
Abstract
Objective:
To describe the practice of prostate-specific antigen (PSA) testing over more than 20 years in Friuli Venezia Giulia (FVG), North-Eastern Italy.
Methods:
A population-based, ecological study was conducted using information derived from regional administrative health-related databases. Data on PSA and prostate biopsies performed on resident men aged ⩾45 years from 1998 to 2019 were retrieved. PSA and biopsy rates were calculated as the number of men who had at least one such procedure in each calendar year over the mean resident male population of the same year. Temporal trends were analyzed using joinpoint regression (annual percentage change –APC).
Results:
A total of 2,502,670 PSA were made between 1998 to 2019 in men aged ⩾45 years. The number of PSA steadily increased from 51,055 in 1998-1999 to 134,504 in 2010-2011, then dropped to 122,080 in 2018-2019. Significant changes in the slopes of PSA rates emerged in 2002 and 2009: the largest increase occurred during 1998-2002 (APC 18.4), followed by a smaller increase in 2002-2009 (APC 3.4) and a subsequent reduction (APC -2.5). Similar patterns emerged for all ages, but the decrease since 2009 was smaller for men aged ⩾65 years. An upward trend emerged in biopsy rate from 1998 to 2001 (APC 13.0), followed by a smaller increase until 2007 (APC 5.7) and a subsequent decrease. Biopsies as percentage of PSA decreased from 3.2% to 2.2%, particularly in those aged ⩾75 years.
Conclusions:
Although overall declining PSA rates have been observed in FVG since 2009, rates remained higher in the ⩾65-year-old group than in the 45-64–year-old group.
Introduction
Prostate cancer (PCa) has been diagnosed in approximately 1.4 million men worldwide according to 2020 GLOBOCAN estimates. 1 The incidence of PCa varies widely across countries (age-standardized rate, ASR, from 6.3 to 83.4 per 100,000 men), with the highest rates found in Northern and Western Europe, Australia/New Zealand, and Northern America, and the lowest rates in Asia and Northern Africa. 1 Differences in PCa diagnostic procedures, including the use of prostate-specific antigen (PSA) test, are thought to be the greatest contributor to these geographic variations. 2
Screening for PCa by PSA remains a controversial issue, as the extent to which it can decrease PCa mortality is unclear.3,4 In this regard, the major randomized trials have reported contrasting effects of PSA screening on PCa mortality. In particular, the European Randomized Study of Screening for Prostate Cancer (ERSPC) provided level 1 evidence that PSA screening leads to a 20% relative risk reduction in PCa-specific mortality after 16 years of follow-up 5 and 30% of metastatic disease after 12 years. 6 On the other hand, the Prostate, Lung, Colon and Ovarian (PLCO) trial, involving over 75,000 men, reported no reduction in PCa deaths in the screening group after 13 years of follow-up. 7 Actually, even though PSA testing and subsequent treatments do contribute to the observed declining mortality, the harms-to-benefits ratio remains controversial because of adverse events. Indeed, PSA testing mainly facilitates the detection of indolent tumors, leading to the diagnosis of cases that would not have caused clinical consequences during a man’s lifetime (i.e., overdiagnosis) with subsequent overtreatment. 8
The body of evidence for the recommendations on PSA testing consists of well-known randomized and controlled medical trials data. Nevertheless, it remains largely unknown whether the use and treatments associated with PSA and diagnosis of PCa are inappropriately high, particularly among the older age groups. The 2013 update of the European Association of Urology (EAU) guidelines did not endorse mass screening for PCa, and recommended screening only in men with a >10 years life expectancy (irrespective of age) after a baseline PSA determination at 40-45 years of age. 9 Since 2008, the US Preventive Services Task Force (USPSTF) had already recommended against mass screening for PCa and further lowered, in 2018, the upper threshold from 75 to 70 years of age.10,11 The last USPSTF guidelines also demand that PSA testing among men aged between 55 and 69 years is preceded by an informed and shared decision-making process with the potential patient. 11
In Italy, the incidence of PCa started to rise in the late 1980s, reaching the highest incidence rates in 2003-2005. 12 Thereafter, incidence rates slightly declined,13,14 a pattern mostly attributable to the widespread introduction of PSA testing. Opportunistic PSA screening has been increasing in Italy since the 1990s, most markedly in the North of the country. 15 While PCa incidence rates increased rapidly during the 1990s, mortality rates changed only modestly, with a tendency to decline since 1999.14,15 Population-based studies describing changes over time of PSA testing in Italy are scarce and recent trends have not yet been reported.16-18
This study aims to evaluate the practice of PSA testing over more than 20-years in the male population of the Friuli Venezia Giulia region, North-Eastern Italy, overall and by age groups. PSA trends were also explored along with prostate biopsy ones.
