Meet-URO 23/I-RARE database set, an Italian national retrospective and prospective registry of rare genitourinary tumors, and from VHIO in Barcelona. The study was approved by the regional ethical committees. Among the 399 patients enrolled, we included only those ones with metastatic or locally advanced not amenable to curative treatment disease (surgery or radiotherapy), and a diagnosis of papillary, chromophobe, translocated or unclassified renal carcinoma. Other inclusion criteria were age ⩾ 18 years, a diagnosis made within 10 years prior to the study start (March 2021) or up to five years afterwards and documented initial disease staging and histopathological characteristics. We excluded rarer histologies for a stronger statistical power and patients with collecting duct carcinoma (CDC), because they have pathological and clinical characteristics, as well as prognosis and type of treatment, that are very different from the other subgroups; moreover, we excluded patients with missing OS data and who did not receive a first-line treatment. As described in Figure 1, we selected 156 patients.

Consort diagram of study inclusion process. VHIO, Vall d’Hebron Institute of Oncology.
Categorical variables were reported as frequency and percentage and continuous variables as median and min-max range according to the distribution. Kaplan-Meier curves and Log-rank test were used to analyze overall survival (OS) and progression-free survival (PFS). For the treatment outcomes analysis, the OS was calculated as the time from the start of the first-line therapy to the date of death or last follow-up; PFS was calculated as the time expressed in months between the start of first-line treatment and the date of progressive disease (PD), according to RECIST v1.1; we excluded from the PFS analysis patients without the date of start of first-line treatment and/or the date of progressive disease. We used Kaplan-Meier curves and Log-rank test to compare overall survival (OS) between the immunotherapy combinations group (ICI-combination group), meant as those patients treated with ICI plus VEGF-TKI or bevacizumab and those treated with ICI plus ICI, and other treatment regimens; we also compared OS of patients treated with cabozantinib and those treated with other VEGF-TKIs. The conventional two-sided 5% level was chosen as the threshold of statistical significance.
Prognostic factors were investigated by univariate and multivariate analyses using Cox proportional hazard regression models. Clinically relevant variables in univariate analysis which resulted significantly correlated with OS entered in multivariate analysis. Multivariable analyses including IMDC score were performed on patients with complete IMDC data; no imputation for missing data was applied.
All statistical analyses were performed with R software (version 4.4.1, R Foundation for Statistical Computing, Vienna, Austria).
Results
Patients’ characteristics
Of 156 patients, 65 were collected from VHIO of Barcelona, while 91 were from Meet-URO 23/I-RARE database in Italy (Figure 1). The median age was 62 years old with a prevalence of males (70.5%). More than half of the patients (n = 88) had papillary RCC (56.4%), 35 had chromophobe RCC (22.4%), 17 translocated RCC (10.9%), while 16 had unclassified renal tumors (10.3%). Nearly 95% of the patients had a good clinical condition, with Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1 at the diagnosis of metastatic disease (Table 1). According to International Metastatic RCC Database Consortium (IMDC) Score, most of the patients were classified as intermediate/poor risk (57.7% and 26.9%, respectively), while only 15.4% were classified as good risk.
Patients’ baseline characteristics.

N, number of patients; ECOG PS, Eastern Cooperative Oncology Group Performance Status; IMDC, International Metastatic RCC Database Consortium.
Median OS was 17.5 months (95% CI 14.7 – 27.6) and median PFS was 10.2 months (95% CI 7.6 – 13.7) (Figure 2).

Progression free survival (on the left) and overall survival (on the right) for all patients.
Regarding type of first-line treatment, patients received cabozantinib, other VEGF-TKIs, ICI monotherapy, ICI plus ICI, ICI plus VEGF-TKI or bevacizumab and other (Table 2). ICI-combinations included cabozantinib plus nivolumab, pembrolizumab plus lenvatinib, pembrolizumab plus axitinib, ipilumumab plus nivolumab and cabozantinib plus atezolizumab. More than 50% of the patients received VEGF-TKIs (cabozantinib or other VEGF-TKIs) and nearly one third of the patients (n = 49) received immunotherapy combinations. Sixty-eight patients (43.6%) received second-line treatment, and 23 patients (14.7%) received third-line treatment (mainly cabozantinib) (Table 2).
