
Abstract
Background:
Insertions of central venous catheters (CVC) has become a common practice in Onco-Hematologic Units to administer systemic treatments. Unfortunately they can cause complications influencing patient’s care-pathway significantly. Oncological patients have a higher thrombotic risk than the general population, therefore specific recent risk scores are spreading through the clinical practice, such as Khorana, Protecht, COMPASS-CAT, and Michigan scores.
Methods:
A retrospective cohort of 177 out of a total of 3046 outpatients accessing the Medical Day Hospital of Istituto Nazionale Tumori di Milano from March 2019 to February 2021 aged ⩾ 18 years who developed CVC complications was analyzed extracting clinical data from their medical records. Focusing on the risk factors, especially through recent risk scores to estimate the thrombotic risk we used Wilcoxon-test for continuous variables and the Pearson-Chi-Square test for categorical variables.
Results:
Anticoagulants resulted a protective factor mostly for partial CVC occlusion (p = 0.0001), preventing CVC occlusions. CVC occlusions were significantly associated with epitelial tumor histotype, (p = 0.0061). Complete CVC occlusions were significantly associated with peripherical inserted central venous catheters (PICC) (p < 0.0001). Catheter-related-thrombosis (CRT) was significantly associated with peripherical-inserted-central-venous-catheter, both when it was diagnosed clinically (p = 0.0121) and radiographically (p = 0.0168).
There was a strong association between CRT and a high grade of Khorana Score (p = 0.0195), Protecht Score (p = 0.0412), COMPASS-CAT Score (p = 0.0027). A positive statistical trend was observed between the Michigan Score and CRT in patients carrying PICC (p = 0.053).
Conclusions:
There are many different and various factors associated with higher or lower risk of CVC thrombotic complications, so it could be useful to test the recent risk scores to estimate thrombotic risk in oncological patients in clinical practice.
Keywords
Introduction
The insertion of central venous catheters (CVC) is a basilar clinical practice in oncological and hematological patients for the infusion of chemotherapy, parenteral nutrition, blood products, antibiotics and other systemic therapies. They can be inserted through a periferic vein, as a peripherical central venous catheter (PICC) that can last up to 6 months in situ, or through subcutaneous access, as Port-a-cath (PORT), which can last for an indefinite period in absence of complications.
Although their use is spreading in clinical practice, CVC can cause complications that can influence a patient’s care pathway significantly. Among the various CVC complications, the most common after infections is catheter-related-thrombosis (CRT), a multi-factorial entity. 1
CRT represents about 50-90% of all the deep venous thrombosis, and insertion of CVC is considered as an independent risk factor for it. 2 Moreover it is demonstrated that CRT is more frequent in oncological patients, with an estimated frequency of 5-10%. 3
CRT, as every thrombotic process, is caused from the Virchow’s triad: endothelial injury, hypercoagulability and altered blood flow.
Risk factors associated with CRT can be related to patient and type of therapy (for example tumor burden, oncological treatments, history of CRT, clinical patient conditions, thrombophilia) and to the catheter (for example type of CVC, time of permanence, access site, number of lumens). 4
CRT is not often recognizable because the majority of cases are asymptomatic. Sometimes when the thrombi involve the tip of CVC the only sign is the impossibility to infuse and to withdraw blood. When a superficial vein is involved, however, there can be pain, swelling and erythema along the vein course.
If CRT is misdiagnosed and not cured, in addition to the malfunctioning of the CVC, there can be serious consequences as pulmonary or right heart thromboembolism (TE), complicated infections with sepsis, post-thrombotic syndrome and chronic venous failure.
Diagnosis of CRT can be assessed, according to the American College of Chest Physicians (ACCP) guidelines with a venous duplex ultrasonography and eventually a D-Dimer assay as first-line tests; in case of negative tests but persistence of high suspicion of CRT it is necessary to do a contrast venography. 5
The problem of using instrumental tests, including the cost of these procedures, can be managed using a diagnostic clinical score, that helps to standardize the diagnostic process: the Costans Score. It includes four clinical signs (presence of an intravenous device, localized pain, unilateral edema, an alternative plausible cause for symptoms) and the results of this study show a high negative predictive value for patients with low scores (0-1 points) and negative D-Dimer test, with a failure rate of 0%. 6
Baskin and his team 7 described four classes of CRT based on the entity of the thrombotic process.