Materials and methods
A population-based, ecological study was conducted using information derived from the regional administrative health-related databases of the Friuli Venezia Giulia, a region in North-Eastern Italy populated by approximately 1,200,000 inhabitants.
Data on PSA testing, including total and free PSA, and prostate biopsies were extracted from the outpatient services database, which collects all diagnostic procedures performed in regional hospitals since 1998. Data on PSA testing and biopsy use include the anonymous unique identifier (randomly assigned to each male resident, and which changes every six months to guarantee the anonymity of individuals), the date of the procedure, and other characteristics, but not the results (i.e., PSA levels or biopsy outcome). For each individual, only one procedure of PSA testing and prostate biopsy per year were counted. The assignment to age groups was based on the age at the first procedure of the year.
PCa cases were identified using the population-based Cancer Registry of Friuli Venezia Giulia, which since 1995 collects data on all new cases of cancer occurring among the population living in the region. The study did not include PCa cases in non-resident men and any cancer diagnoses identified at autopsy only.
To guarantee the highest completeness and accuracy of the information, data from the above-cited databases were limited to the concurrently available period, i.e., 1998–2019.
For the purpose of this analysis, only PSA tests and biopsies performed on resident men aged ⩾45 years were considered (see Supplementary Table 1). The following indicators were computed: (i) the PSA testing rate, calculated as the number of men tested at least once per year in each included calendar year divided by the mean resident male population in the same year (derived from public data of the Italian National Institute of Statistics, ISTAT); (ii) the biopsy rate, calculated as the number of men who underwent prostate biopsy in each calendar year divided by the mean resident male population in the same year (derived from ISTAT); and (iii) the percentage of men undergoing prostate biopsy over men tested with PSA in each calendar year.
Time trends were explored using joinpoint regression analysis in order to detect time points where significant changes had possibly occurred. Annual percent change (APC) estimates and 95% confidence intervals (CIs) were obtained by fitting a linear regression line to the natural logarithm of annual rates using the calendar year as a regressor. This calculation assumes that the rates changed at a constant rate over the entire calendar-year interval observed.
Results
A total of 2,502,670 PSA tests were made during the study period in men aged ⩾45 years. The number of PSA testing steadily increased in all age groups and overall, i.e., from 51,055 in 1998-1999 to 134,504 in 2010-2011, and then dropped to 122,080 in 2018-2019 (Supplementary Table 1).
Figure 1 shows the trends in rates of men tested with PSA and men who underwent prostate biopsy (calculated as the number of men who underwent at least one such procedure in each included year over the mean resident male population of the same year), as well as the corresponding trend in PCa incidence. Joinpoint analysis showed statistically significant changes in the slopes of PSA rates in 2002 and in 2009, highlighting a sharp increase of rates in 1998-2002 (from 13,990 to 27,405 per 100,000 men-year; APC 18.4, 95% CI: 13.3 to 23.7) that was followed by a smaller increase in 2002-2009 (from 27,405 to 35,019 per 100,000 men-year; APC 3.4, 95% CI: 1.7 to 5.2), and a subsequent reduction (from 35,019 to 28,498 per 100,000 men-year; APC -2.5, 95% CI: -3.3 to -1.8).