Treatments.
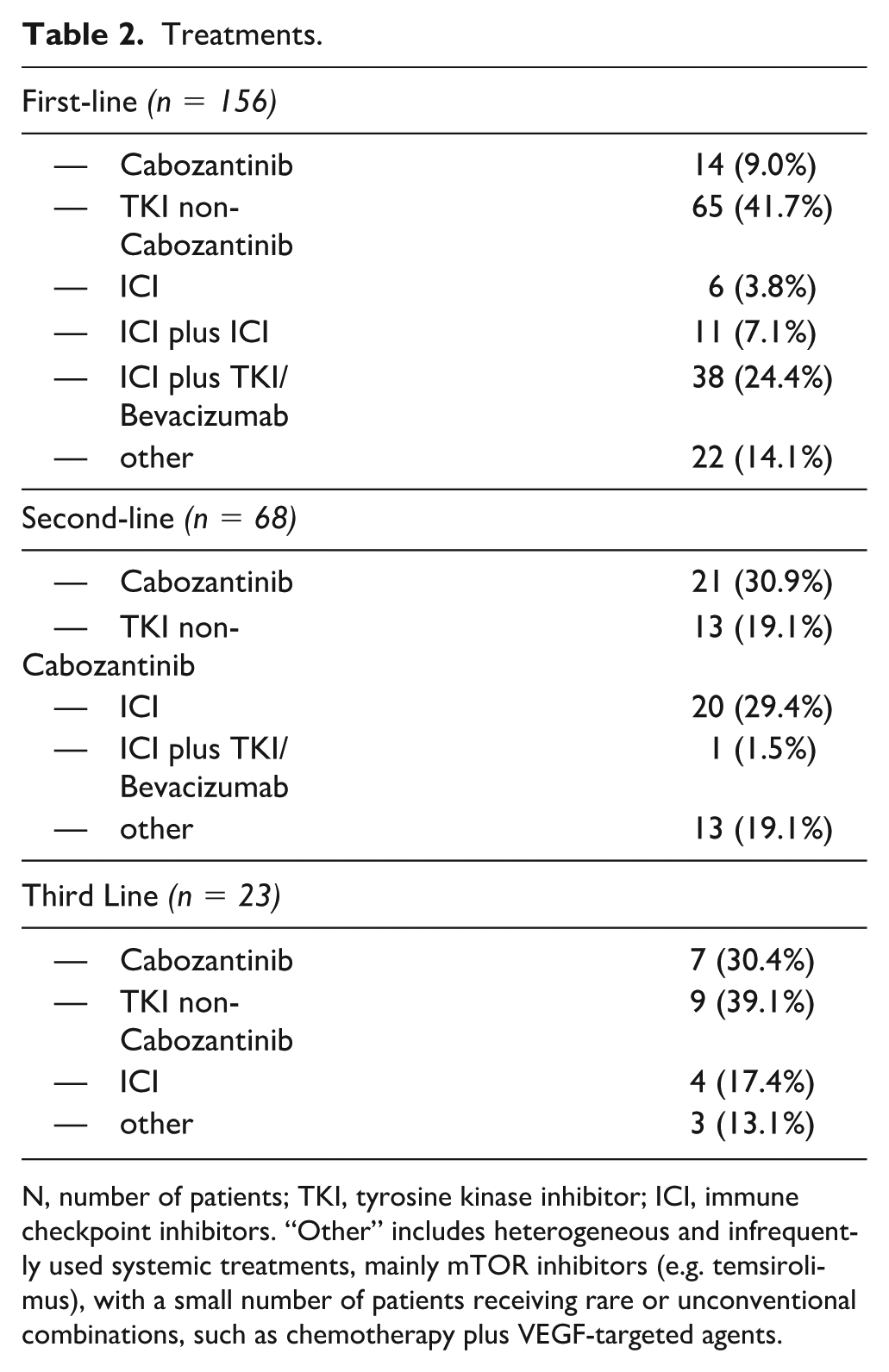
N, number of patients; TKI, tyrosine kinase inhibitor; ICI, immune checkpoint inhibitors. “Other” includes heterogeneous and infrequently used systemic treatments, mainly mTOR inhibitors (e.g. temsirolimus), with a small number of patients receiving rare or unconventional combinations, such as chemotherapy plus VEGF-targeted agents.