Therapeutic strategies for CRT are focused on reducing the symptoms, eliminating the CVC dysfunction, preventing CRT complications. 8
According to ACCP Guidelines from 2016, anticoagulation is effective in cancer-patients, using low molecular weight heparin (LMWH) heparin for almost 3 months. CVC should not be removed as routine in all patients with CRT, but only in case of infection or conditions that contraindicate anticoagulants for high bleeding risk. When CVC is removed is necessary to continue anticoagulation for other 3 months and monitor with instrumental exams. 9
In selected cases, such as severe symptoms, extended thrombus from axillary to subclavian vein, recent symptoms, no risk of bleeding, good performance status and good life expectation, using pharmacological thrombolysis with or without thrombectomy in addition to anticoagulants is suggested. Specifically, Tenecteplase 2 mg or Alteplase 2 mg can be instilled into the occluded catheter with a dwell time of 1-2 hours. In the major cases this is sufficient to relieve the occlusion (80-90% of the cases). 10
There are no specific methodologies for CRT prevention in patients with a CVC, in fact the only way is to choose the right dimension of CVC at the moment of insertion and remove the CVC when there is no more need for it. Moreover, FOTROCON Delphi consensus statement contra-indicates the systematic use of thromboprophilaxis in cancer patients with a CVC. 11
Based on these evidences and on the absence of other ways to prevent CRT in cancer patients, it can be useful to improve some recent scores to estimate thrombotic risk (as Khorana Risk Score, Protecht Score, COMPASS-CAT Risk Score) and CRT risk in patients with a PICC (Michigan Risk Score).12-14
Over the primary thrombotic risk of cancer patients, the typology of CVC can also influence the risk, mostly for CRT. In fact a systematic review from Johansson and her team has shown a higher risk of CRT in patients with a PICC and a lower risk for non-thrombotic obstructions in comparison with other CVC. 15
Aims
The aims of our study are to analyze the typologies of complications and outcomes of central venous catheters in a retrospective cohort of outpatients accessing the Oncology Department of Fondazione IRCCS Istituto Nazionale dei Tumori di Milano for systemic therapy and for CVC maintenance and to explore potential risk factors associated to CVC related thrombosis, applying the recent clinical risk scores.
Materials and methods
Inclusion criteria
Inclusion criteria were: oncological and hematologic outpatients aged ⩾18 years; accessing the Medical Day Hospital for CVC maintenance and for intravenous systemic treatments in Fondazione IRCCS Istituto Nazionale dei Tumori di Milano who developed a CVC complication; and patients with clinical information available for consultation, through their medical records.