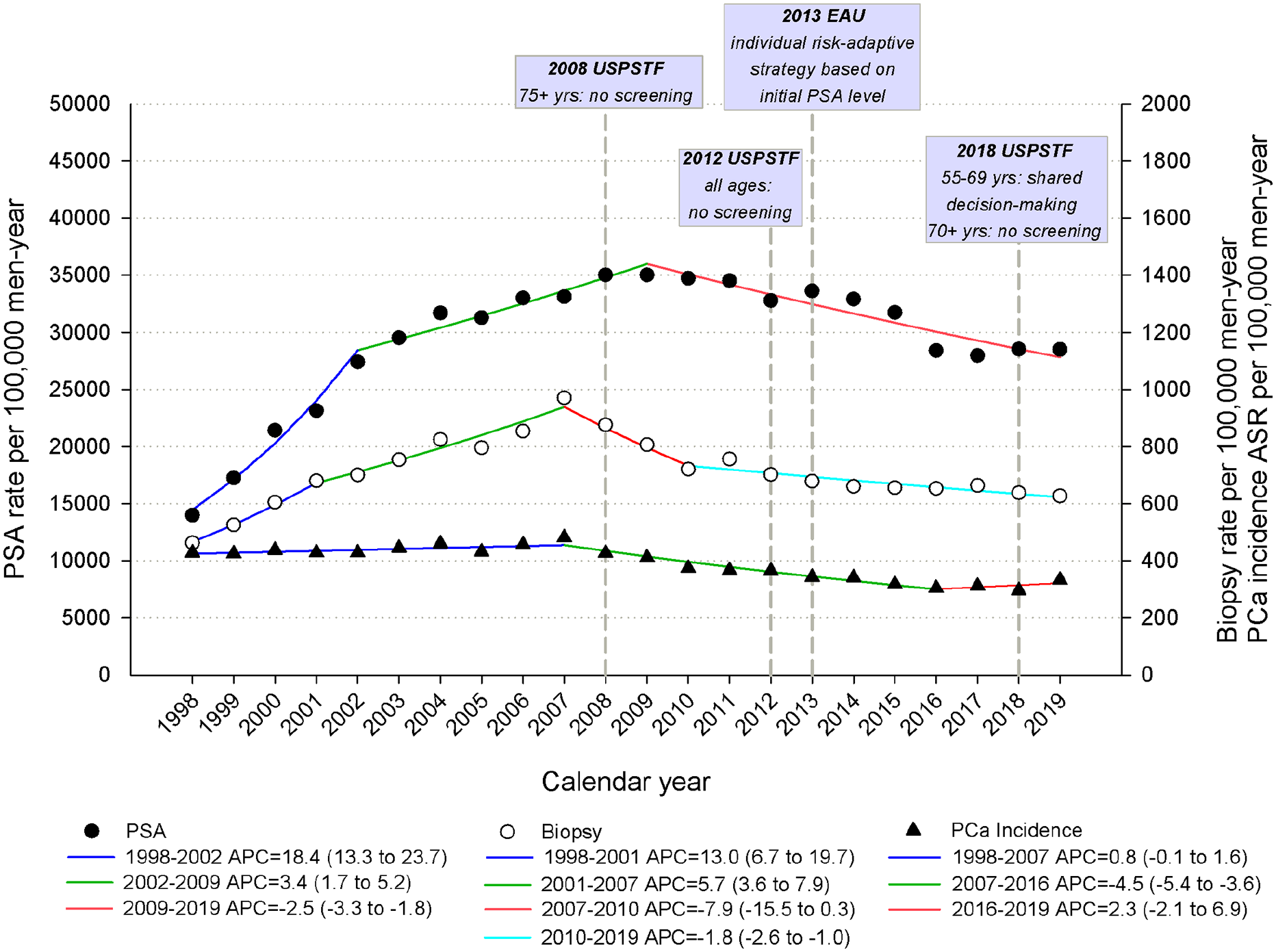
Trends in rates of men tested with PSAa per 100,000 men-year (left scale), rates of men who underwent prostate biopsya per 100,000 men-year (right scale), and age-standardized rates (ASR)b of prostate cancer (PCa) incidence per 100,000 men-year (right scale) in men aged ⩾45 years and corresponding joinpoint analyses. Friuli Venezia Giulia, Italy, 1998-2019.
