
Abstract
Nail lichen planus is a chronic inflammatory condition that may be isolated to the nail, resulting in longitudinal nail ridging, trachyonychia, and splinter hemorrhages, and may be highly refractory to conventional treatment. The management of nail lichen planus remains challenging because of the lack of standardized treatment guidelines, and the efficacy of existing therapies, both topical and systemic, is often inconsistent or unsatisfactory. Emerging reports have suggested that abrocitinib, a selective Janus kinase 1 inhibitor, may be safe and effective in treating severe nail lichen planus. This report describes the case of a woman in her late 40s with refractory nail lichen planus who was successfully treated with abrocitinib.
Introduction
Nail lichen planus (NLP) is an inflammatory disorder affecting the nail unit that occurs in approximately 10%–15% of patients with cutaneous or mucosal lichen planus (LP) and occasionally present as an isolated entity. 1 NLP is characterized by a spectrum of nail findings, including longitudinal ridging, trachyonychia, distal splitting, and subungual hyperkeratosis. Additionally, it may present with the irreversible, pathognomonic sign of dorsal pterygium, which indicates severe nail matrix damage resulting from inflammation or trauma. Without intervention, the disease can progress to irreversible sequelae such as scarring, anonychia, and significant functional impairment, thereby underscoring the importance of early diagnosis and management to mitigate permanent damage. Dermoscopy serves as a critical adjunct for detecting subclinical nail involvement in LP, revealing markedly higher prevalence of subtle features such as multiple splinter hemorrhages, onycholysis, prominent hyponychial vascular structures, and longitudinal erythronychia that are often invisible to the naked eye.2,3 In atypical or refractory cases, nail unit biopsy with histopathological examination remains the gold standard for definitive diagnosis and for excluding mimics such as psoriasis or onychomycosis. 4
Current therapeutic strategies for NLP include high-potency topical or intralesional corticosteroid injections, intramuscular corticosteroid injections, retinoids, and immunosuppressive agents. However, these approaches are frequently limited by suboptimal efficacy, high relapse rates, and adverse effects and are unsuitable for all patients with NLP, particularly those with refractory disease. 5 Intralesional injections, although effective, are often poorly tolerated because of procedural pain and require repeated administration. Systemic therapies are associated with risks of long-term toxicity, including hepatic, renal, and metabolic complications, further complicating management. 6
Recent insights into NLP pathogenesis have highlighted the role of T cell–mediated inflammation driven by interferon-γ (IFN-γ) signaling via the Janus kinase (JAK) and signal transducer and activator of transcription (STAT) (JAK-STAT) pathway. This cascade promotes keratinocyte apoptosis and cytotoxic cluster of differentiation 8 (CD8)+ T cell recruitment, ultimately leading to nail matrix destruction. JAK inhibitors, which disrupt this pathway, have emerged as promising targeted therapies.7,8 Case reports and pilot studies have described the successful use of JAK inhibitors (e.g. tofacitinib and baricitinib) in patients with refractory NLP, with rapid nail improvement and minimal adverse effects.9–11 Abrocitinib, a selective JAK1 inhibitor, blocks downstream signaling of pro-inflammatory cytokines (e.g. IL-4, IL-13, and IFN-γ) and offers theoretical safety advantages over pan-JAK inhibitors because of its specificity.12,13 Previous case reports have supported its use in NLP.14,15
Herein, we report the case of a woman in her late 40s with more refractory NLP than that described in previous reports who was treated successfully with abrocitinib.
Case report
The reporting of this study conforms to Case Report (CARE) guidelines. 16 Written informed consent for treatment and publication of this case was obtained from the patient. A woman in her late 40s presented to Daping Hospital, Army Medical University (Chongqing, China), in June 2024 with a more than 3-year history of progressive dystrophy affecting all 10 fingernails. She was successively diagnosed with onychodystrophy, tinea unguium, and nail psoriasis at other institutions. Over the subsequent 2.5 years, she received various treatments, including oral multivitamins, topical halometasone, calcipotriol, and oral terbinafine, all of which proved ineffective.
Subsequently, the patient sought care at a different hospital, where nail biopsy with pathological examination confirmed the diagnosis of NLP (Figure 1). Following the diagnosis, she underwent a four-month treatment regimen consisting of intralesional corticosteroid injections (1 mL of triamcinolone acetonide mixed with 1 mL of 1% lidocaine in a 1:1 ratio), topical steroids, anti–interleukin-8 cream (mouse monoclonal antibody against human interleukin-8 cream), and oral medications (compound glycyrrhizin tablets, hydroxychloroquine sulfate, total glucosides of paeony, and tretinoin). Although minor improvement was observed, the intralesional injections had to be discontinued because of severe pain and nail bleeding. Consequently, the nail condition deteriorated further, and the patient developed significant anxiety and insomnia.
