
Abstract
Objectives:
Concurrence of pregnancy and cancer diagnosis is increasingly frequent in Italy. The study aimed to compare women with pregnancy-associated cancers (PACs) to those of childbearing age, focusing on fertility, induced abortion, and miscarriage.
Methods:
The population-based study included women aged 15-49 years, both with and without PAC, who were residents in the area covered by the 19 participating Cancer Registries between 2003 and 2015 and identified by individual deterministic linkage with the Hospital Discharge Database.
Results:
Overall, 2,218,139 obstetrics hospitalizations occurred, covering delivery (75%), induced abortion (14%), and miscarriage (11%). Among 2409 women with PAC, 69% gave birth, 16% had an induced abortion and 15% a miscarriage. Compared with the reference population, the fertility rate in women with PACs was steadily lower (mean values 25.7/1000 vs 37.7/1000), while induced abortion (from 359/1000 - SRR 1.99, 95%CI 1.32-3.00 - in 2003 to 147/1000 - SRR 1.11, 95%CI 0.59-2.09 - in 2015) and miscarriage ratios exhibited a decreasing trend.
Conclusion:
These results are consistent with international literature and are probably due to advancements in diagnostic and therapeutic opportunities. This is the first Italian population-based study analysing fertility and pregnancy outcomes among women with PAC based on a reliable information on cancer diagnosis.
Keywords
Introduction
Pregnancy-associated cancer (PAC) refers to cancer identified either during pregnancy or within one year of childbirth.1 -3 The simultaneous occurrence of cancer and pregnancy presents a significant challenge for clinicians, who must prioritize the well-being of both the mother and fetus, as well as for epidemiologists who aim to accurately quantify its frequency.
Although PAC is infrequent, with an incidence of approximately 1 in 1000 pregnancies,4,5 accounting for 0.07%-0.1% of all malignant tumours, 6 its occurrence has increased in recent decades. 7 This rise is partly attributable to the global trend of increasing maternal age.2,8 In Italy, where the average age at delivery has risen considerably over the past 20 years, 8 making it one of the European countries with the highest maternal age, a recent population-based study estimated a PAC incidence rate of 1.24 per 1000 pregnancies. 9
Breast cancer is the most frequently diagnosed malignancy during pregnancy, followed by malignancies of the thyroid and other endocrine glands, melanoma, female genital organs, and digestive organs. 9 The frequency distribution by site mirrors that of the general female population of childbearing age. 10
Although a cancer diagnosis may affect fertility rates, 11 advancement in early detection, effective therapies, the ability to preserve gametes and access to assisted reproductive technologies have become significant aspects for couples desiring pregnancy. While systemic chemotherapy and some radiotherapies pose a higher risk of miscarriage and congenital malformations, other cancer treatments are feasible during pregnancy.4,12-13 On the contrary, when the oncological condition does not represent an immediate threat to life, pregnancy can be ended, and the start of chemotherapy postponed. The diagnosis of cancer may impact not only the risk of miscarriage but also decisions regarding pregnancy termination, which can be influenced by social and psychological factors.
Despite this, there is a lack of comprehensive epidemiological studies addressing fecundity and abortion in women with PAC and those of reproductive age.
The present study aims to investigate whether the reproductive outcomes (delivery, miscarriage, and induced abortion) in women with PAC are comparable to those of women of childbearing age. The study also explores how these trends may have changed over time alongside advancements in the clinical management of tumors during pregnancy.
Materials and methods
This longitudinal retrospective population-based study collected cases of cancers that occurred between 2003 and 2015 from 19 Italian Cancer Registries (CRs), located in Northern (n=8), Central (n=2), and Southern (n=9) Italy and covering about 22.0 % of the Italian population (Online Supplementary Table A). Only cancer registries capable of providing cases for a continuous period of five years were included in the analysis. Benign, uncertain, and non-melanoma skin cancers were excluded from the study analysis.
Cases of cancer in women aged 15-49 years during the study period were identified by the participating CRs, according to the ICDO-3 classification. These cases were linked to obstetric hospitalization codes, selected through the Hospital Discharge Database (HDD), and grouped by pregnancy outcomes (Online Supplementary Table B) according to the International Classification of Diseases, 9th revision, Clinical Modification (ICD9-CM)). In the present study, we define as PAC the women with a cancer diagnosis:
a) giving birth between nine months before and 12 months after a cancer diagnosis,
b) having a miscarriage or an induced abortion between three months before and 12 months after.
