
Abstract
Objective:
In this study, we aimed to analyze technical and diagnostic potential, and safety of the small-caliber vacuum-assisted biopsy (SCVAB) device in a multicenter consecutive study taking into consideration the type and location of breast lesion.
Methods:
We collected data from 5 breast imaging centers where radiologists used the SCVAB device for biopsies in 162 patients. We analyzed the conditions for using the SCVAB device according to the characteristics of the lesions, the volume of excision, and the analyzability obtained by biopsy samples.
Results:
The biopsies of 80 circumscribed masses, 61 complex lesions, and 24 microcalcification foci were included in the study. The reasons for choosing SCVAB as an initial technique were identified. A total of 47 lesions were removed with SCVAB; among them, 24 lesions were initially chosen for total excision. SCVAB was used as a second-choice biopsy method after core-needle biopsy failure in 20 cases. If SCVAB had not been available, vacuum-assisted biopsy would have been the most frequently used technique (106 under ultrasound, and 18 under stereotactical guidance).
Conclusions:
The SCVAB system is an alternative to classical vacuum biopsy, enabling representative samples to be obtained from lesions that are difficult to access, complex, small, or in cases of unsuccessful previous biopsy. The SCVAB system was determined as the chosen technique by the radiologists in this study due to feasibility, ergonomics and absence of side effects detected in this study.
Introduction
Breast cancer is the most frequently occurring cancer among women and the cause of death of more than 500,000 women worldwide every year. Regardless of increasing incidences since the 1990s, there has been a tendency of decrease in breast cancer mortality over the last 25 years in Europe and North America. This could be explained at least in part by implementation of medical imaging techniques for the detection of breast cancer at earlier stages, follow-up of patients who undergo targeted treatment, and control after remission.1,2
The next step in management of detected lesions is biopsy under ultrasound, stereotactic, or MRI guidance. Obtaining good-quality samples for histopathologic examination is essential for a definitive diagnosis that permits optimal preoperative workup, counseling, and surgical planning for patients with malignant breast lesions. The goal is to make the diagnostic procedure minimally invasive with a needle and to go to the operating room one time for definitive treatment. There are several percutaneous tissue acquisition techniques currently in use.3-7 The core needle biopsy by 14-G caliber has been one of the prevailing methods since it was first performed. 8 However, this technique has limitations related to technical aspects and the quantity of obtained breast tissue. The aim of the biopsy is to obtain sufficient and precise tissue samples for diagnosis, particularly in cases of microcalcification foci. This led to development of vacuum-assisted biopsy systems, initially with 11-G caliber needles.4,8-16 Understanding that larger tissue samples allow the most accurate anatomopathologic diagnosis resulted in the development of devices with calibers up to 7 G and systems for monobloc excision.17-19 The role of vacuum-assisted biopsy was extended to therapeutic procedures. 20
A vacuum-assisted biopsy device equipped with a smaller 13-G needle is available (Mammotome Elite®, Leica Biosystems, Newcastle, UK; Vacora, Bard, Tempe, AZ). This device combines the beneficial characteristics of core needle and vacuum-assisted biopsy techniques and may be implemented with positive outcomes according to this study.
The objective of the study was to analyze technical success, diagnostic potential, and safety of a small-caliber vacuum-assisted biopsy (SCVAB) device in a multicenter consecutive study taking into consideration the type and location of breast lesions. We aimed to show in certain clinical situations SCVAB appears more suitable than other techniques of biopsies. The histologic results are not listed in this study, but we took into consideration the lesion characteristics size, form, and localization, and the analyzability of the sample obtained by Mammotome Elite (sufficient for the follow-up decision or not).
Methods
The Institutional Review Board of the University Hospital of Nimes approved this prospective consecutive multicentric study (reference 16.11.01).