Sample
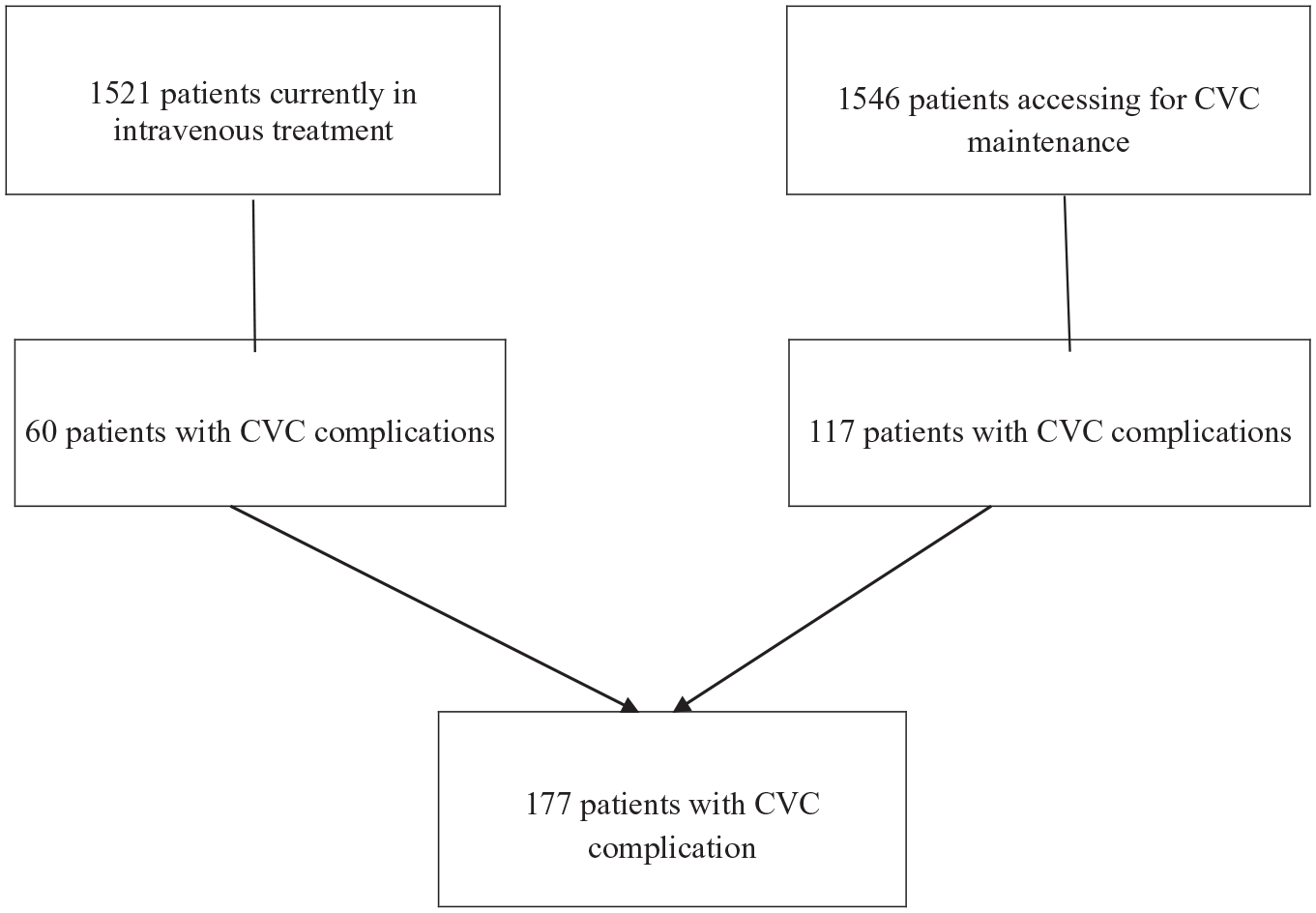
During the period from 1 March 2019 until 10 February 2021 about 1546 outpatients came in for CVC maintenance and about 1521 for intravenous systemic treatment to the Medical Day Hospital of Fondazione IRCCS Istituto Nazionale dei Tumori di Milano, totaling 3067 outpatients.
A registry of all the complications of CVC has been collected including all the clinical characteristics of the patients through their medical record, identifying a sample of 177 outpatients with CVC complications. Among these, 117 outpatients came in only for CVC maintenance, while 60 came for intravenous systemic therapies.
Diagnostic and therapeutic procedures
Current inner guidelines do not recommend the use of radiologic imaging as a routine procedure for CVC occlusion, consequently diagnosis of CRT was done considering clinical suggestive presentation when present and using imaging (fluoroangiography or ultrasonography or thorax X-ray) when diagnostic suspicion was considerable.
According to the European Guidelines, our unit uses validated procedures in case of CVC occlusion. They consist of one local application of fibrinolytic agent, urokinase, for a period of 1 hour with a maximum of two attempts in case of partial occlusion or four attempts in case of complete occlusion.
Statistical analysis
Descriptive analyses were based on standard statistics, such as percentages for categorical data, median and interquartile ranges for continuous variables. Between-group comparisons were performed with unpaired two-sample Wilcoxon-test when considering continuous variables. Regarding categorical variables, associations were investigated by means of Pearson’s Chi-square test (or Fisher’s test when appropriate because of small numbers), or by means of the Cochran-Mantel-Haenszel stratified test. The significance threshold was set at the conventional 5% level for two-sided tests. Statistical analyses were performed with the SAS® software, version 9.4.
Results
Descriptive analysis
Between 1 March 2019 and 10 February 2021 about 1546 patients accessed the Medical Day Hospital for CVC maintenance, and 117 of them developed CVC complications (7.6%), while about 1521 patients accessed to receive an intravenous systemic treatment, and 60 of them developed CVC complications (3.9%), see Figure 1.
Considering all the cases of CVC complications, among 177 patients about 176 had an occlusive one (partial or complete) and one patient had a malfunction of CVC (due to reverse central venous catheter).
According to CVC type, among 176 patients with a CVC occlusive complication, 89 had a PICC (peripheral inserted central catheter), 81 had a Port-a-cath and six had other type of CVC (Groshong, Pro-Line).