The age group analysis of PSA trends revealed similar patterns in the 45-54 and 55-64 years groups, with an initial spike up to 2002 (APC 24.6, 95% CI: 16.6 to 33.2 and APC 20.5, 95% CI: 14.7 to 26.6, respectively), a second period of leveling off or lower increase up to 2009 (APC 2.5, 95% CI: -0.1 to 5.1 and APC 2.9, 95% CI: 1.0 to 4.9), and a third period of declining rates (APC -4.8, 95% CI: -6.0 to -3.7 and APC -4.7, 95% CI: -5.6 to -3.8) (Figure 2). Among men aged 65-74 and ⩾75 years, PSA rate steeply increased up to 2003 (APC 12.6, 95% CI: 9.8 to 15.5 and APC 12.3, 95% CI: 9.4 to 15.4, respectively), then it rose less markedly up to 2010-2011 (APC 2.5, 95% CI: 1.1 to 4.0 and APC 2.9, 95% CI: 1.7 to 4.2) before starting to slightly decrease (APC -1.9, 95% CI: -2.6 to -1.2 and APC -1.2, 95% CI: -2.0 to -0.3). The highest PSA rate was persistently among men aged 65-74 years, with values exceeding 50% since 2008 (Figure 2).
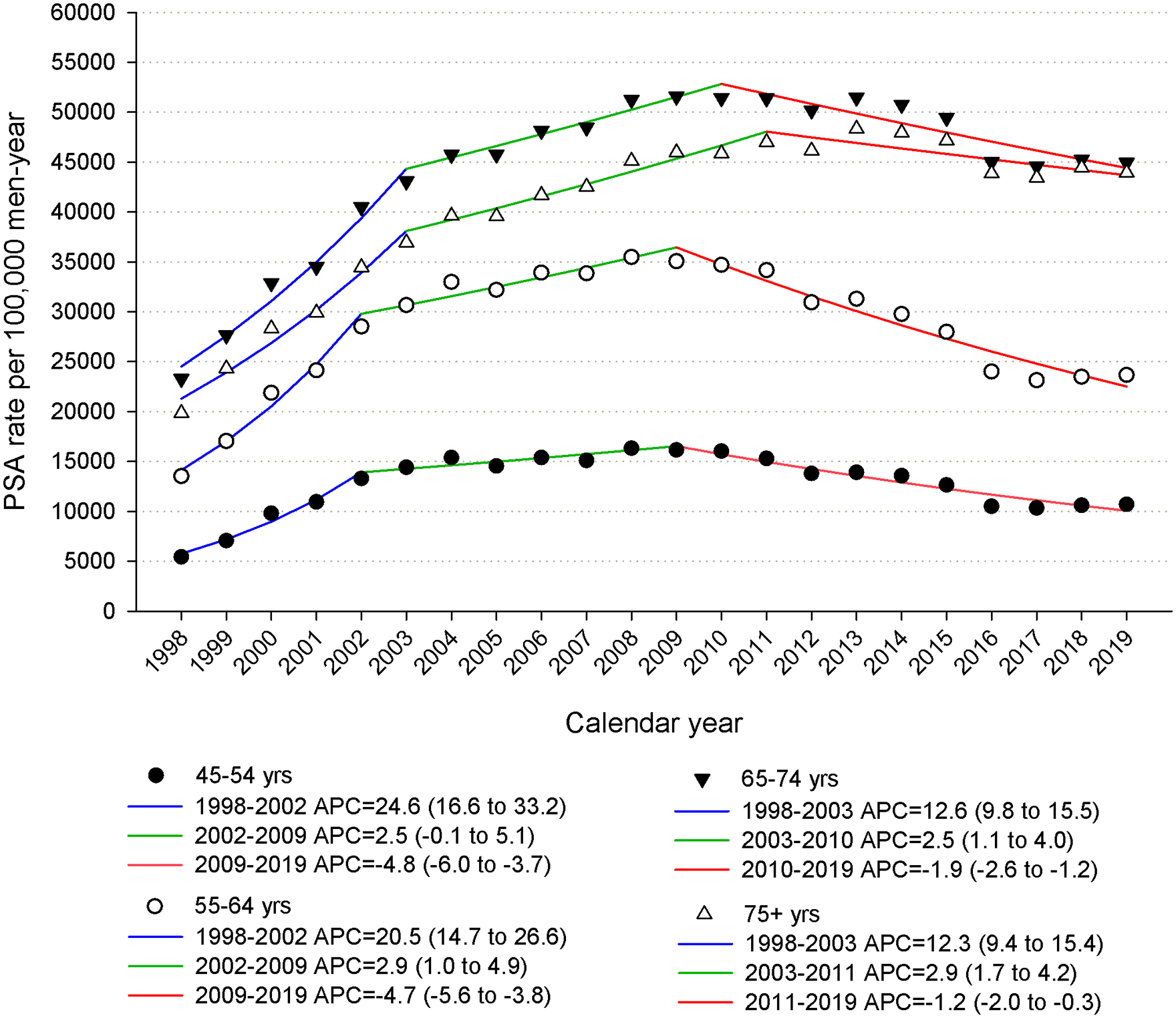
Trends in rates of men tested with PSAa per 100,000 men-year, by age, in men aged ⩾45 years and corresponding joinpoint analyses, Friuli Venezia Giulia, Italy, 1998-2019.