The data were collected from 5 accredited breast imaging centers in France (4 private cancer centers and 1 public center) where SCVAB devices were used for breast biopsies during 6 months. In this study, 162 patients (mean age 45 years old; range 25–78) were eligible for analysis. All patients signed informed consent. Women with breast lesions detectable by ultrasound underwent SCVAB either as a first-choice method or after failure of another system. The device was chosen according to the type and location of the lesion.
The SCVAB device Mammotome Elite is equipped with a 13-G-caliber needle and a vacuum aspiration mechanism. The biopsy cycle includes several steps: a vacuum is created, the samples are acquired by rotating and moving the knife forward at the biopsy site, and the tissue is transported into a collector cup at the rear of the gun (Figure 1). This insertion technique allows the collection of multiple samples. The needle was generally placed by the deep edge of the lesion, which allows it not to be hampered by its acoustic artefact and, thus, to appreciate well the targeting and the extent of the samplings within the lesion. The absence of removal and return of the needle during the procedure prevents the occurrence of air artifacts and targeting errors. All the biopsies were ultrasound-guided (analysis in the 2 orthogonal plans) under local anesthetic in sterile conditions (Figure 2). The number of taken samples varied for each biopsy and depended on the type and size of the lesion.

Small-caliber vacuum-assisted biopsy device (Mammotome Elite) with 13-G caliber needle.
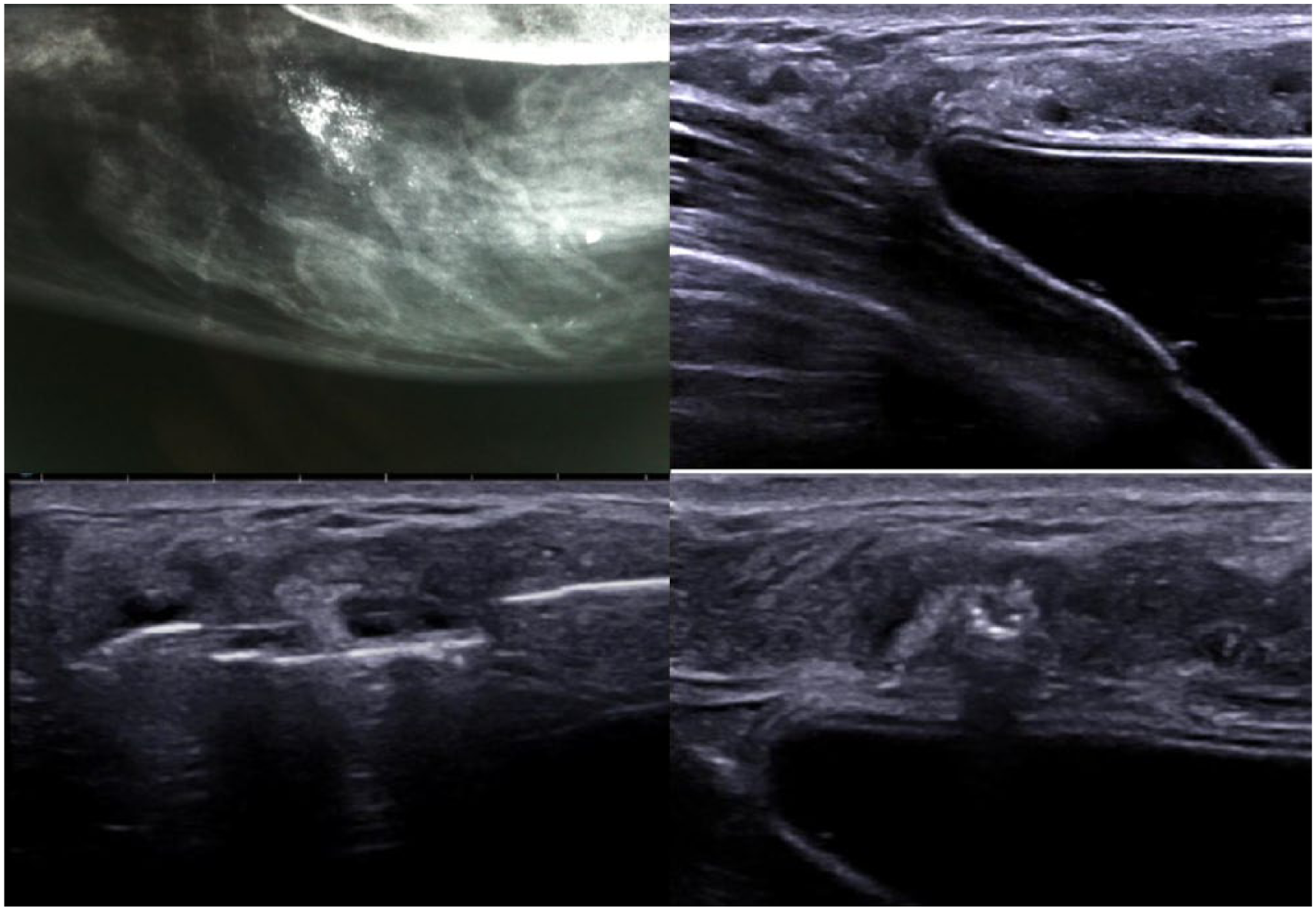
Microcalcification foci ACR4 (a, left upper corner). Impossible to perform stereotactically guided biopsy: lesion visible with ultrasound (b, right upper corner). Macrobiopsy of foci with ultrasound-guided Elite device. Needle positioning (c, d; left and right lower corners).
Among analyzed parameters were patient demographics, medical history including previous biopsy for the same lesion (the type of method), the volume of excision, the sample’s analyzability, and the complications. The lesion characteristics were defined as follows: (1) circumscribed masses, (2) complex masses with heterogeneous echogenicity (Figure 3), (3) noncircumscribed masses, and (4) clusters of microcalcifications (Figure 2). The longest axe of the lesion and its position within the breast were described as within mammary gland, subcutaneous, or on the pectoral wall. The reasons why SCVAB had been selected were also noted. More than one reason could be selected and could be related to the characteristics of the lesion (size, difficulty of access), desired sample volume (representative, total excision), and finally the ease of use compared to other techniques (based on volume and density of the breast). For each biopsy, the radiologists were queried about other techniques (i.e., fine needle aspiration, stereotactic or ultrasound-guided core needle biopsy, surgical incisional biopsy) they would have alternatively chosen if SCVAB was not available.