Moreover among 176 cases of CVC occlusive complication, 95 had partial occlusion (53.9%), while 81 had a complete occlusion (46.1%).
After applying the local fibrinolytic agent, 116 patients had a positive outcome (65.9%), 59 ones had a negative outcome (33.5%) and one patient had unknown outcome due to hospitalization for worsening conditions (0.6%).
Considering the 59 patients with a negative outcome after procedures, 20 accessed the unit to receive treatment (33.9%) and 39 accessed only for maintenance of CVC (66.1%).
Among the 176 patients with a CVC occlusion, 47 did an instrumental diagnostic test through ultrasonography or fluorangiography or thorax X-ray (26.7%), of which 39 did the test after a negative outcome with fibrinolytic.
Among these 47 patients, eight cases of CRT were identified, each one having a PICC (17%).
CVC occlusion and patient risk factors
Sample characteristics are summarized in the Table 1.
Sample characteristics.
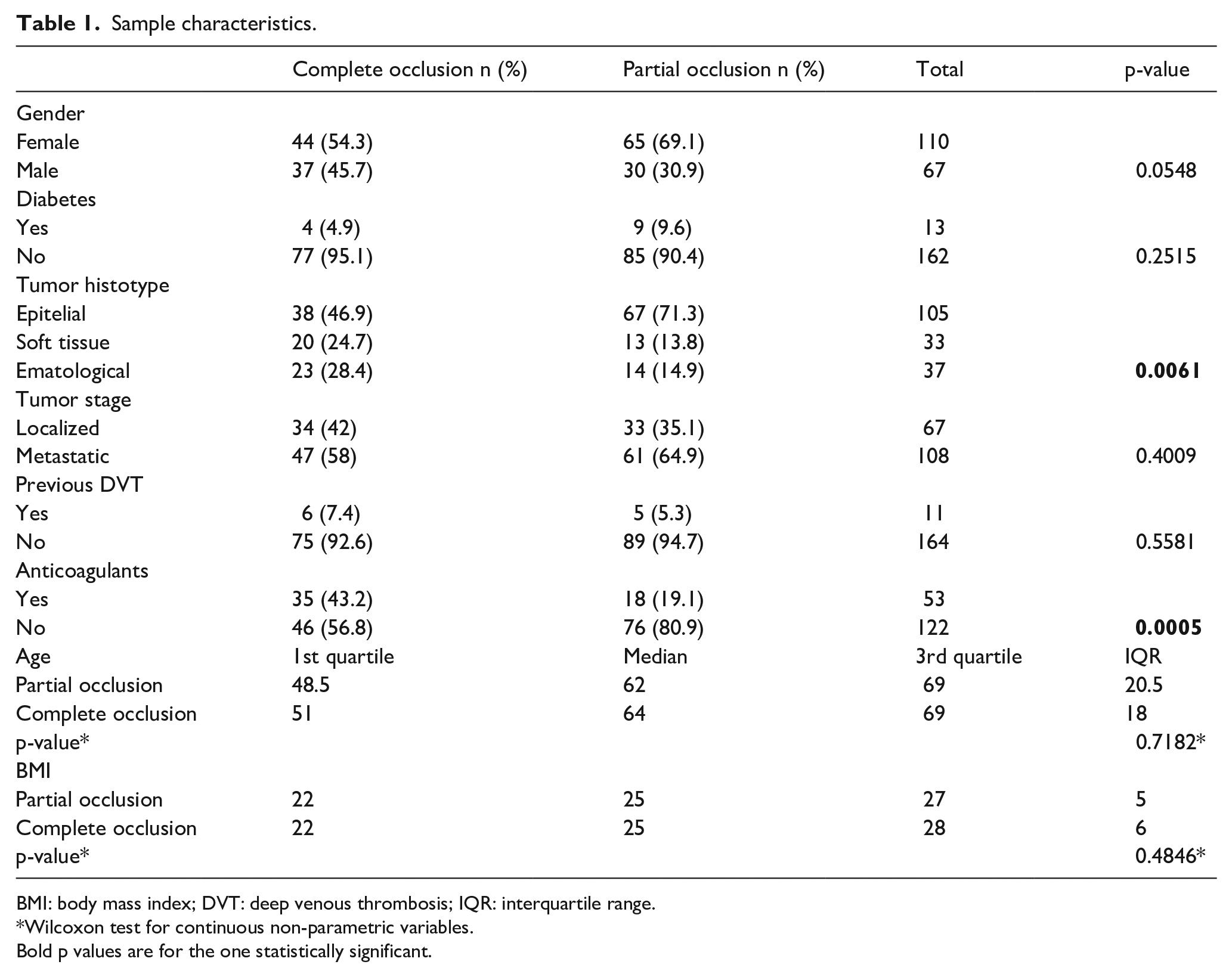
BMI: body mass index; DVT: deep venous thrombosis; IQR: interquartile range.
