
Abstract
Background
External iliac artery thrombosis is a rare vascular complication that can result in a series of serious adverse outcomes. Existing studies on external iliac artery thrombosis after open reduction of acetabular fracture have primarily focused on the classical ilioinguinal approach. However, despite the increasing use of the para-rectus approach for the management of complex acetabular fractures in recent years, no case of external iliac artery thrombosis following this approach have been reported.
Conclusion
This case represents the first reported instance of external iliac artery thrombosis following acetabular fracture fixation via the para-rectus approach. It underscores that even minimally invasive approaches carry risks of vascular complications. Gentle intraoperative manipulation and meticulous vascular monitoring are essential to prevent such complications. Patient outcomes are closely associated with rapid identification of postoperative vascular abnormalities and timely interventional therapy.
Background
Surgical management of acetabular fractures remains challenging because of their complexity, necessitating the selection of an appropriate surgical approach to optimize outcomes (Table 1). Compared with the traditional ilioinguinal approach, the para-rectus approach has gained widespread adoption because of its minimally invasive nature and direct visualization of the anterior acetabular column. 1 However, even with the para-rectus approach, the risk of postoperative vascular complications persists. To the best of our knowledge, this report describes the first documented instance of external iliac artery thrombosis following acetabular fracture fixation via the para-rectus approach, highlighting the persistent risk of vascular injury despite minimally invasive techniques.
Comparison of surgical approaches for acetabular fractures.
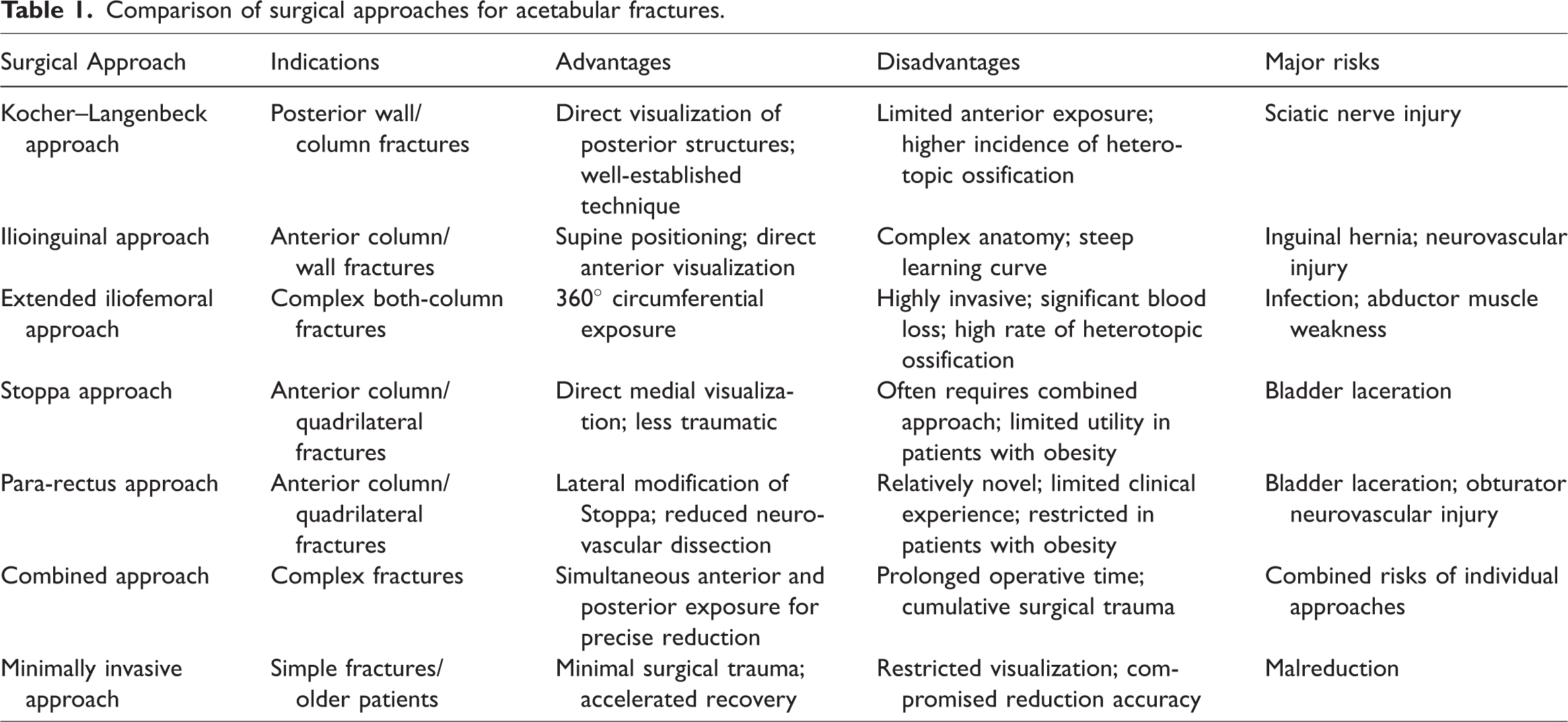
Previous studies have primarily focused on thrombotic complications associated with the ilioinguinal approach, as reported by Langford et al. 2 and Klos et al. 3 However, vascular complications associated with the para-rectus approach remain poorly documented. This case report helps address this gap. The objectives of this report are to enhance awareness of such rare complications and to explore the prevention and management of vascular complications, ultimately improving patient outcomes.
Case presentation
Patient presentation
A 50-year-old female with no significant past medical history presented with a left acetabular both-column fracture and iliac wing fracture (Figure 1) after a fall from a second-floor balcony (approximately 4 m). The patient was admitted to Qingdao Municipal Hospital in July 2024. Due to anemia and suboptimal preoperative status, initial management included symptomatic treatment and supracondylar femoral skeletal traction. No arterial or venous thrombosis was observed on preoperative vascular ultrasound.