Joinpoint analysis identified three inflection points in prostate biopsy rates in 2001, 2007, and 2010 (Figure 1): rates increased from 463 per 100,000 men-year in 1998 to 680 per 100,000 men-year in 2001 (APC 13.0, 95% CI: 6.7 to 19.7), a further smaller increase emerged up to 2007, peaking at 970 per 100,000 men-year (APC 5.7, 95% CI: 3.6 to 7.9), after which the rates began to decrease (from 720 per 100,000 men-year in 2010 to 627 per 100,000 men-year in 2019; APC -1.8, 95% CI: -2.6 to -1.0).
Time variations in percentages of men undergoing prostate biopsy over men tested with PSA are shown in Figure 3. Overall, the percentage of biopsy/PSA testing decreased over the study period (from 3.2% in 1998-1999 down to 2.2% in 2018-2019) (Figure 3A). The decrease particularly involved men aged ⩾75 years, for whom the percentage dropped from 3.9% in 1998-1999 to 1.7% in 2018-2019 (Figure 3B). Biopsies as percentages of PSA were few in the youngest men (<1%) over the whole study period.
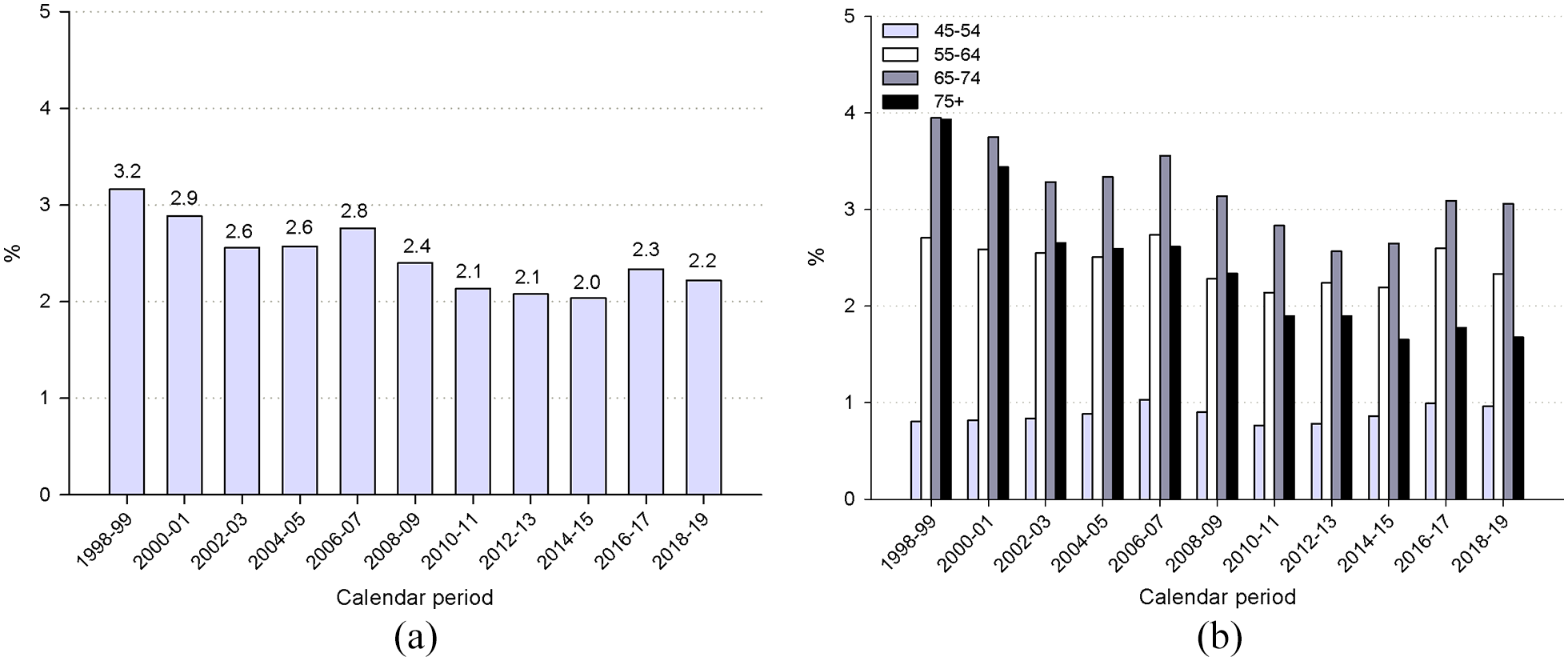
Trends in percentages of men aged ⩾45 years undergoing prostate biopsy over men tested with PSAa: overall (a) and by age group (b). Friuli Venezia Giulia, Italy, 1998-2019.
For comparison purposes, Figure 1 also shows the corresponding trend in PCa incidence among men aged ⩾45 years in Friuli Venezia Giulia, i.e., relatively stable rates from 1998 to 2007 (range 428-to-482 per 100,000 men-year), followed by a decline in 2007-2016 down to 304 per 100,000 men-year and a leveling off thereafter.
Discussion
This study provided a population-based evaluation of the use of PSA testing over more than 20 years among the male population of the Friuli Venezia Giulia region. Our findings showed that PSA testing use is rather diffused in this Italian area with a substantial proportion of men aged ⩾55 years (20-43%) undergoing PSA testing at least once a year in the 1998-2019 period. We found that the PSA rate (based on individuals who had at least one PSA in the considered year) increased up to 2009 and then declined afterward. This pattern was consistent across all ages, though the magnitude of the decrease from 2010-2011 onwards was smaller for men aged ⩾65 years than among those aged 45-64 years.
The percentage of men who were tested for PSA at least once per year concurs with the scanty data available from studies conducted in Italy in the 2000s. A survey conducted in 2002-2008 reported that 31-46% of men above the age of 50 years were tested for PSA. 16 Moreover, a study carried out in the Tuscany region over a 2-year period (2004-2005) reported a PSA screening frequency of 24% in men aged ⩾55 years. 17 To our knowledge, no other Italian investigation has recently evaluated PSA testing use.