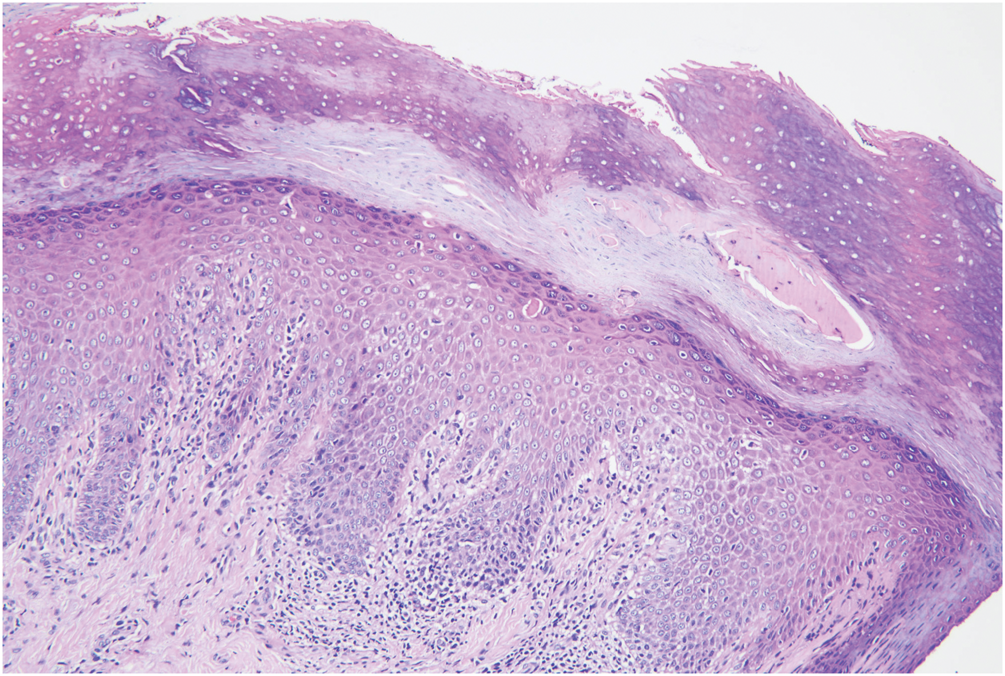
Photomicrograph of the histopathology of a nail biopsy specimen from a woman in her late 40s with refractory nail lichen planus. Histopathological examination showed hyperkeratosis and parakeratosis (top), thickening of the epithelial granular layer, acanthosis, necrotic keratinocytes, and degeneration of basal epithelial cells. The underlying dermis contained a mild inflammatory infiltrate of lymphocytes. Hematoxylin and eosin (H&E); magnification 20×.
Finally, the patient was referred to our hospital for further management. Her medical history was significant for atopic dermatitis and allergic rhinitis. Although atopic dermatitis can occasionally cause nail changes, the characteristic clinical presentation and histopathological findings confirmed the diagnosis of NLP and excluded atopic dermatitis-related onychodystrophy. All laboratory findings were within normal limits, including complete blood count, liver and renal function tests, lipid profile, thyroid function tests, and screening for viral hepatitis. A chest computed tomography (CT) scan performed at an external hospital was also unremarkable. Physical examination revealed trachyonychia, longitudinal ridging, fissuring, diffuse erythema of the lunula, and subungual hyperkeratosis affecting all 10 fingernails. Fungal microscopy and culture findings were negative. Dermoscopic examination further supported the diagnosis of NLP, with an initial Typical Nail Lichen Planus Severity Index (tNLPSI) score of 152. 17 Based on the refractory history, clinical presentation, and investigative findings, a diagnosis of refractory NLP was established.
Given the treatment history and emerging evidence supporting the use of JAK inhibitors in LP, we initiated therapy with oral abrocitinib at a dose of 100 mg once daily. Clinical and dermoscopic evaluations were performed during the first 6 months. Rapid and substantial clinical improvement was observed. After 2 months of treatment, her tNLPSI score decreased to 76. After 6 months of treatment, both physical and dermoscopic evaluations (Figure 2) showed remarkable improvement in the nail abnormalities. The tNLPSI score further decreased to 18, with smoothing of the nail plate, normal outgrowth from the proximal nail fold, and resolution of erythema and hyperkeratosis. Additionally, her comorbid atopic dermatitis, anxiety, and insomnia improved markedly. The treatment was well tolerated, with no adverse effects reported. Currently, the patient has remained free of significant recurrence for more than 6 months after discontinuation of medication.