Prognostic factors
In the univariate analysis, the clinicopathological factors that were significantly associated with survival were histology, presence of bone metastases, IMDC score and type of first-line therapy (ICI-combination vs other treatments).
At the multivariate analysis, significant prognostic factors identified were bone metastases, associated with worse outcomes (HR 2.42, 95%CI: 1.13-5.18, p = 0.023), type of first-line-therapy, with patients treated in this setting with ICI-combination that showed better outcomes compared to other regimens (HR 0.30, 95%CI 0.14-0.67, p = 0.0034), and IMDC Score, where patients classified as poor-risk had significantly worse outcomes compared to those in the good-risk group (HR 10.66, 95%CI: 2.91-39.04, p = 0.0004) (Table 3).
Univariate and multivariate analysis.

HR, hazard ratio; ref, reference; CI, confidence interval.
Treatment outcomes
The survival analysis showed a significant advantage for the ICI-combination group, with a median OS not reached (NR, 95%CI 17.3-NR months) compared to 14.7 months in the other regimens (95%CI 10.7-22.7, p = 0.0053) (Figure 3). The median PFS in the ICI-combination group was 11.8 months (95%CI 8.9–NR). The overall objective response rate (ORR) for patients treated with ICI plus VEGF–TKI combinations was 53.3% (16 out of 30 evaluable patients), with ORR of 55.5% (10/18) in papillary and 46.1% (6/13) in chromophobe subtypes. Considering all ICI-combinations, including ICI–ICI regimens, the ORR was 48% (17 out of 35 evaluable patients), and only four patients (11.4%) showed progression at first evaluation. We also compared the outcomes of patients treated with cabozantinib (n = 14) versus other VEGF-TKIs (n = 65) as front-line treatment; the median OS for cabozantinib was significantly higher (NR vs 14.7 months, p = 0.05) (Figure 3).