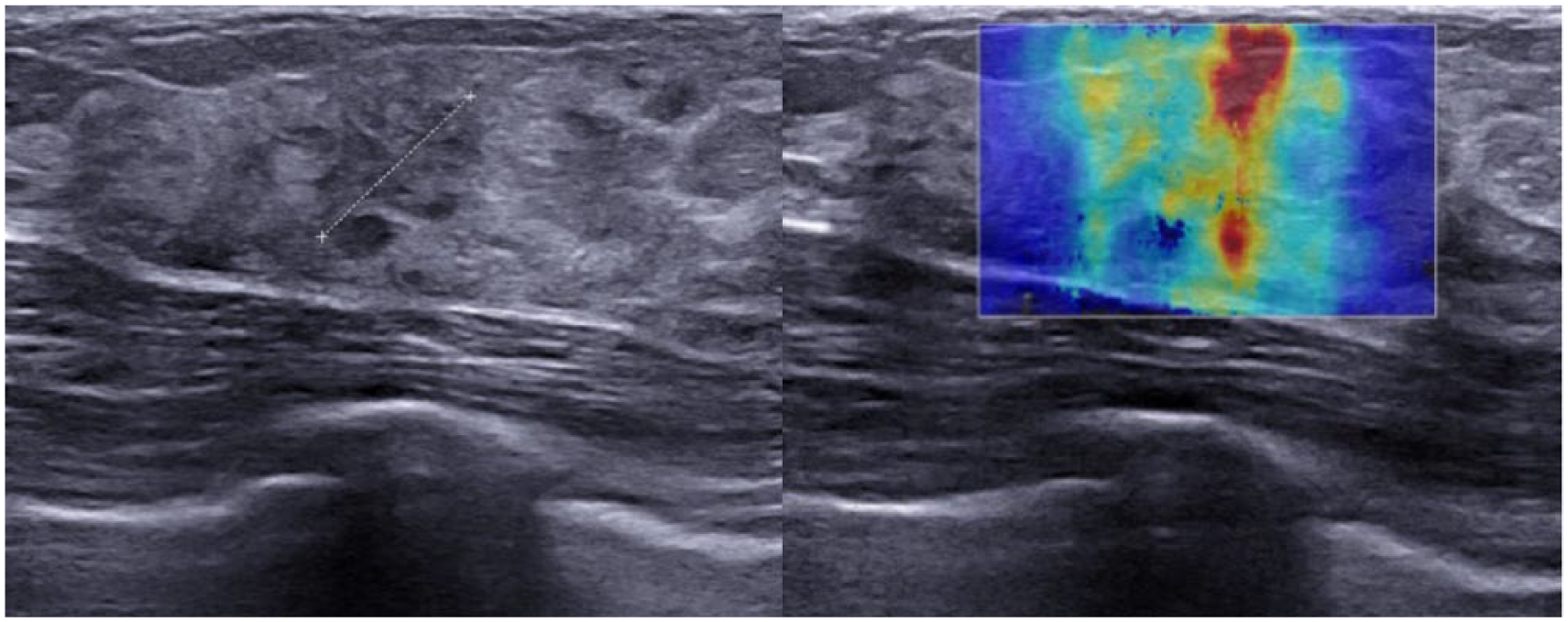
Complex lesion ACR4b (oval, microlobulated margins, heterogeneous echogenicity, stiff on elastography) biopsied by small-caliber vacuum-assisted biopsy.
Immediate complications and adverse effects such as bleeding, skin or pectoral wall wound, unusual pain, vagal episode, and SCVAB system dysfunction were registered in the radiologists’ report. At 1 month, follow-up was performed by phone in order to evaluate satisfaction and midterm complications.
Results
Among the 162 SCVAB-biopsied lesions included in the study, there were 61 circumscribed lesions, 77 complex lesions, and 24 clusters of microcalcifications. The lesions were located within mammary glands (n=99), subcutaneously including retroareolar and axillar region (n=35), and on the pectoral wall (n=28). The mean diameter of the lesion was 9.1 mm for the circumscribed lesions, 9.5 mm for the clusters of microcalcifications, and 12.8 mm for the complex lesions. The microcalcifications’ foci were located within mammary glands (n=11), subcutaneously (n=8), and on the pectoral wall (n=5). The complex lesions were located within mammary glands (n=43), subcutaneously (n=23), and on the pectoral wall (n=11). The circumscribed lesions were located within the mammary glands (n=45), subcutaneously (n=12), and on the pectoral wall (n=4) (Table 1).
Location and size of biopsied lesions using the SCVAB device.