The reference population included all women aged 15-49 years, residents in the areas covered by the participating CRs and hospitalized for delivery, induced abortion, or miscarriage during the study period. 9
In case of multiple hospitalizations of the same woman occurring within a time interval of less than six months, she was counted once. In the case of multiple cancers, the earliest diagnosis was used in the analyses. The PAC proportion was calculated by pregnancy outcome (delivery, miscarriage, and induced abortion) and stratified by age, citizenship, and area of residence. The chi-square test estimated the difference in proportion at 95% level.
To compare the fertility of women with PAC to the reference population, fertility rates were calculated for both groups as the number of deliveries by 1000 resident women aged 15-49 years. The rates were standardized using the direct method, with the reference population being Italian women in five-year age groups based on the 2011 ISTAT census. 14 For calculating the fertility rate, the number of live births was estimated based on the number of deliveries recorded in the National HDD.
The induced abortion and miscarriage ratios were calculated as the number of induced abortions or miscarriages/deliveries per 1000. These indicators were also standardized using the direct method, with the reference population being Italian women who gave birth in Italy in 2015 by four age groups (<25, 25-34, 35-39, ⩾40), as reported by Euro-Peristat. 8 The age-standardized relative risks (SRR) of induced abortion and miscarriage were estimated by calendar years using the STDRATE Procedure 15 of Statistical Analysis System Software (SAS version 9.4), the 95% confidence intervals (CIs) were calculated assuming the log-normal distribution. Sensitivity analyses were run limiting the analysis to PAC with reproductive outcomes occurring after the cancer diagnosis. The present study was coordinated by the Istituto Superiore di Sanità (Italian National Institute of Health – ISS) in collaboration with the Italian Society of Gynaecology and Obstetrics (SIGO) and the Italian Association of Cancer Registries (AIRTUM).
Results