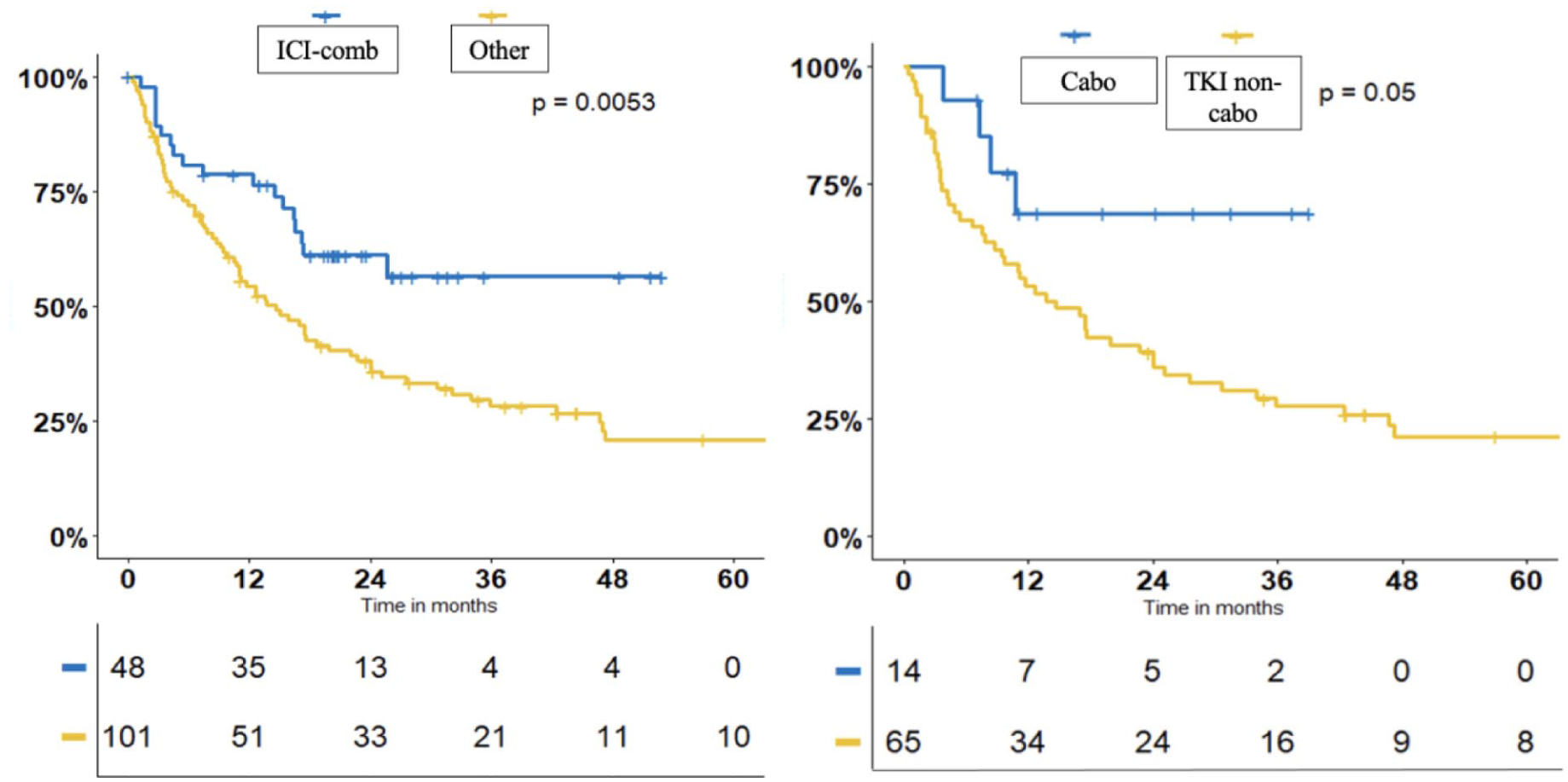
OS for ICI-combinations versus Other (on the left) and OS for Cabozantinib vs TKI non-cabozantinib. OS, overall survival; ICI-combinations, immune checkpoint inhibitors (ICI) plus ICI or ICI plus tyrosine kinase inhibitors (TKI) or bevacizumab.
Exploratory subgroup analyses were performed to further characterize treatment outcomes according to histology and type of ICI-based regimen. Progression-free survival and overall survival were analyzed separately in papillary and chromophobe RCC subgroups, and exploratory comparisons were conducted between ICI–ICI and ICI–VEGF-TKI regimens, as well as between ICI-based combinations and cabozantinib monotherapy. In these exploratory analyses, ICI–VEGF-TKI regimens showed numerically more favorable outcomes compared with ICI–ICI, and ICI-based combinations appeared to be associated with numerically improved outcomes compared with cabozantinib monotherapy. Given the limited sample sizes and the exploratory nature of these analyses, no formal comparative conclusions can be drawn. Detailed results are reported in the Online Supplementary Material.
Discussion
Given the rarity and heterogeneity of non-clear cell renal cell carcinoma (nccRCC), along with the frequent lack of established therapeutic standards, it is crucial to collect multicentric real world case series and share therapeutic approaches across centers, including those from different countries. This study represents a multicenter and international collaborative effort, highlighting the importance of international cooperation in understanding and managing these rare tumors.
