
Abstract
Horticultural therapy is a plant-based therapeutic intervention that has shown promise in alleviating depressive symptoms and supporting clinical rehabilitation. This scoping review synthesizes current evidence on the use of horticultural therapy for individuals diagnosed with depression. A systematic search across eight Chinese and international databases identified 1044 studies, of which 18 met the inclusion criteria. These studies were conducted in diverse settings, including hospitals, nursing homes, schools, and community centers. Interventions ranged from active participation (e.g. planting and floral arrangement) to passive engagement (e.g. nature walks). Outcomes included psychological indicators such as depression and anxiety levels and physiological markers such as salivary cortisol and cardiovascular response. Most studies reported positive effects on mood and quality of life. However, variations in intervention design, duration, frequency, and facilitator qualifications limited comparability. This review highlights horticultural therapy as a promising complementary approach for depression rehabilitation while emphasizing the need for standardized protocols and culturally adapted applications in future research.
Introduction
Depression is one of the most prevalent psychological disorders that frequently co-occurs with chronic physical illnesses; its global prevalence is approximately 4.4%. It is a leading contributor to both mental and physical disability worldwide. 1 According to the United Nations report, “Depression: A Global Crisis”, depression was the third leading global cause of disease burden in 2004 and is projected to rank first by 2030. 2 Data from a 2019 study has indicated that the prevalence of depression among older adults in China ranges from 3.7% to 34.8%. 3
Common symptoms of depression include persistent sadness, loss of interest, fatigue, and cognitive impairment. These symptoms can lead to serious consequences such as exacerbation of comorbid conditions, increased caregiver burden, and elevated suicide risk. 4
Depression imposes substantial emotional and functional burdens on both patients and caregivers. Only approximately one-third of patients experience remission during their initial treatment, and relapse rates remain high. 5 Consequently, most patients undergo prolonged and multifaceted treatment, which may include pharmacological interventions (e.g. use of antidepressants); talking therapies (e.g. cognitive behavioral therapy); physical activity; and nature-based interventions, such as horticultural therapy (HT).6,7
Although pharmacological treatment has long been considered the primary intervention for depression, non-pharmacological approaches such as cognitive-behavioral therapy and physical activity are now widely recognized as effective first-line treatments. In addition, complementary interventions, including HT, are increasingly employed, particularly for patients who prefer non-medication-based strategies or for whom pharmacotherapy is contraindicated.
HT, as a form of non-pharmacological intervention, is drawing growing interest in the treatment of depression. It is typically defined as engagement in gardening activities under the guidance of a registered horticultural therapist with the aim of achieving therapeutic, rehabilitative, or vocational goals.8–10 Over recent decades, growing awareness of nature’s restorative potential has brought increased empirical attention to HT. Prior studies have supported its effectiveness across diverse populations, including healthy individuals 11 as well as patients with dementia, 12 schizophrenia, 13 and individuals exhibiting depressive symptoms. 14 Recent systematic reviews and meta-analyses have further supported the efficacy of HT in improving mental health outcomes, particularly among individuals with depression and anxiety. For example, Wood et al. 15 reported large and significant effects of social and therapeutic horticulture on depression and moderate effects on anxiety across 17 studies. Similarly, Pant,iru et al. 16 reported that gardening interventions significantly improved well-being and quality of life in both general and vulnerable populations. These findings reinforce the therapeutic potential of HT and underscore the need for targeted reviews focusing on clinically diagnosed patients and optimal implementation parameters.
HT activities can generally be categorized into two types, participatory and observational. Participatory activities involve active engagement in gardening tasks such as planting, watering, pruning, and harvesting, which are believed to promote physical movement, sensory stimulation, and a sense of accomplishment. In contrast, observational activities refer to passive interaction with nature, such as viewing gardens, walking through green spaces, or attending guided horticultural sessions without direct physical involvement. Both formats have demonstrated therapeutic potential; however, their mechanisms of action and outcomes may differ.17,18 Recent studies15,19,20 have shown that HT significantly reduces symptoms of depression and anxiety, improves mood and cognitive function, and enhances social interaction and self-efficacy. These benefits are linked to physical movement, sensory stimulation, and the emotional reward of nurturing living plants.