Preoperative image: left acetabular both-column fracture and iliac wing fracture.
Surgical intervention
On day 11, open reduction and internal fixation via the para-rectus approach were performed (Figure 2). The surgical technique involved incising the anterior rectus sheath lateral to the rectus abdominis, followed by retroperitoneal exposure and anatomic reduction of the quadrilateral area fractures. Fixation was achieved using an acetabular wing-shaped anatomical plate (Figure 3). The surgery lasted 2 h, and intraoperative assessments revealed good pulsation in the external iliac artery and femoral artery.
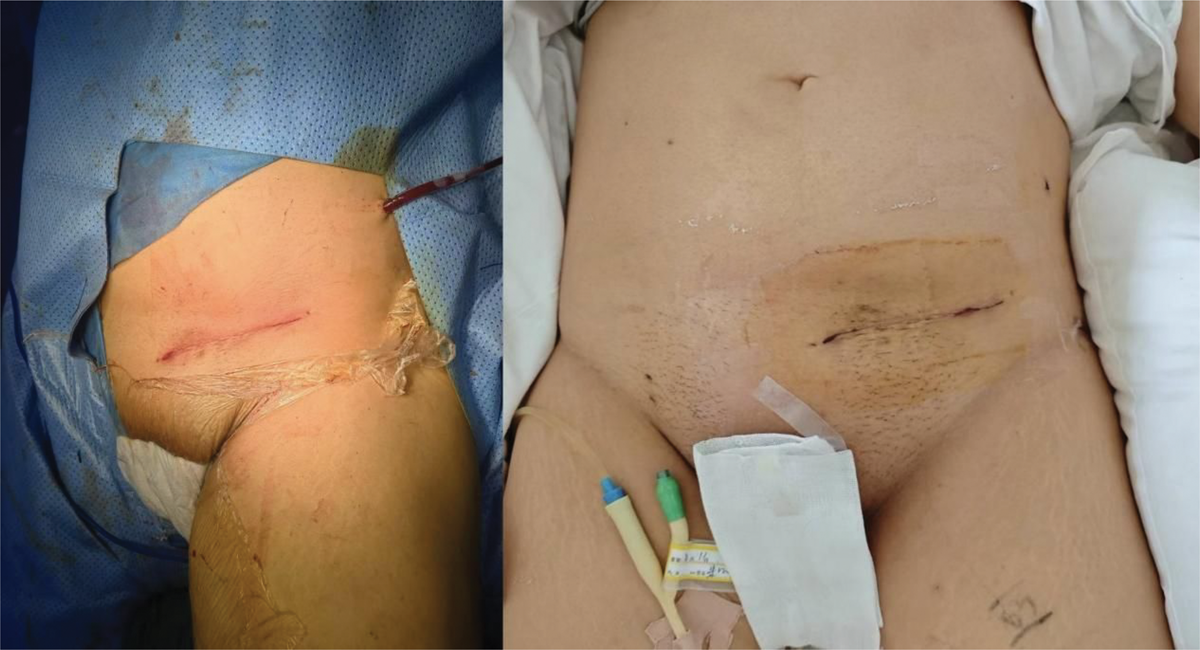
Image of the surgical incision for the para-rectus approach, including intraoperative and postoperative views.

Postoperative image: the fracture was well reduced and fixed with an acetabular wing-shaped anatomical plate.
Postoperative complications and management
One hour postoperatively, the patient developed a cool left lower limb temperature, mottled skin discoloration, and diminished dorsalis pedis artery pulsation, indicating lower limb ischemia. Despite intravenous papaverine, the symptoms persisted. Computed tomography angiography (CTA) revealed nonvisualization of the left external iliac artery and faint opacification of the femoral and deep femoral arteries (Figures 4 and 5). Three hours after the initial surgery, an emergency interventional procedure was performed. A vascular sheath was inserted via left femoral artery puncture, and under angiographic guidance, a thrombectomy catheter was advanced to the thrombus segment of the external iliac artery. Approximately 10 cm of dark-red, organized thrombus was successfully retrieved through negative-pressure aspiration and catheter withdrawal (Figure 6), and postprocedural angiography confirmed restored patency. Postoperative vascular ultrasound revealed unobstructed blood flow in the lower-extremity vessels. The patient recovered fully and was discharged uneventfully.