During the study period in the areas of the participating CRs, there were 2,218,139 hospitalizations for deliveries (74.9%), induced abortions (14.0%), and miscarriages (11.1%) among women aged 15-49 years. Among those women, 2409 PAC were identified: 1660 (68.9%) gave birth between nine months before and 12 months after a cancer diagnosis, 393 (16.3%) and 356 (14.8%) had respectively an induced abortion and a miscarriage between three months before and 12 months after a cancer diagnosis (Table 1).
Characteristics of women with pregnancy-associated cancer (PAC) compared with the reference population. Women aged 15-49 resident in the participating Italian Cancer Registries hospitalized for delivery, induced abortion, or miscarriage between 2003 and 2015.
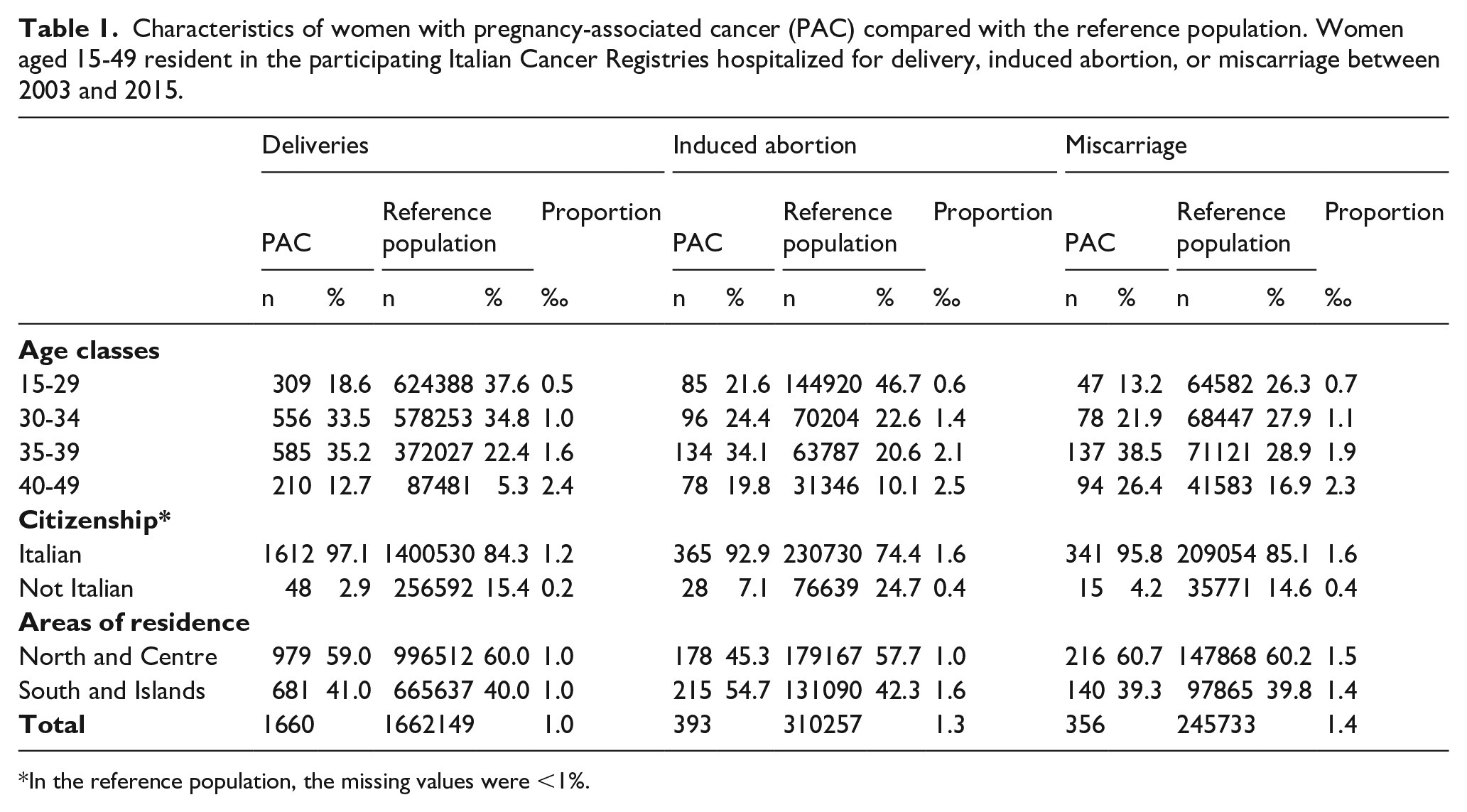
In the reference population, the missing values were <1%.
The PAC proportion was slightly lower in pregnancies that ended with a delivery (1.0 per 1000 pregnancies) than in pregnancies that ended in induced abortion (1.3/1000) or miscarriage (1.4/1000).
For all pregnancy outcomes, the proportion of women aged 35 years or older was higher in PAC than in reference population (47.9% vs 27.6% for deliveries, 53.9% vs 30.7% for induced abortion, and 64.9% vs 45.8% for miscarriage) (Table 1).
Comparing women’s citizenship, among PAC, the proportion of foreign women who gave birth was less than half of those who opted for an induced abortion (2.9% vs 7.1%).
Looking at the areas of the participating CRs, there were no differences in the percentage of deliveries in the reference population and PAC between Northern and Central Italy and the South and Islands (around 60% vs 40% in both groups), with a PAC proportion of 1/1000 in both areas. In the South, the proportion of induced abortions in PAC was higher compared to the North (54.7% vs 45.3% p-value<0.001), whereas in the reference population, this proportion was reversed (42.3% vs 57.7% <0.001).
During the study period, the standardized fertility rate in the reference population was higher than that of PAC, with an average of 37.7/1000 deliveries and 25.8/1000 deliveries, respectively (Figure 1). During the examined years, the PAC proportion for the three pregnancy outcomes showed no substantial differences between different geographic areas of residence or women’s citizenship (data not shown).