Wilcoxon test for continuous non-parametric variables.
Bold p values are for the one statistically significant.
Central venous catheter occlusion, especially partial type, was positively associated with epitelial origin tumors more than other hystologies (p = 0.0061).
Anticoagulants represent a protective factor, especially for CVC partial occlusion (p = 0.0001).
Besides, CVC occlusion is not associated to age, Body Mass Index, diabetes, previous deep venous thrombosis or tumor stage. A positive trend between CVC occlusion and feminine gender is observed (p=0.0548).
CVC occlusion and central venous catheters characteristics
Complete CVC occlusion resulted more frequently in patients having PICC than those with other types of CVC (p<0.0001), see Table 2. Stratifying the sample for type of CVC and for having CRT or not, the association between CRT and PICC is clear, both when the CRT was diagnosed clinically and radiographically (p=0.0168), see Table 3.
Type of occlusion in association with type of central venous catheter.
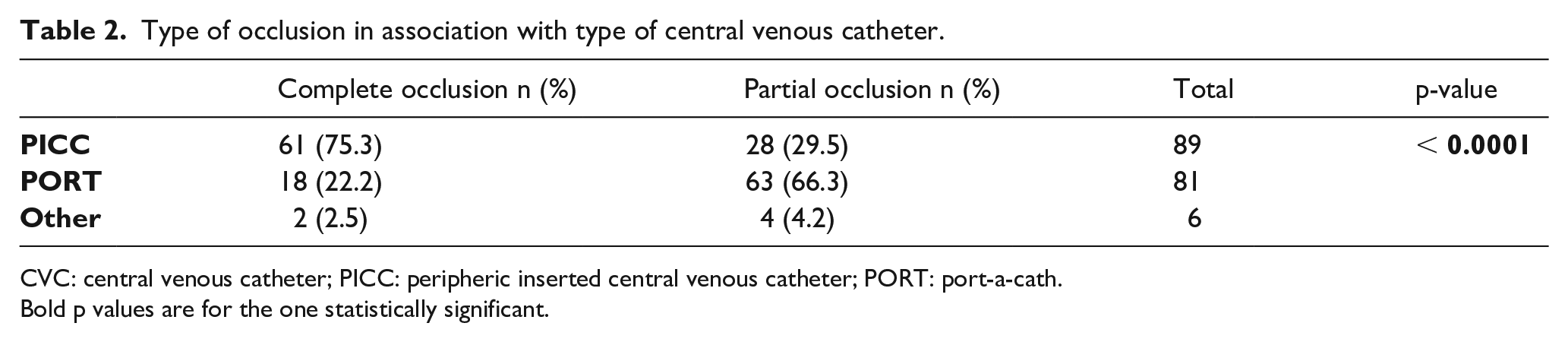
CVC: central venous catheter; PICC: peripheric inserted central venous catheter; PORT: port-a-cath.Bold p values are for the one statistically significant.
Catheter related thrombosis and association with radiographical and clinical diagnosis.