Notably, the effectiveness of these interventions is significantly influenced by environmental settings, the nature of these activities, and duration of engagement. 21 Research suggests that interventions conducted in natural outdoor environments or immersive green spaces yield stronger psychological benefits than those performed in indoor or urban settings.22–24 Common activities such as planting, flower arranging, and nature-based crafts have been associated with improvements in mood, stress reduction, and social engagement. 5 In terms of duration, short-to-medium–term programs (typically 11–20 sessions or 100–500 min in total) appear most effective, with diminishing returns observed for longer interventions. 25 These findings underscore the importance of tailoring HT programs to specific populations and contexts to maximize therapeutic outcomes.
Although several systematic reviews and meta-analyses have explored the impact of HT on mental health, important gaps remain. For example, Xu et al. 25 focused on older adults with depression and confirmed the overall effectiveness of HT; however, they did not examine the variations in intervention format or setting. Sin et al. 26 and Wood et al. 15 evaluated the benefits of horticultural activities for general populations, emphasizing improvements in well-being and stress reduction; however, they offered limited insights into clinical depression and structured therapeutic design. Kuo et al. 27 conducted a meta-analysis of randomized controlled trials (RCTs) targeting individuals with depressive disorders; however, they did not differentiate between participatory and observational formats and did not assess the influence of environmental context or duration. In contrast, the present review aimed to map current evidence with a specific focus on how HT is applied in depression care and identify knowledge gaps related to activity type, therapeutic setting, and optimal intervention duration.
Thus, this scoping review aimed to systematically evaluate the current body of literature to clarify the effectiveness of HT in alleviating depressive symptoms and identify optimal intervention parameters, including environmental settings, activity types, and duration for future research and clinical applications. A targeted literature search was conducted across eight Chinese and international databases to ensure comprehensive coverage of relevant studies.
Materials and methods
Research questions
Based on a preliminary literature review, the following research questions were formulated: (a) What are the intervention methods, specific content, and outcome indicators of HT for patients with depression? and (b) What implementation characteristics (e.g. environmental settings, activity types, and duration) influence the effectiveness of HT in this population?
Search strategy
A systematic search was conducted across eight Chinese and English databases, including the China National Knowledge Infrastructure (CNKI), Wanfang, Chinese Science and Technology Journal Database (VIP), Chinese Biomedical Literature Database (CBM), PubMed, Web of Science Core Collection, Embase, and Cochrane Library. In addition to the eight core databases, supplementary searches were conducted in PsycINFO, Scopus, and Google Scholar to capture relevant psychological and interdisciplinary studies. Manual searches of reference lists and grey literature (e.g. unpublished reports, theses, and conference proceedings) were also performed to ensure comprehensive coverage, according to the best practices outlined in recent reviews of HT interventions. The time frame was from database inception to 31 March 2025. A combination of subject terms and free-text terms was employed, using the Boolean operators “and” and “or” to build flexible search strategies tailored to each database.
The complete search strategies used for each database, including all terms and Boolean combinations used, are provided in Appendix A to ensure transparency and reproducibility. Additionally, manual searches of the reference lists of the included studies were performed to identify any potentially relevant literature not captured in the initial database queries.
Inclusion and exclusion criteria
Inclusion criteria
Studies were included if they met the following criteria, based on the “Population, Concept, Context” (PCC) framework recommended for scoping reviews by the Joanna Briggs Institute (JBI). 28
Population: Adults (aged ≥18 years) with a confirmed diagnosis of depression established by a qualified health practitioner (e.g. psychiatrist, clinical psychologist, or general physician) using standardized criteria such as the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and International Classification of Diseases, 10th revision (ICD-10) or validated diagnostic tools (e.g. Patient Health Questionnaire-9 (PHQ-9), Hamilton Depression Rating Scale (HAMD)).
Concept: Structured HT interventions designed with therapeutic intent, involving active engagement in plant-based activities (e.g. planting, garden maintenance, and nature-based crafts) delivered by a trained horticultural therapist or under professional supervision.
Context: Clinical rehabilitation or intervention phase referred to any structured therapeutic period in which HT was integrated into a formal treatment or recovery plan, including inpatient, outpatient, and community-based settings.