Clinical and dermoscopic features of the fingernails in a woman in her late 40s with refractory nail lichen planus before and after treatment with abrocitinib. (a) Before treatment with abrocitinib; (b) after 6 months of treatment with abrocitinib.
Discussion
This case report illustrates that abrocitinib, a selective JAK1 inhibitor, can be an effective and well-tolerated treatment for refractory NLP, particularly in patients who have failed multiple conventional therapies. It also highlights the importance of early intervention with targeted therapies to prevent permanent nail damage and improve quality of life. Our patient, a woman in her late 40s, presented with severe, refractory NLP affecting all 10 fingernails, which had proven resistant to multiple conventional therapies over a 3-year period. The pathogenesis of LP is driven by a T cell–mediated inflammatory response, wherein cytokines such as IFN-γ activate the JAK-STAT pathway. This signaling cascade promotes keratinocyte apoptosis and recruits cytotoxic CD8+ T cells, leading to destruction of the nail matrix.18,19 To contextualize our findings, we reviewed recent literature on the use of JAK inhibitors in isolated NLP (Table 1). Given the refractory nature of her condition and emerging evidence supporting JAK inhibition in NLP, treatment with the abrocitinib (100 mg once daily) was initiated. By competitively inhibiting JAK1, abrocitinib attenuates downstream signaling of key cytokines, including IFN-γ, IL-4, and IL-13, thereby modulating the inflammatory process. Marked clinical improvement was observed within 2 months of therapy, characterized by reduced subungual debris and the emergence of normal nail growth from the proximal nail fold. This rapid response aligns with the central pathogenic role of JAK-STAT signaling in NLP and is consistent with outcomes reported for other JAK inhibitors in similar clinical contexts.
Summary of published cases utilizing JAK inhibitors for nail lichen planus.
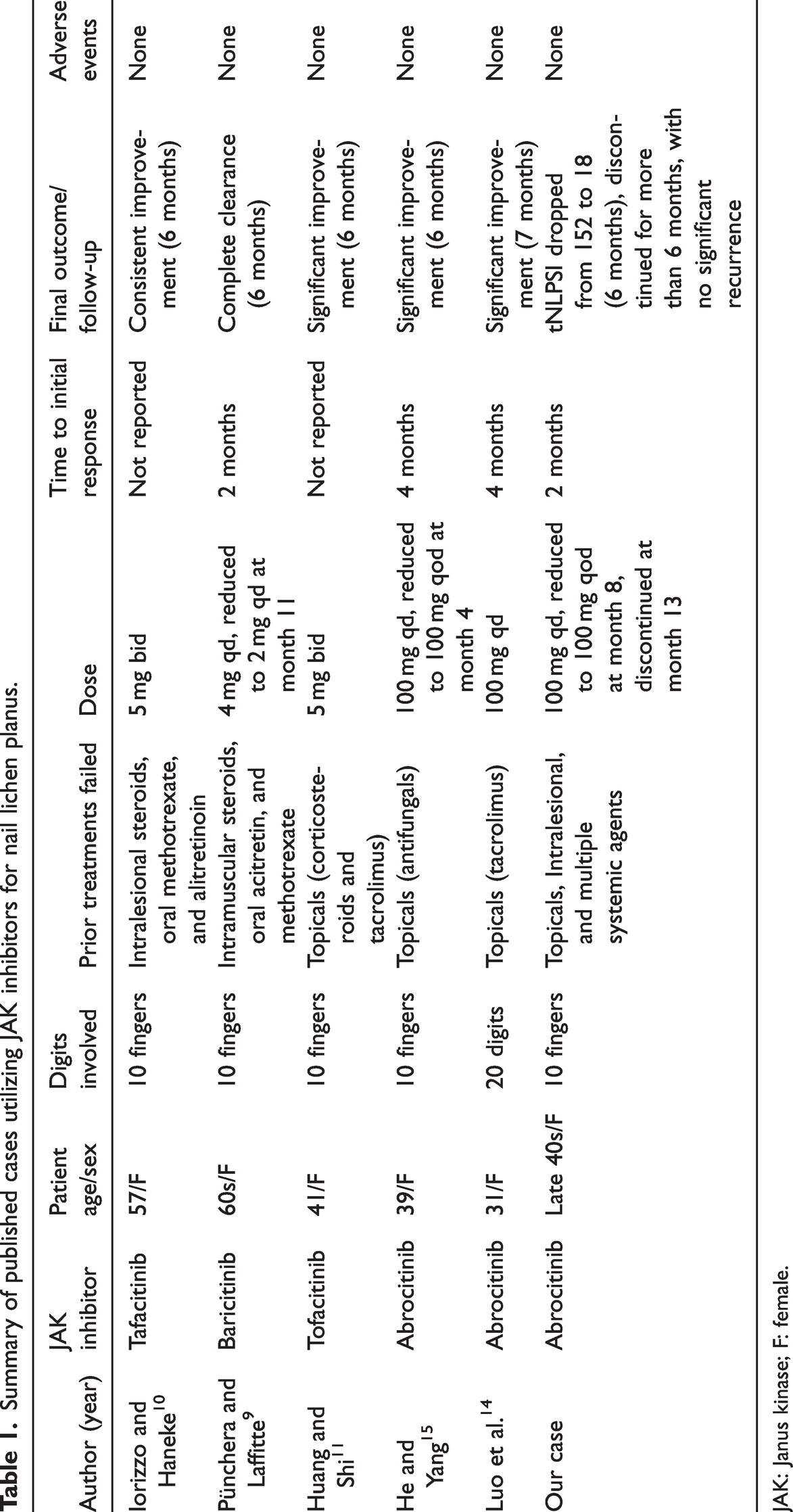
JAK: Janus kinase; F: female.