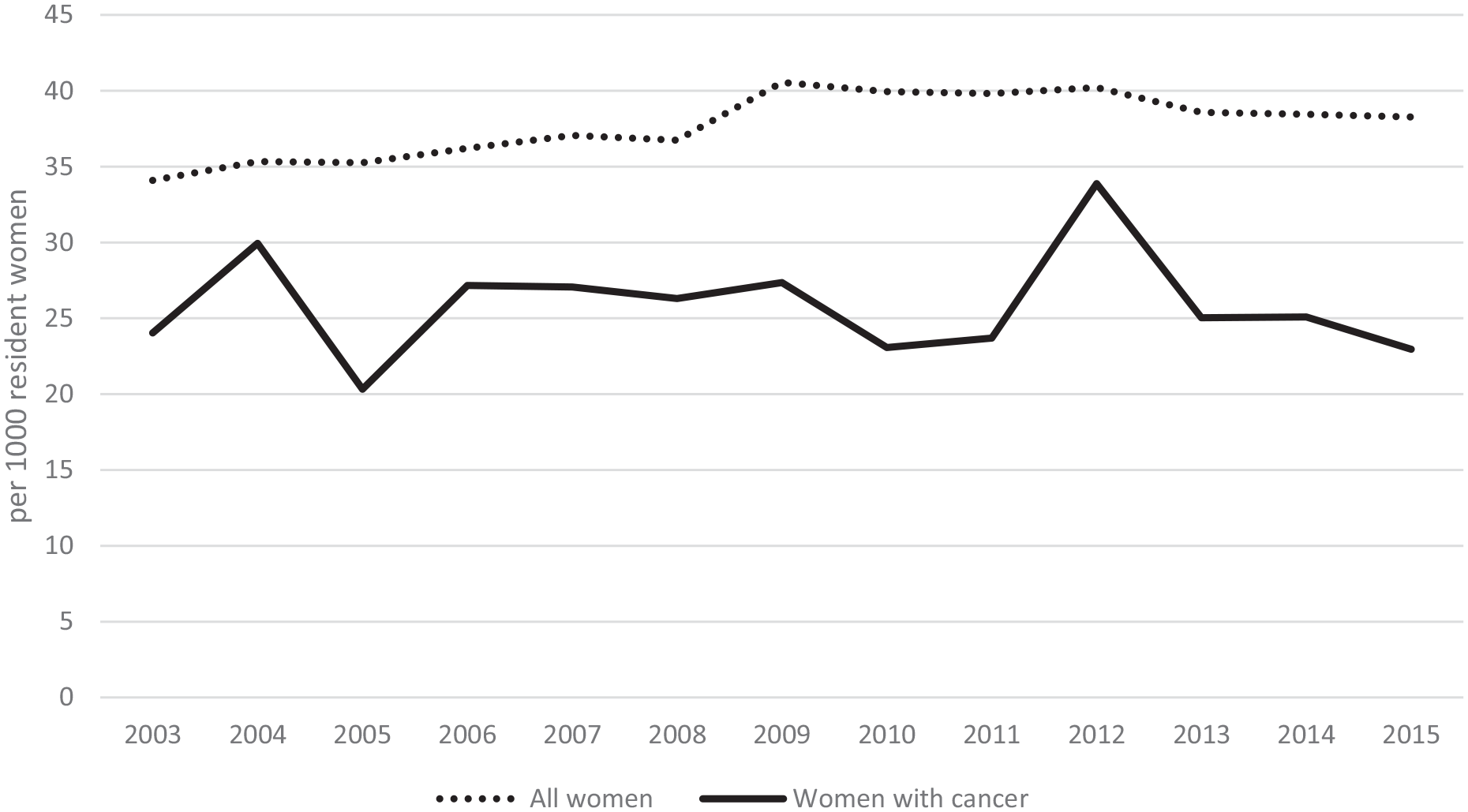
Standardized fertility rate in the reference population and women with pregnancy-associated cancer. Women aged 15-49 resident in the participating Italian Cancer Registries between 2003 and 2015. For the calculation of fertility rate, the number of live births was approximated using the number of deliveries.
Between 2003 and 2010, the induced abortion ratio among PACs was higher compared to that of the reference population (Figure 2). In this period, a fluctuating and decreasing trend can be observed in women with cancer. From 2011 to 2015, the induced abortion ratio almost overlaps with the one of the reference population, with SRRs no longer statistically significant confirming this trend (Figure 2 and Online Supplementary Table C).