Exclusion criteria
Studies were excluded if they met any of the following conditions: (a) articles not in Chinese or English; (b) conference abstracts, editorials, and other sources lacking full-text access or sufficient methodological detail for data extraction; (c) duplicate publications; (d) articles that mentioned HT but lacked sufficient detail on the intervention, including the type of activities conducted, duration and frequency of sessions, therapeutic intent, delivery personnel, or setting; and (e) studies without clear distinction of HT from other therapeutic components, making replication or attribution of outcomes impossible.
Study selection and data extraction
All retrieved references were imported into EndNote 21 software for management. Duplicate entries were removed using built-in tools. Two evidence-based trained researchers independently screened the titles and abstracts according to the inclusion and exclusion criteria. Full texts were then reviewed to determine final eligibility.
Data were extracted using a pre-defined standardized form by two researchers independently. Extracted data included information about the first author, publication year, country, study population, article type, sample size, intervention type, outcome indicators, and assessment tools. Discrepancies were resolved through discussion or consultation with a third reviewer.
This scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist 29 to ensure transparency and methodological rigor. The study selection process is illustrated in the PRISMA-ScR flow diagram (Figure 1).

Flow diagram of the literature selection process.
Intervention setting classification
To facilitate comparative analysis, intervention settings were categorized into two broad types based on their operational context and population characteristics: (a) institutional settings, including hospitals, nursing homes, and university campuses, typically characterized by structured environments and professional oversight and (b) community-based settings, encompassing community centers and public spaces, often defined by informal engagement and broader public accessibility.
Results
Literature screening results
In total, 1044 articles were initially retrieved, including 563 from Chinese databases and 449 from English databases. An additional 32 articles were identified through guideline-related websites, including the World Health Organization (WHO), National Institute for Health and Care Excellence (NICE), Chinese Clinical Guideline Network (CCGN), and American Psychiatric Association (APA) platforms. After removing 232 duplicates using EndNote 21, 812 unique records remained. Title and abstract screening resulted in the exclusion of 726 irrelevant articles, leaving 86 for full-text review. Ultimately, 68 articles were excluded due to the following reasons: (a) insufficient or unclear description of HT interventions (n = 28); (b) study populations not meeting inclusion criteria (e.g. not diagnosed with depression) (n = 24); and (c) lack of full-text access (e.g. conference abstracts and editorials) and language limitations (non-English/Chinese) (n = 16). In addition to database searches, guideline-related websites (e.g. national clinical practice portals and professional HT associations) were screened to identify potentially relevant studies and grey literature. In total, 18 studies were included in the final analysis.
A flow diagram depicting the literature selection process is presented in Figure 1.
Characteristics of the included studies and interventions
The 18 included studies were published from the time of database inception to 2025, all involving patients diagnosed with depression. Study types consisted primarily of RCTs, with some quasi-experimental and cross-sectional designs. Sample sizes varied considerably, ranging from <30 participants to >150. Eleven studies targeted general depression populations, while seven focused on patients with comorbid conditions such as stroke (n = 3), malignant tumors (n = 1), hypertension (n = 1), anxiety disorders (n = 1), or cognitive impairment (n = 1). Most groups included both male and female participants.
Study settings included hospitals, nursing homes, university campuses, and community-based environments. Specifically, nine30–39 studies were conducted in medical institutions, two38,40 in nursing homes, three41–43 on university campuses, and one 44 in a community setting. Additionally, one study employed virtual reality (VR) to simulate a therapeutic garden environment. 45
Of the 18 included studies, 17 involved participatory horticultural activities such as planting, harvesting, floral arrangement, and mini-landscape design. These interventions emphasized hands-on engagement with plants and natural materials. In contrast, one study 46 used an observational approach where participants engaged in guided walking through green spaces without direct horticultural activity. This intervention focused on passive nature exposure as a therapeutic mechanism. Intervention durations ranged from 4 to 16 weeks, with session frequencies ranging from 1 to 3 times per week. Each intervention session lasted 30–120 min.
Detailed characteristics of the included studies are provided in Table 1. Details of the HT interventions in the included studies are summarized in Table 2.
Basic characteristics of the included studies (n = 18).