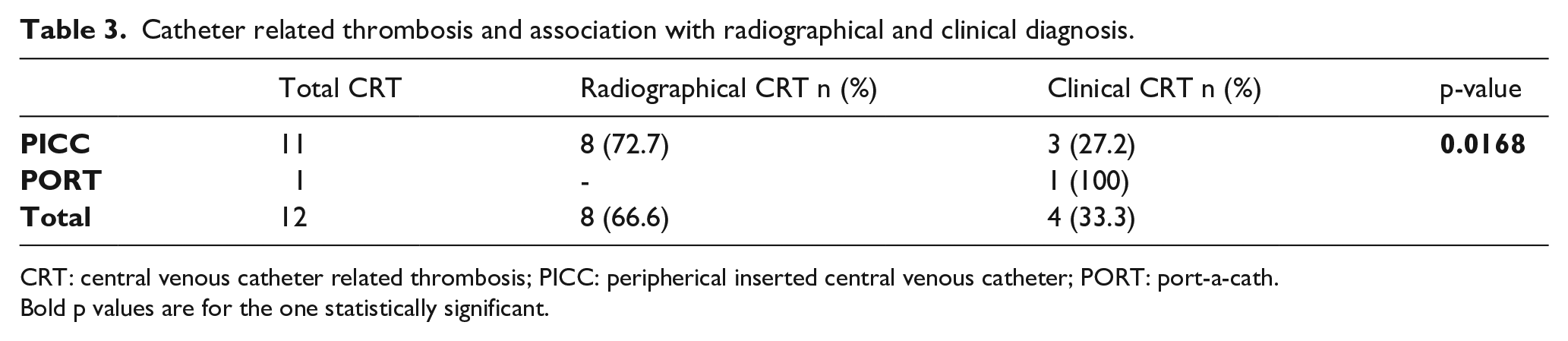
CRT: central venous catheter related thrombosis; PICC: peripherical inserted central venous catheter; PORT: port-a-cath.Bold p values are for the one statistically significant.
On the other hand, having a previous CRT seems not to increase the risk of CVC occlusion.
CVC occlusion and risk scores
Testing for the upcoming risk scores patients with a CRT, a strong positive association is evident between developing CRT and thrombosis score grade applying Khorana (p = 0.01), Protecht (p = 0.04) and COMPASS (p = 0.002) risk scores.
For patients with PICC, the Michigan Risk Score was applied, but that failed to demonstrate a strong statistical significance in association with developing CRT, although it was borderline (p = 0.053), see Table 4.
Association between upcoming scores and central venous catheter thrombosis.
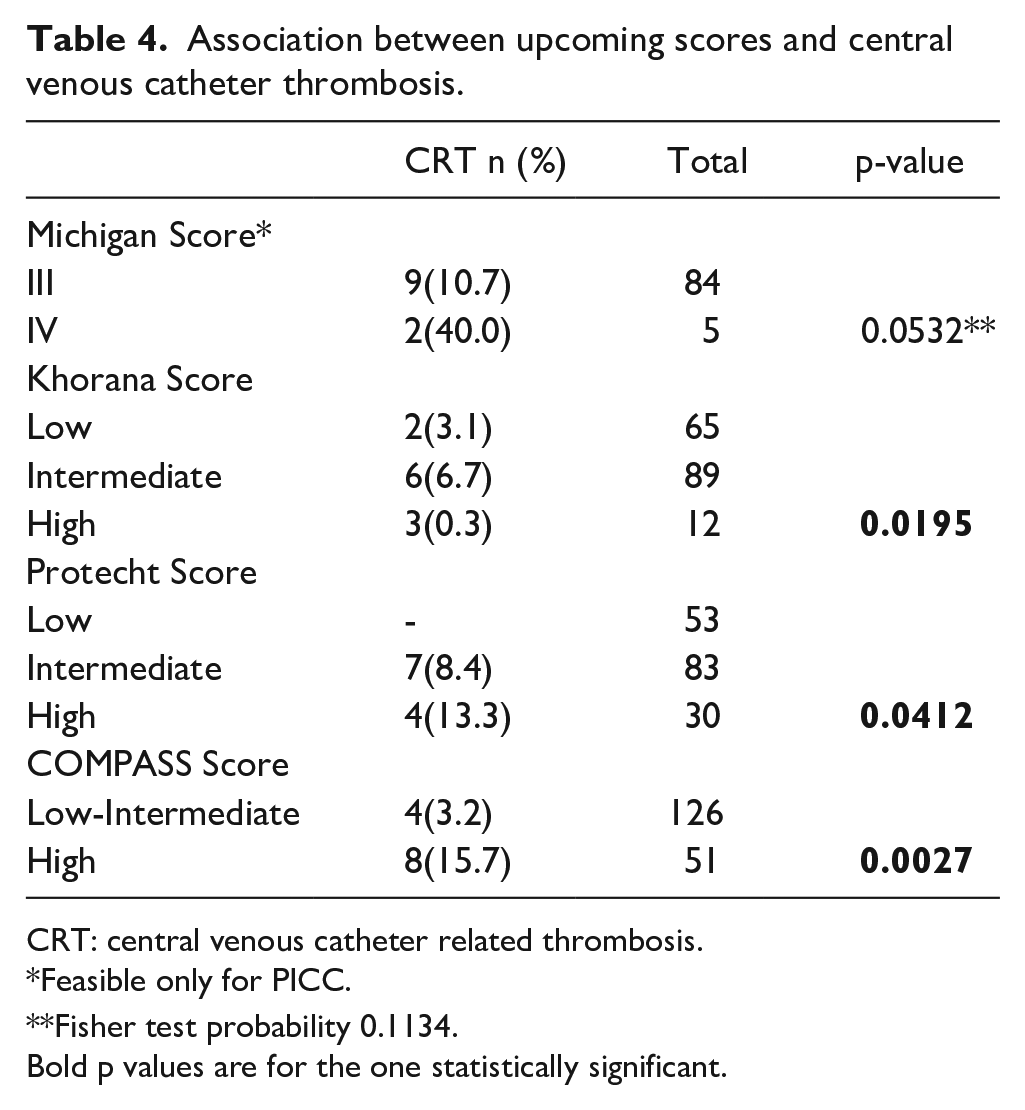
CRT: central venous catheter related thrombosis.