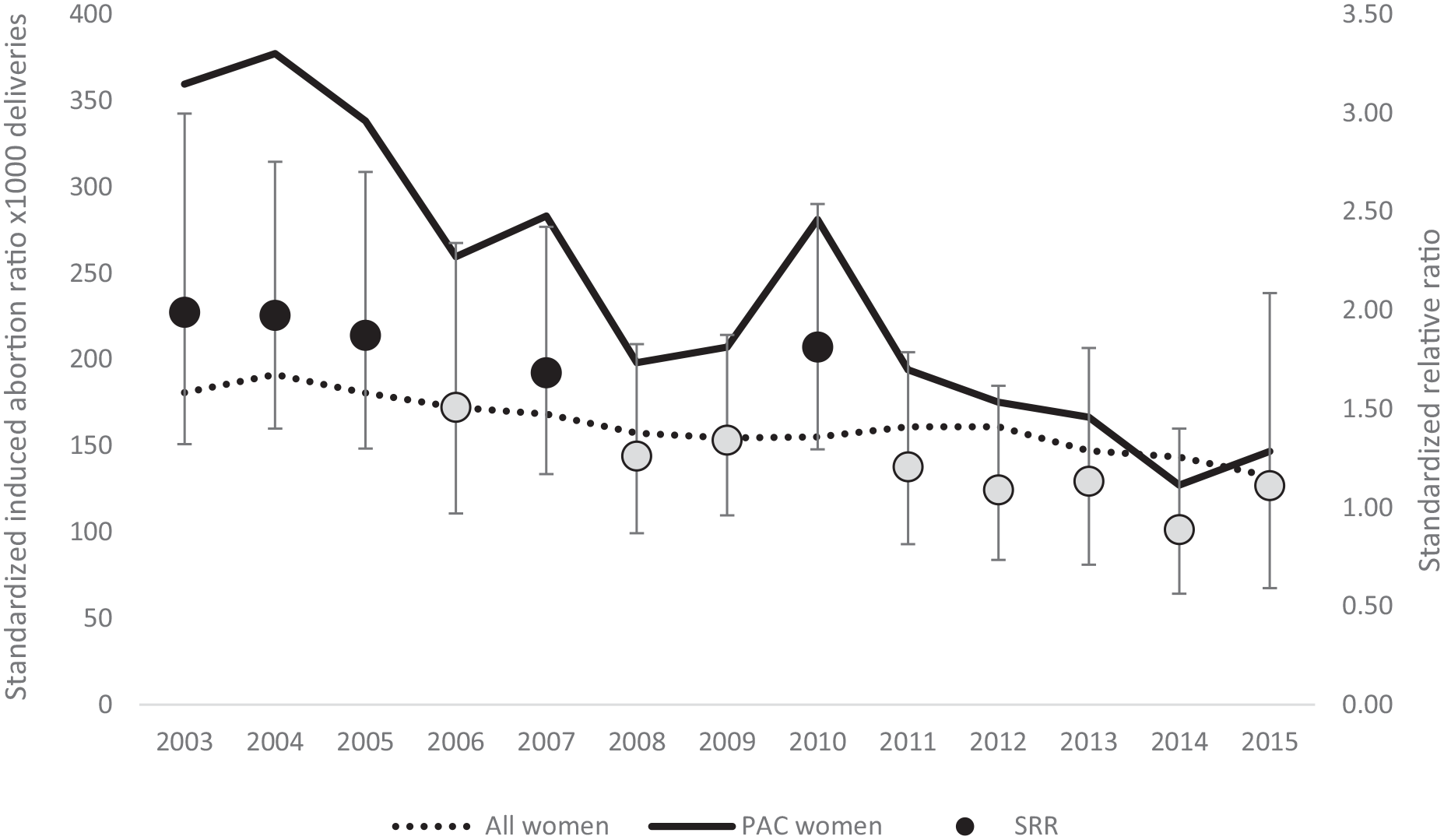
Standardized induced abortion ratio in the reference population and women with pregnancy-associated cancer. Women aged 15-49 resident in the participating Italian Cancer Registries between 2003 and 2015.
The trend of miscarriage ratio was quite stable over time in the reference population while exhibiting variability among women with cancer (Figure 3). Except for 2004 and 2011, it was higher in PAC. The SRRs were never statistically significant, except for 2014 when the gap between the two groups increased considerably (SRR 1.85, 95%CI 1.33-2.57) (Online Supplementary Table C). Overall, both the induced abortion and miscarriage ratios were significantly higher, respectively 1.34 (95%CI 1.20-1.49) and 1.16 (95%CI 1.04-1.30).