CTA revealed nonvisualization of the left external iliac artery and faint opacification of the femoral and deep femoral arteries. CTA: computed tomography angiography.

Axial CT images of bilateral external iliac arteries. (A) Preoperative; (B) postoperative, proximal part of the thrombus; and (C) postoperative, distal part of the thrombus. CT: computed tomography.

Thrombus removed by interventional operation.
Discussion
As a classic example of high-energy trauma, the surgical management of acetabular fractures remains one of the challenges in orthopedic surgery. 4 In recent years, the para-rectus approach has been increasingly used in acetabular fracture surgery because of its minimally invasive nature and direct anatomical exposure. 5 However, this case highlights that even with minimally invasive approaches, the risk of postoperative vascular complications cannot be overlooked.
External iliac artery thrombosis is a rare but critically severe complication following acetabular fracture surgery and may be associated with multiple factors. Acetabular fractures frequently occur with direct vascular injury or traction to pelvic vessels, resulting in endothelial damage and subsequent thrombus formation. 6 Despite being minimally invasive, the para-rectus approach may still result in indirect injury or compression of the external iliac artery and its branches during surgical manipulation. Additionally, prolonged postoperative bed rest and restricted limb mobility may contribute to blood stasis, further increasing the risk of thrombosis. 7 In this case, the patient developed coldness and mottled skin discoloration in the left lower limb within 1 h postoperatively, suggesting rapid-onset vascular compromise, likely associated with the potential effects of intraoperative manipulation on the blood vessels.
This case underscores the importance of gentle intraoperative techniques and vascular monitoring. Although the para-rectus approach offers a relatively clear anatomical visual field, excessive traction or compression on the external iliac artery and its branches must be avoided. Direct vascular contact should be minimized during the procedure, particularly during exposure of the quadrilateral area and fracture reduction. Intraoperative assessment of external iliac and femoral artery pulsations is essential, with immediate angiography or ultrasonography recommended when abnormalities arise. Notably, despite normal intraoperative arterial pulsations in this case, external iliac artery thrombosis still occurred, indicating limitations in intraoperative vascular evaluation and emphasizing the need for continued postoperative surveillance.
Prompt recognition and intervention are critical for prognosis. 8 In this patient, early signs of external iliac artery thrombosis, including coolness, mottled skin, and weak dorsalis pedis pulses, manifested within 1 h postoperatively. Suspected vascular complications warrant immediate CTA for diagnosis, followed by urgent endovascular intervention. 9 In this case, CTA confirmed the diagnosis within 2 h postoperatively, and emergency thrombectomy successfully restored perfusion, thereby avoiding limb ischemia. This outcome highlights the importance of rapid response and timely treatment.
This case serves as a reminder that vascular complications may persist even with minimally invasive approaches. Comprehensive preoperative vascular assessment, including ultrasonography and a detailed history of vascular disease, helps identify high-risk patients. Meticulous intraoperative technique and close postoperative circulatory monitoring are imperative. Early postoperative activity and anticoagulant therapy may also help reduce the incidence of vascular complications. Future studies should focus on optimizing surgical techniques and developing preventive strategies for vascular complications in para-rectus approach surgeries.
Conclusion
This case represents the first reported instance of external iliac artery thrombosis following acetabular fracture repair via the para-rectus approach, emphasizing that minimally invasive techniques do not eliminate vascular risks. Gentle intraoperative handling, real-time vascular assessment, and prompt postoperative intervention are crucial for complication prevention and outcome improvement. Clinicians should enhance vigilance for postoperative vascular complications and strengthen postoperative monitoring and management, ultimately improving patient outcomes in the management of acetabular fractures.
Footnotes
Author contributions
Wenlian Song and Tengbo Yu conceived and designed the study. Kecheng Lao performed the surgery and collected the clinical data. Wenlian Song analyzed the data and wrote the main manuscript text. Kecheng Lao prepared Figures 1 to ![]() . Jinli Chen provided critical feedback and helped shape the research, analysis, and manuscript. All authors reviewed and approved the final manuscript.
. Jinli Chen provided critical feedback and helped shape the research, analysis, and manuscript. All authors reviewed and approved the final manuscript.
Declaration of conflicting interests
We have deidentified all patient details.
Ethical approval was obtained from the Ethics Committee of Qingdao Municipal Hospital.
Informed consent was obtained from the patient for the publication of this case report.
The authors declare that they have no competing interests.
The reporting of this study conforms to CARE guidelines. 10
Funding
The work is supported by the Shandong Provincial Natural Science Foundation Project (ZR2023MH205).