Comparison with published cases reveals several distinctive aspects of our report. First, the consistency of response across different JAK inhibitors (Table 1) firmly establishes the JAK-STAT pathway as a critical therapeutic target in NLP. However, with respect to efficacy and speed of onset, selective JAK1 inhibitors such as abrocitinib appear to act as rapidly as pan-JAK inhibitors (e.g. tofacitinib) and theoretically offer a superior safety profile by avoiding JAK2/JAK3-related hematological abnormalities. Second, our patient exhibited an exceptionally severe, treatment-resistant phenotype. Although previous cases documented resistance to one or two treatment modalities, our patient failed extensive treatments including topical, intralesional, and systemic agents. The use of a quantitative score (tNLPSI reduction from 152 to 18) provides robust evidence supporting the efficacy of this off-label treatment approach. Furthermore, the complete resolution of her concomitant systemic comorbidities, including atopic dermatitis, anxiety, and insomnia, suggests a broader systemic immunomodulatory benefit of abrocitinib.
Despite the excellent initial response and favorable safety profile, the long-term outlook and practical management of NLP with JAK inhibitors remain uncertain. Because NLP is a chronic inflammatory disease, sudden discontinuation of abrocitinib may precipitate severe relapse. In our case, the patient received 100 mg daily for 8 months. Subsequently, the dose was tapered to 100 mg every other day (qod) as a maintenance phase. Following 13 months of total therapy, the medication was successfully discontinued. She is currently undergoing regular follow-up and remains in complete remission without signs of relapse for more than 6 months after discontinuation of the medication. These findings provide important clinical evidence regarding tapering and withdrawal strategies.
This case provides important evidence that abrocitinib monotherapy can induce rapid and sustained remission in multiply refractory NLP, including cases with extensive nail involvement. The concurrent resolution of systemic comorbidities underscores a potential systemic immunomodulatory benefit beyond localized nail pathology. Early intervention with such targeted therapies may be crucial in preventing irreversible nail damage. However, the generalizability of these findings remains limited by the single-case nature of this report and the relatively short follow-up period. Further prospective studies and larger case series with long-term follow-up are warranted to definitively establish the efficacy, optimal dosing, long-term safety, and durability of response of abrocitinib particularly for NLP as well as to compare it with other available JAK inhibitors for managing this challenging condition.
Conclusions
Abrocitinib demonstrated remarkable efficacy in multiply refractory NLP, yielding significant quantitative improvement (tNLPSI reduction) and functional nail restoration. Its targeted JAK1 inhibition addresses core immunopathogenetic mechanisms and maintains an excellent safety profile. The successful long-term tapering and drug withdrawal strategy observed in this case provides valuable practical insights and addresses a major knowledge gap in NLP management. Further prospective studies and larger case series with long-term follow-up are warranted to definitively establish standardized treatment guidelines, optimal dosing, and long-term maintenance strategies for JAK inhibitors in this challenging condition.
Footnotes
Acknowledgments
The authors thank the patient for consenting to the publication of this case and for her cooperation during the treatment and long-term follow-up.
Author contributions
Conceptualization, Q.H.C.; writing—original draft preparation, L.W.; writing—review and editing, L.F.L.; visualization, L.W.; supervision, X.L. All authors have read and agreed to the published version of the manuscript.
Data availability statement
All data supporting the findings of this study are contained within the article. Deidentified source data (e.g. scale scores and time-stamped toxicology results) can be provided by the corresponding author upon reasonable request, subject to privacy and institutional safeguards. No publicly archived datasets were generated.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Funding
This research received no external funding.
Informed consent statement
Written informed consent was obtained from the patient involved in the study, including consent to publish this case study.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived for this study due to its nature as a single patient, noninterventional case report using fully deidentified clinical information and involving no procedures beyond routine care.