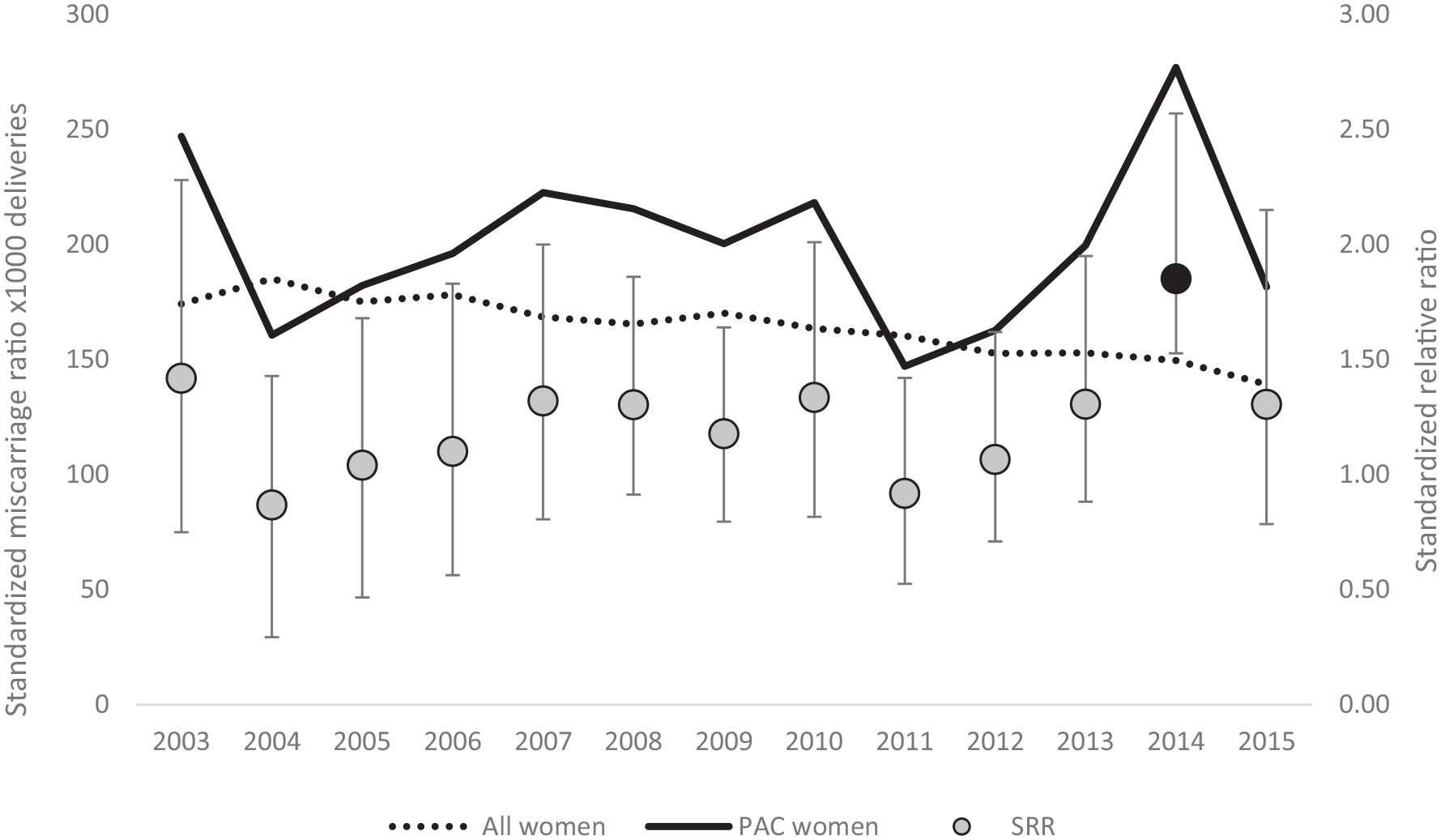
Standardized miscarriage ratio in the reference population (line x) and women with pregnancy-associated cancer (line y). Women aged 15-49 resident in the participating Italian Cancer Registries between 2003 and 2015.
Sensitivity analyses
By limiting the analysis to PAC with reproductive outcomes occurring after the cancer diagnosis, we identified 1385 cases: 72.0% gave birth, 17.4% had an induced abortion, and 10.6% a miscarriage. The results of the sensitivity analyses did not differ significantly from those of the main analysis.
Discussion
The present study was designed to gather evidence about the trend of fertility and abortion in women with PAC. Between 2003 and 2015, the standardized fertility rate in women with cancer was constantly lower than the one of the reference population of women aged 15-49 years (mean value of 25.8/1000 deliveries vs 37.7/1000). However, deliveries represented the most frequent pregnancy outcome (68.9%) among both women with PAC (68.9%) and the reference population (74.9%). The induced abortion ratio in women with PAC decreased consistently and continuously during the study period until it showed a trend comparable to that of the reference population.