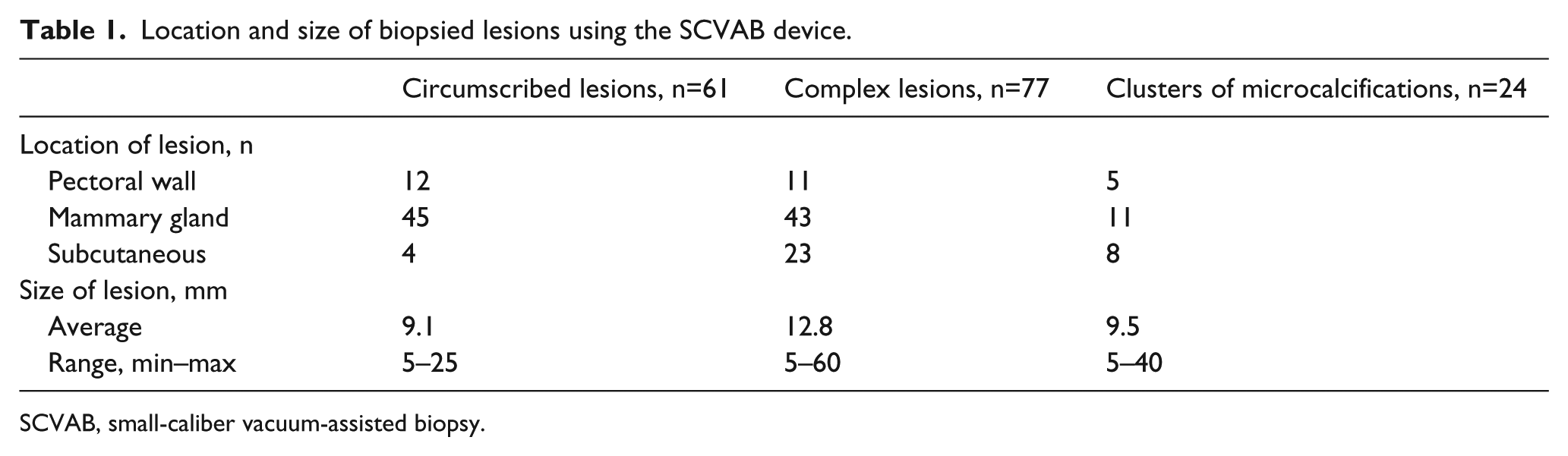
SCVAB, small-caliber vacuum-assisted biopsy.
The reasons for choosing SCVAB as an initial technique were identified as small size of the lesion (n=45), difficult access (subcutaneously, retroareolar and axillar region, and pectoral wall; n=58), in order to obtain a representative sample (n=118), and comfort in use (n=60). In 99.3% of cases, representative samples were obtained by SCVAB in first intention biopsies (1 case of system dysfunction). In 42% of cases (60 of 142), SCVAB was chosen due to the simplicity of use compared to ultrasound-guided vacuum-assisted biopsy (Table 2).
Reasons for choosing the SCVAB device or an alternative method.
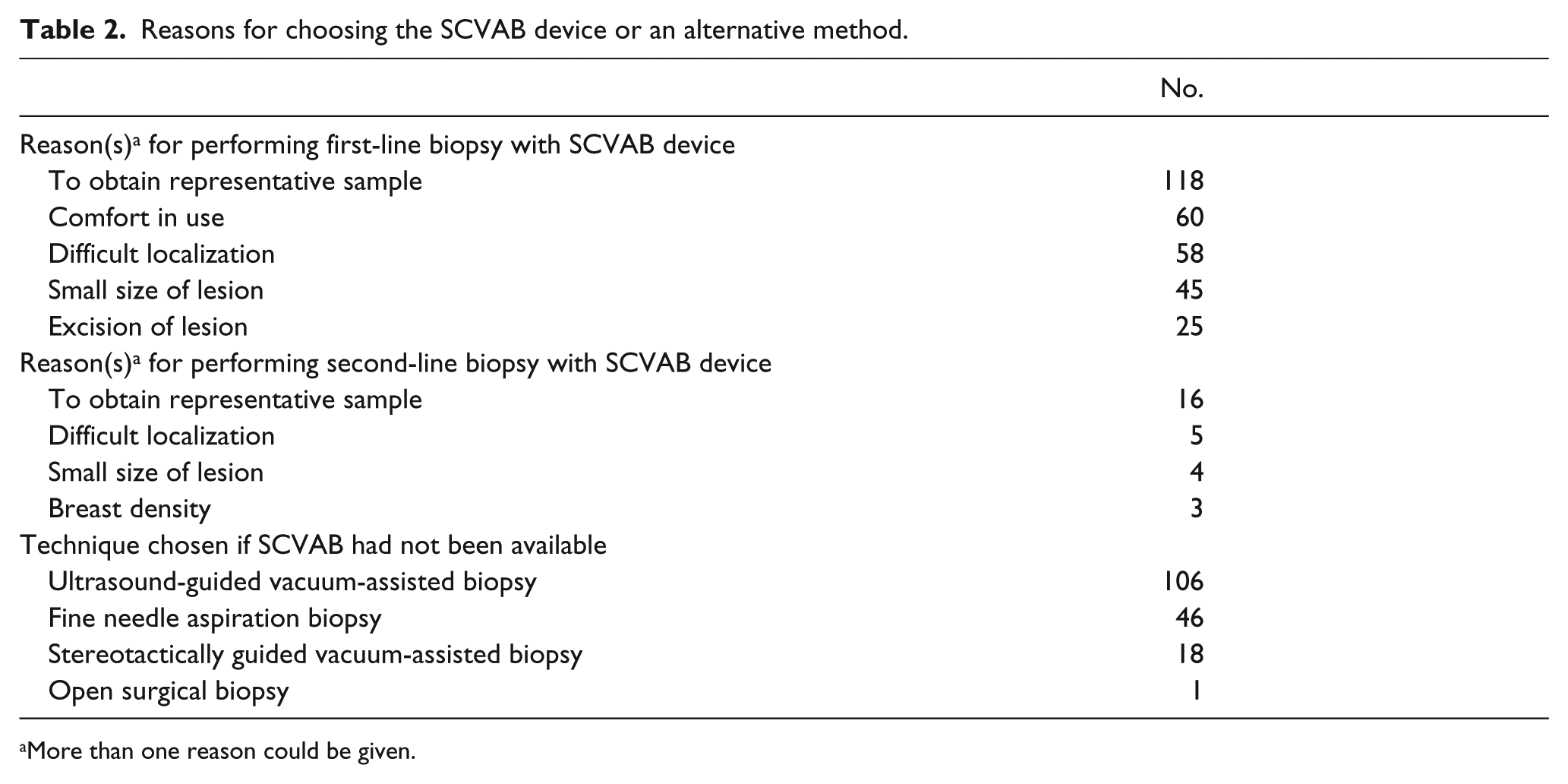
More than one reason could be given.
A total of 47 lesions from 4 to 16 mm were removed by the SCVAB device. Twenty-four lesions were initially chosen for total excision by SCVAB. The success rate was 96% (1 lesion measuring 11 mm was not completely removed). For 4 to 5 mm lesions (n= 11), the success rate was 100%. Twenty-three lesions were not initially intended to be removed.
SCVAB was used as the first technique for the biopsy of 142 lesions, and in 20 cases after failure of core needle biopsy. Twenty samples obtained with previous biopsy could not have been analyzed according to anatomopathologic criteria. Among them, 3 technical failures, failures due to the lesion size (n=9), position (n=5), and breast density (n=3) were described. The reasons for choosing SCVAB were described as follows (more than one could be given): difficult access due to the lesion size (n=9), position (n=5), or breast density (n=3), or aiming to obtain a representative sample (n=16) (Table 2). Finally, the larger volume of the samples obtained with SCVAB, as depicted in Figure 4, led to improved diagnostic accuracy compared to core needle biopsy (14 G) in these 20 cases.