The decrease in PSA testing rate in the most recent period is similar to that observed in the United States19-21 and Australia. 22 Contributing factors for these patterns may include changes in perception of the usefulness of PSA screening among providers and the general public following the 2008 USPSTF recommendations. Rather contradictory results from the publication of the PLCO and ERSPC trials in 2009 23 and the updates from the 2012 USPSTF and 2013 EAU guidelines may have also contributed to the downward trends in PSA. 19
The emphasis on the need for shared decision-making for PSA screening24,25 may also have impacted trends in rates of PSA-tested men, particularly among men below 65 years. However, there is no clear definition of the shared decision process and on its possible application in Italy and elsewhere. 26
The magnitude of the decrease in PSA rates among the oldest age group was small in Friuli Venezia Giulia, though most guidelines recommend against PSA-based screening for PCa in men ⩾75 years because of the harms of overdiagnosis and overtreatment.24,27,28 Indeed, men aged ⩾75 years represented almost one third of all men tested in the ⩾45 year group in 2018-2019 in our analysis, with rates that reached approximately 50% per year since 2008. One possible explanation for the high rates found among older men in this study is that they may undergo more regular medical checkups and, therefore, may be more willing to accept PSA screening. Moreover, physicians may be uncomfortable with estimating the life expectancy of patients, 29 which may contribute to a tendency for excessive screening in elderly men who have limited life expectancies. Further studies describing the management of older men with high PSA levels and the care of those diagnosed with PCa are needed to quantify whether overdiagnosis or overtreatment is occurring in this age group.
PSA testing rates among men aged 45-54 years were low, ranging from 5,451 to 16,329 per 100,000 men-year. The use of PSA in this age group is controversial, particularly before 50 years, except in high-risk groups (e.g., those with first-degree relatives having had PCa at a young age).9,24 In our analysis, men tested at age 45-49 represented 12-13% of all men tested in our study period.
Time changes in the rates of prostate biopsy in relation to PSA rates in our study are difficult to interpret due to the lack of individual information. Prior analyses have shown that rates of prostate biopsy and PCa incidence closely parallel rates of PSA testing, 30 whereas we found that the practice of taking a biopsy after PSA test became increasingly rare in the Friuli Venezia Giulia region. Our results may suggest that the prescription of a PSA test, normally made by family doctors, may not always be followed by the prescription or by the performance of a prostate biopsy, especially among the elderly. A reason potentially associated with the high levels of PSA testing could be that, in addition to its role in screening, PSA is also largely used to monitor patients on active surveillance for early PCa or to monitor the progression of the disease following treatment (e.g., surgery or radiotherapy).
Although our investigation does not allow firm conclusions about the impact of PSA testing on PCa detection, it is the first in Italy to provide recent population-based estimates of the frequency and trends of PSA testing use. The strengths of our study include its population-based design and the availability of data over 20 years in parallel with corresponding PCa incidence rates. The most important limitation is the lack of individual linkage between PSA testing outcome and the performance/outcome of a prostate biopsy. In addition, we had no access to information on the determinants of PSA testing, i.e. whether the decision was based on prostatic or urinary symptoms or if it was merely for screening purposes, and whether it was discussed between the doctor and the patient.
Conclusions
Our findings revealed a declining rate of men tested with PSA since 2009 in the Friuli Venezia Giulia region. Nevertheless, the magnitude of the decrease was smaller among men ⩾65 years than among those aged 45-64 years. To which extent abnormal PSA findings had been properly followed-up is also unclear. A more granular linkage study encompassing the whole spectrum of screening and triage for PCa in the population and in specific subgroups (i.e., the elderly with significant medical comorbidity) is warranted to assess adherence to evolving guidelines.
Supplemental Material
sj-pdf-1-tmj-10.1177_03008916221128343 – Supplemental material for The use of PSA testing over more than 20 years: A population-based study in North-Eastern Italy
Supplemental material, sj-pdf-1-tmj-10.1177_03008916221128343 for The use of PSA testing over more than 20 years: A population-based study in North-Eastern Italy by Martina Taborelli, Federica Toffolutti, Ettore Bidoli, Luigino Dal Maso, Stefania Del Zotto, Elena Clagnan, Michele Gobbato, Diego Serraino and Silvia Franceschi in Tumori Journal
Footnotes
Acknowledgements
The authors wish to thank Mrs. Luigina Mei for editorial assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Italian Ministry of Health (Ricerca Corrente and RCR-2021-2367121, Alliance Against Cancer, WP 15, PPRER).
Research ethics and patient consent
Cancer Registries are identified as collectors of personal data for surveillance purposes without the need of explicit individual consent. The approval of a research ethic committee is not required as this descriptive study was conducted without any direct or indirect intervention on patients.
Data availability statement
The analyzed data are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.