Compared to the extensive data available for non-pregnant cancer patients, there is limited evidence-based information concerning diagnostic and treatment strategies for pregnant women with cancer.16-17 However, emerging insights and evidence-based knowledge, alongside numerous international expert consensus meetings, have facilitated the development of a more standardized approach aimed at ensuring better outcomes for both mother and child.16 -18 As a result, nowadays, cancer therapy can be prioritized over the termination of pregnancy, leading to an increasing number of live births over time. 19 Analysing the results of the present study, consistent with other papers,12,20-21 it can be speculated that increased awareness regarding the effectiveness of cancer therapy during pregnancy has instilled greater confidence in clinicians and couples to proceed with the pregnancy.
Madanat et al. studied the probability of parenthood after a cancer diagnosis in a Finnish cohort of around twenty-five thousand cancer survivors and their siblings. 22 The relative probability of parenthood following early onset cancer for women aged 20-34 years was significantly reduced by around 60% but increased over calendar years. This difference, although to a lesser extent, is confirmed by a Norwegian registry-based study, 23 in which the first-time parenthood probability at the age of 35 years in female patients was statistically lower compared to the probability in the general population (66% vs 79%).
Although the mean age at delivery has increased in the general population, in the present study the proportion of women aged ⩾35 was higher among women with PAC than in the whole cohort, in line with other studies.1,2 This is partly due to the aging of pregnant women and the improvement of modern medicine in cancer early diagnosis and treatment even during pregnancy.
The association between PAC and induced abortion is poorly studied. In our study, the standardized induced abortion ratio in women with cancer was higher than the one of the reference population (1.34, 95%CI 1.20-1.49) but showed a constant decreasing trend until it converged with that of the general population in the final years of observation. Similar results were obtained from one of the most recent population-based studies conducted in Lombardy Region (Italy), 12 where, between 2010 and 2020, a slight increase in the proportion of births among women with PAC was observed alongside a reduction in the risk of induced abortions among those women compared to the general population, from 1.08 (95%CI 0.92-1.26) in 2010-2012 to 0.87 (95%CI 0.65-1.17) in 2019–2020.
In our study, women with PAC living in Southern Italy showed higher proportions of induced abortions compared to those in the Central-Northern regions (PAC proportion of 1.6 per 100,000 and 1.0 per 100,000, respectively). This finding is consistent with those by Esposito et al. 12 However, no statistically significant differences were found when analysing trends between these geographical areas. Conversely, in the general population, the trend is reversed with the surveillance system for legal induced abortions reporting lower rates in the South compared to the Central-North. These results may be read as lower awareness and access to diagnostic and therapeutic opportunities that could ensure the continuation of their pregnancy among women in the South of the country.
The fluctuating trend of miscarriages is challenging to interpret, as many events occur outside hospitals particularly in cases of early miscarriages or when they occur in younger women. 24 Hospital access for miscarriage management may differ between the general female population and women with cancer, who may adopt a more conservative approach and tend to have a higher rate of hospitalization compared to the general population, making the HDD inadequate for this analysis. However, pregnant women with cancer have shown an increased risk of miscarriage, with a risk ratio of 1.16 (95%CI 1.04-1.30). The timing of the cancer diagnosis, particularly if it occurs early in pregnancy, can influence pregnancy outcomes and may heighten the risk of miscarriage. Administering chemotherapy is contraindicated during the first trimester because of an increased risk of miscarriage and significant teratogenic effect since organ development primarily happens during this period. 19
To the authors’ knowledge, this is one of the largest population-based studies, covering 22% of the Italian population living in the North, Centre, and South of the country. Moreover, the record linkage between Cancer Registries and the Hospital Discharge Database guarantees a higher degree of precision and completeness in case identification, providing more reliable information compared with studies relying solely on administrative health data. Finally, the adopted definition of PAC allows comparability with other studies.
The main limitation of the study is the heterogeneity of the data updates sent from the various cancer registries, with a delay of approximately three years. Another limitation is the lack of data about maternal characteristics and perinatal outcomes, such as malformations that would allow a more in-depth analysis of fertility and abortion trends to better guide the decisions of couples and clinicians. The use of HDD to identify reproductive outcomes certainly posed additional limitations: the parity of the woman, which could influence pregnancy outcomes, as well as the cancer diagnosis, is unknown. For instance, a prior breastfeeding experience may have positively impacted the prognosis of breast cancer. 25 Additionally, the lack of data on gestational age prevents us from determining the timing of conception and the specific pregnancy trimesters, making it challenging to accurately define the time window for assessing the overlap between cancer and pregnancy events.