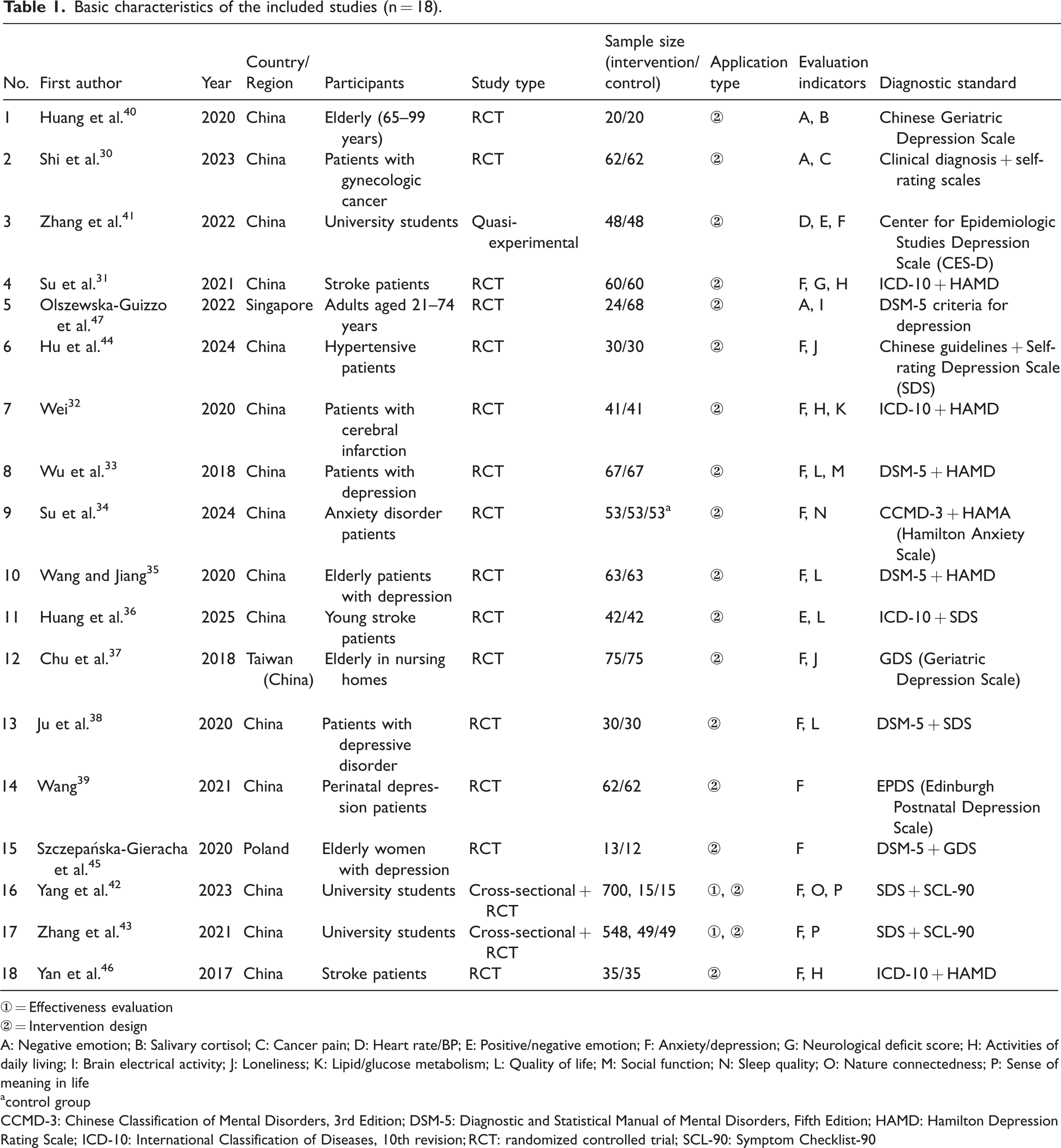
① = Effectiveness evaluation
② = Intervention design
A: Negative emotion; B: Salivary cortisol; C: Cancer pain; D: Heart rate/BP; E: Positive/negative emotion; F: Anxiety/depression; G: Neurological deficit score; H: Activities of daily living; I: Brain electrical activity; J: Loneliness; K: Lipid/glucose metabolism; L: Quality of life; M: Social function; N: Sleep quality; O: Nature connectedness; P: Sense of meaning in life
control group
CCMD-3: Chinese Classification of Mental Disorders, 3rd Edition; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; HAMD: Hamilton Depression Rating Scale; ICD-10: International Classification of Diseases, 10th revision; RCT: randomized controlled trial; SCL-90: Symptom Checklist-90
Horticultural therapy intervention details in the included studies (n = 18).