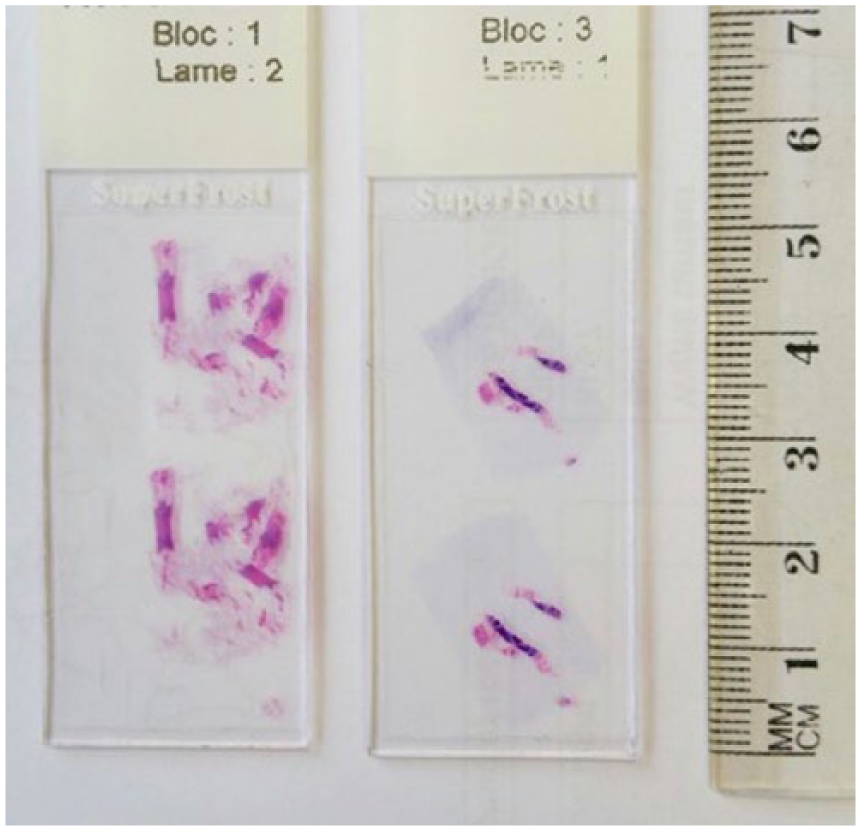
Biopsy volume by small-caliber vacuum-assisted biopsy device 13 G (bloc 1, lame 2) and ultrasound-guided core needle biopsy 14 G (bloc 3, lame 1).
According to radiologists’ responses (Table 2), if SCVAB had not been available, vacuum-assisted biopsy would have been the most frequently used technique (106 under ultrasound and 18 under stereotactical guidance). This is followed by core needle biopsy in 46 cases and surgical excision in 1 case.
The results from the biopsy enabled 162 patients to be diagnosed and treatment to be decided (99.3% of the first intention biopsies and 100% of the second intention biopsies).
Conclusion
The results suggest that SCVAB is a feasible technique with few complications (1 case of bleeding and 1 case of system dysfunction reported). Regardless of the lesion type (solid or clusters of microcalcifications), the histologic results obtained with the biopsy sample were always sufficient to proceed with treatment decisions for patients. The participating radiologists were all experienced with ultrasound-guided core needle biopsies, but not all were experienced with ultrasound-guided vacuum-assisted biopsies. A solid experience in core needle percutaneous tissue acquisition coupled with specific training organized by the device manufacturer were sufficient to allow the radiologists to maneuver the SCVAB device and obtain the samples.
The radiologists selected the SCVAB device due to its efficiency and feasibility. Its small caliber needle made it almost as simple to use as the core needle biopsy gun. The classic vacuum-assisted biopsy systems have larger needles and are less easy in use due to the fluid collection tube coupled with the central unit. In almost all technical conditions, the required amount of targeted tissue was obtained with few complications.
The Vacora Bard system requires a coaxial guide and the needle has to be removed from the breast after each biopsy in order to collect the sample before proceeding to the next biopsy. This is not the case with the Elite system, where the samples are collected automatically in a cup, which allows leaving the needle in place during the procedure. This is an advantage for ultrasound-guided procedures as the needle needs to be moved as little as possible in order to maintain the precise targeting of the lesion and to avoid air-generated artifacts. The aspiration mechanism used in both systems (Vacora Bard and Mammotome Elite) allows collecting a volume greater than that of the classic core needle of the same caliber. Neither system requires a connection to an external module or power source during the procedure.