During the 12-year observation period of the study, there was a progressive reduction of induced abortion in women with cancer, suggesting a progressive improvement in the management and treatment of PAC. Detection of early stage indolent cancers and a better understanding of chemotherapy options may have played a role in the observed decline. 19 Through the linkage with the Birth Registry, gestational age at delivery could also be known a crucial piece of information in assessing the perinatal care provided, given the significant impact of preterm birth, even in high-income countries.8,26 -28
Given the high variability in cancer management and available treatments in different countries, the results of the present study cannot be generalized to low-income countries.
Conclusions
The results of the present study are quite novel in the scientific literature, since the topic of fertility in women with cancer remains minimally explored. The reduction in induced abortions and increase in deliveries among women with cancer can be looked upon with optimism by both clinicians involved in the childbirth care and couples wishing to have children. More timely and accurate diagnosis, along with the availability of treatments that can increasingly be administered during pregnancy, represent significant steps forward in improving the quality of life for women with PAC.
We hope that this study will stimulate researchers to explore this topic further, by integrating reliable information from the various health care administrative data such as the Birth Registry. This would also allow analysis of perinatal outcomes, including mode of delivery, gestational age at birth, and maternal and neonatal outcomes.
Supplemental Material
sj-pdf-1-tmj-10.1177_03008916241298810 – Supplemental material for Fertility and abortion: A population-based comparison between women with cancer and those in childbearing age
Supplemental material, sj-pdf-1-tmj-10.1177_03008916241298810 for Fertility and abortion: A population-based comparison between women with cancer and those in childbearing age by Alice Maraschini, Edoardo Corsi Decenti, Serena Donati, Silvia Francisci, Tania Lopez, Rosalba Amodio, Fortunato Bianconi, Emanuela Bovo, Rossella Bruni, Marine Castaing, Claudia Cirilli, Rosa Pasqualina De Vincenzo, Giuseppe Furgiuele, Linda Guarda, Silvia Iacovacci, Lucia Mangone, Walter Mazzucco, Anna Melcarne, Elisabetta Merlo, Michael Mian, Giuseppe Sampietro, Giovanni Scambia, Tiziana Scuderi, Ausilia Sferrazza, Fabrizio Stracci, Antonina Torrisi, Vito Trojano, Maria Francesca Vitale and Daniela Pierannunzio in Tumori Journal
Footnotes
Author contributions
Conceptualization: A.Ma., E.C.D., S.D., S.F., T.L. and D.P. Data curation: R.A., F.B., E.B., R.B., M.C., C.C., G.F, L.G., S.I., L.M, A.Me., E.M., M.M., W.M., G.Sa., T.S., A.S., F.S., A.T. and M.F.V. Formal analysis: A.Ma. and D.P. Funding acquisition: D.P. Methodology: A.Ma., E.C.D. and D.P. Validation: R.A., F.B., E.B., R.B., M.C., C.C., R.P.D.V, G.F., L.G., S.I., L.M., A.Me., E.M., M.M., W.M., G.Sa., G.Sc., T.S., A.S., F.S., A.T., V.T. and M.F.V. Writing – Original draft: A.Ma., E.C.D., S.D., S.F., T.L. and D.P. Writing – Review & editing: A.Ma., E.C.D., S.D., S.F., T.L. and D.P.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Italian National Institute of Health (Bando Ricerca Indipendente ISS 2020–2022), project code ISS20-a4627f16ba39.
Institutional Review Board
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Italian National Institute of Health (Protocol code AOO-ISS 0028471, 26 September 2018).
Informed consent
The Italian legislation identifies regional and national health authorities as collectors of personal data for surveillance purposes without explicit individual consent. This study is a descriptive analysis of anonymous aggregate data without any direct or indirect intervention on patients (Decreto del Presidente del Consiglio dei Ministri, 3 March 2017, Identificazione dei sistemi di sorveglianza e dei registri di mortalità, di tumori e di altre patologie, 17A03142, GU Serie Generale n.109 del 12-05-2017). Available at:![]() (accessed on 9 March 2023).
(accessed on 9 March 2023).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.