Our demographic and clinical data are consistent with existing literature, demonstrating a median age of 62 years and a predominance of male patients (70.5%). The distribution of histological subtypes in our cohort, with papillary and chromophobe being the most common, aligns with known epidemiological patterns. These tumors typically grow slowly, with a high proportion diagnosed at a localized stage, often curable through surgical treatment. However, when metastatic, the prognosis is worse compared to metastatic clear cell RCC, a finding consistent with our study showing low OS in nccRCC patients.3,22,23
Regarding prognostic factors, our analysis underscores the relevance of the International Metastatic RCC Database Consortium (IMDC) score in nccRCC, confirming that it remains a valuable prognostic tool not only in patients with ccRCC but even in patients with non-clear cell subtypes treated with more contemporary regimens (i.e. cabozantinib or ICI combinations), as validated in other retrospective cohorts.24,25
The role of immunotherapy, particularly in combination with other therapies, has been well established in ccRCC and less clearly in nccRCC; our retrospective study strengthens this role, demonstrating that combinations of immune checkpoint inhibitors (ICIs) or ICIs with VEGF-TKIs are significantly associated with better outcomes. Our data suggest that combination therapy may be considered a good first-line choice in treating nccRCC, in accordance with indications by ESMO and NCCN guidelines based on phase II studies.15,17–20
In addition to immunotherapy, cabozantinib emerged as a superior option compared to other VEGF-TKIs in our study, showing a significant survival advantage. This finding corroborates previous studies in particular in papillary RCC, such as the PAPMET trial, 8 suggesting that cabozantinib should be preferred over other TKIs for first-line treatment, especially when ICI combinations are contraindicated.
Despite these interesting results, our study has several limitations inherent to its retrospective and non-randomized design. The lack of centralized pathological and radiological review, the relatively small sample size, and the incomplete availability of some clinically relevant variables, such as IMDC score (that may have affected the multivariable analyses) reflect the intrinsic challenges of studying rare and heterogeneous diseases like non-clear cell renal cell carcinoma.
In addition, treatment allocation was not randomized and may have been influenced by confounding by indication. Patients selected for ICI-based combinations may have differed from those receiving VEGF-TKI monotherapy in terms of clinical characteristics, disease burden, or access to newer therapies. A potential temporal (era) effect cannot be excluded, as ICI-based combinations were more frequently administered in more recent years. Although multivariable analyses were performed to adjust for known prognostic factors, residual confounding may persist. Therefore, the observed associations should be interpreted as hypothesis-generating rather than as evidence of causality.
Finally, the biological and clinical heterogeneity of nccRCC subtypes further limits the generalizability of these findings across all histologies.
Conclusion
Our study underscores that immunotherapy combinations (ICI plus ICI or ICI plus VEGF-TKI) appear to be more effective than other therapeutic options for metastatic nccRCC as first-line therapy, as previously suggested by prospective phase II single-arm trials; moreover, our data confirmed that cabozantinib may be a good option when ICI based therapy is contraindicated.
Furthermore, it provides a comprehensive descriptive evaluation and identification of potential prognostic factors in this setting, highlighting that the IMDC score remains a reliable prognostic factor even in nccRCC, including in contemporary cohorts like ours which includes patients treated with ICI-combinations.
These findings contribute valuable real-world evidence and underscore the need for prospective multicentric studies to establish standardized treatment protocols for this diverse group of tumors. The collaborative effort of pooling data from multiple centers, including those from different countries, is essential to improve our understanding and management of nccRCC.
Supplemental Material
sj-docx-1-tmj-10.1177_03008916261436580 – Supplemental material for International multicenter experience of prognostic factors and treatment outcomes of metastatic non-clear cell renal cell carcinoma
Supplemental material, sj-docx-1-tmj-10.1177_03008916261436580 for International multicenter experience of prognostic factors and treatment outcomes of metastatic non-clear cell renal cell carcinoma by Alessandro Rametta, Sebastiano Buti, Marco Stellato, Marco Maruzzo, Luca Lalli, Alessandro Acunzo, Michele Maffezzoli, Davide Bimbatti, Francesco Pierantoni, Francesco Massari, Paola Ermacora, Roberto Iacovelli, Alessia Mennitto, Claudia Mucciarini, Matteo Santoni, Lucia Fratino, Rafael Morales, David Marmolejo, Laia Catalan, Cristina Suarez and Giuseppe Procopio in Tumori Journal
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.