The Mammotome Elite device has the same technical advantage as the vacuum-assisted technique; that is, a single insertion allowing multiple samples to be collected until the required volume is achieved for correct histologic analysis. SCVAB offers similar advantages to vacuum-assisted biopsy in the approach to ultrasound detectable lesions, enabling a representative sample to be taken in 118 of 142 cases of first intention biopsies (Table 2). SCVAB provided an effective management of previous biopsy failures in 20 cases.21-23 In 2/5 of the cases, the SCVAB was chosen due to the simplicity of use compared to ultrasound-guided vacuum-assisted biopsy (Table 2). The core needle biopsy remains the reference in solid lesions. SCVAB was used for complex lesion with heterogeneous echogenicity in order to obtain representative sample (Figure 4) or when core-needle biopsy was not technically feasible, e.g., axillar or retroareolar region.
Despite varying experiences in ultrasound-guided vacuum-assisted biopsy, the radiologists strictly complied with the indications for vacuum-assisted biopsy that corresponded to the technical and histologic requirements regarding the type of lesion.23-25 The technical constraints that would have made core needle biopsy difficult to perform were as follows: size, location, deformability of the breast, difficulty to penetrate, or presence of breast implants. With SCVAB, the risk of pectoral wall or cutaneous complications is lower than with core needle biopsy because there is no shotgun principle used. Greater volume of obtained sample reduces the risk of false diagnosis related to the poor targeting of small lesions. The risk of false-negative diagnosis is significant in core needle biopsies for the samples taken from complex lesions or with indistinct borders, whereas SCVAB permits the collection of larger and better analyzable samples in these cases. For all the patients in this study, the definitive treatment decisions were based on the histopathologic analysis of the samples obtained by SCVAB. In particular, SCVAB was identified as a favorite device to biopsy small lesions and those with difficult access. The small caliber of the needle makes the penetration of the breast easier than with classic vacuum-assisted biopsy, and the procedure is less dependent on breast density or deformability. These qualitative and quantitative advantages contribute to significant reduction of misdiagnosis. In cases of radiologic/histologic discordance or discovery of atypical hyperplasia on first biopsy, the choice of SCVAB use in second intention must be discussed from case to case because of the limited possibilities of complete lesion excision by this device (small caliber of needle). 26
Ultrasound-guided vacuum-assisted biopsy can be considered as an alternative to surgical biopsy for excision of benign lesions, such as fibroadenomas, papillomas, and radial scars.21,25,27,28 These devices have a larger-caliber needle or a monobloc excision system. In our study, SCVAB was primarily chosen for tissue acquisition for diagnostic procedures because the small-caliber needle (13 G) limits the excision potential of the device.14,29 In our study, SCVAB was also used for total excision of 24 lesions that were initially targeted for excision and showed 100% efficacy for removal of 4 to 5 mm lesions.
Among the limitations of our study is the absence of randomized comparison with another technique. The radiologists selected patients based on technical and clinical guidelines and their own experience. However, the conditions of this study reflect a real-life setting that the radiologists face in their practice. The decisions regarding the choice of biopsy technique based on the characteristics of each lesion were assessed. A total of 162 patients were included in this study.
In addition, we obtained data for the Mammotome Elite system SCVAB device, so we cannot extrapolate our results to other available vacuum-assisted small-caliber biopsy devices.
These results show the SCVAB device as advantageous in the range of available percutaneous biopsy devices. SCVAB proved to be an ergonomic alternative to classical vacuum-assisted biopsy and core needle biopsy due to failure in the 20 cases. The device permits obtaining representative samples with good analyzability from small lesions with complex echogenicity or ones with difficult access particularly in axillar and retroareolar regions. The SCVAB device is simple to use for various reasons discussed earlier and offers the benefit of collecting the required amount of tissue, which is why the radiologists from 5 centers selected it for their clinical practice. In previously discussed conditions, the SCVAB device can be safely used for excision of 5-mm breast lesions.
Footnotes
Acknowledgements
The authors thank Daniel Deschamps, MD, Brigitte Marie, MD, and Gaelle Gillis, MD, for their participation in inclusion of the patients; and Lucia Luconi of Devicor Medical for help in data processing.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.