Feasible only for PICC.
Fisher test probability 0.1134.
Bold p values are for the one statistically significant.
Discussion
Our analysis suggests that the most frequent CVC complication observed in outpatient clinic is the occlusive one, instead of infections, which is more frequent in hospitalized patients.
In our experience PICCs resulted more thrombogenic than other types of CVC, with the majority of complete occlusion in comparison with others. This is confirmed in the literature 15 and the biological reason stands in a double way to induce activation of coagulation pathway: directly activating factor XII and wall injury induced by the PICC itself. 16 This, in association with other coexisting factors in oncological and hematological patients, increases the risk of developing a CRT compared to other types of CVC.
Anticoagulant therapies resulted in a prophylactic role. Shoutian et al 17 demonstrate an important role of anticoagulants especially in patients with PICC, who have a superior thrombosis risk compared with other patients carrying other CVC.
An important question regards the diagnosis of CRT, which is occasionally hidden because of the absence of symptoms. In our study 17% of CRT were diagnosed radiographically, while for the most part of CRT was diagnosed clinically.
Also stratifying for the presence of a radiographical diagnosis of CRT, PICC-CRT were for the most part compared with other CVC.
CRT has been associated mostly with carcinomas than other histological types. This can be related to the fact that this category included a number of tumors with a major thrombogenic attitude due to treatments and to biologic characteristics (breast 20%, lung 18.3%, gastro-intestinal tract 10%, uro-genital tract 3.3%). In terms of stage, metastatic carcinomas were 61.9% while localized ones were 38%.
Our study supported the predictive role of the main upcoming thrombotic risk scores in oncology, resulting in an association between CRT and higher grade of Khorana Risk Score, Protecht Risk Score and COMPASS Risk score. Even if CRT is a different entity as concern the pathogenesis and the site of development, the presence of a correlation suggests the multifactoriality of CRT pathogenesis and the similarities with other deep venous thrombosis not CVC-related.
We cannot prove a statistically significant association between high class of Michigan Risk Score and CRT in PICC-carrying patients, probably due to the exiguous cases of CRT detected in our sample, preserving a positive statistical trend. If we analyze qualitatively the two cases who developed CRT having high-risk class of Michigan Risk Score, we see that both of them had a previous DVT, while the other cases of CRT with an intermediate-risk class of MRS had a lower percentage (1:9) of this condition. Despite of the exiguous number of cases of CRT detected in our sample, this can be considered a relevant pathogenic element in developing thrombotic CVC complications. The link described could probably be a starting point to study in an extended sample of other possible markers influencing risk of CRT. Knowing already the major thrombotic tendency of PICC instead of other types of CVC, adding coagulation indexes (as D-Dimer, Fibrinogen, platelet levels) could guide towards a more individualized way of choosing the type of CVC to insert.
The limits of our study are the lack of a control arm and the elongation of the intervals between maintenance due to the pandemic period, potentially influencing our results. This could represent a basis for a future study with a more complex design.
Conclusions
Patients affected by oncological and hematological illnesses have an increased risk of developing thrombosis. Therefore a baseline evaluation of the thrombotic risk can be relevant in order to avoid complications that can influence the care pathway and the quality of life.
The risk of CRT estimated with the clinical scores shown in our case series supports the importance of applying them in the clinical practice.
It is likely that, with future evidence from interventional studies, the use of recent risk scores could drive the choice of the proper CVC to insert in every patient, limiting CRT events.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.