EEG: electroencephalogram; FAA: frontal alpha asymmetry; GAD: generalized anxiety disorder; VR: virtual reality
Most participants had mild to moderate depression, and all interventions were supervised by professionals such as researchers, rehabilitation specialists, or certified horticultural therapists. Two studies also conducted cross-sectional surveys in addition to performing interventions.42,43
In addition, Table 2 summarizes the theoretical mechanisms proposed to explain these effects. These include biophilia and nature connectedness, stress reduction, sensory stimulation, emotional regulation, and neurobiological pathways such as endorphin release and monoamine modulation. Such mechanisms help contextualize how different horticultural activities may contribute to psychological improvement across diverse populations.
Summary of findings
Of the 18 studies, those conducted in medical institutions (n = 9)30–39 reported more consistent and statistically significant improvements in depression scores compared with those conducted in community settings (n = 1), suggesting greater efficacy of HT administered in structured clinical environments. Additionally, 17 studies employed participatory activities, and all reported positive outcomes, whereas the single observational study 47 demonstrated limited effect size. These findings suggest that active engagement enhances therapeutic outcomes. However, due to heterogeneity in study design and outcome measures, these conclusions should be interpreted with caution.
The included studies applied HT to alleviate depressive symptoms through diverse designs and outcome measures. Most studies reported statistically significant improvements in depression, anxiety, and overall psychological well-being.
Common benefits reported across the included studies were reduced negative emotions, improved sleep quality, enhanced social functioning, and an increased sense of meaning and nature connectedness. Outcome measures varied across studies, including standardized psychological scales (e.g. HAMD, Beck Depression Inventory (BDI), and Self-Rating Depression Scale (SDS)), physiological indicators (e.g. salivary cortisol and electroencephalogram (EEG)), and quality-of-life assessments. These findings support the therapeutic potential of horticultural interventions in clinical and rehabilitative contexts.
Discussion
These findings are consistent with prior research indicating that nature-based interventions can positively influence mental health. For example, Soga et al. 48 found that gardening activities were associated with reductions in depression and anxiety levels across diverse populations. Similarly, Clatworthy et al. 49 emphasized the therapeutic potential of HT in enhancing mood and social engagement. Our synthesis adds to the growing body of evidence by highlighting specific characteristics such as setting, activity type, and duration that may influence intervention outcomes.
This study presents a qualitative synthesis of evidence supporting the positive impact of HT on patients with depression. Prior research has indicated that horticultural activities can improve mood and reduce stress levels. 50 Claims regarding self-confidence, self-esteem, and physical functioning were removed due to lack of supporting evidence. During intervention sessions, patients are often willing to share and discuss their positive experiences, which may contribute to improved social interaction and a stronger sense of community.
Medical institutions demonstrated greater efficacy than community settings
Environmental settings may play a significant role in the effectiveness of interventions, consistent with previous findings. 51 Among the 18 studies, 9 were conducted in medical institutions, including hospitals and nursing homes. These studies reported more consistent and significant improvements in depression-related outcomes compared with those conducted in community settings, suggesting an influence of structured environments and professional support. Descriptive synthesis of the included studies suggested that interventions conducted in medical institutions yield more consistent therapeutic outcomes than those conducted in community settings, potentially due to structured environments and professional facilitation. Our results suggest that HT administered in care institutions is more effective than that administered in community settings. This observation is supported by the fact that eight of the nine studies conducted in medical institutions reported statistically significant improvements in depression scores, while the single community-based study lacked quantitative outcome measures. Possible contributing factors include the following: (a) patients in institutional settings may receive more structured support and supervision and (b) hospitals and nursing homes often have access to professional staff trained in therapeutic care. These interpretations remain speculative and should be explored further. Possible explanations include the following: (a) patients in medical institutions often exhibit a stronger desire for recovery, which positively influences therapeutic outcomes and (b) medical facilities such as hospitals and nursing homes generally provide more professional staff and structured healthcare support than community settings. These factors support the adoption of long-term and regular horticultural interventions in institutional environments.
Therapeutic outcomes appear closely linked to environmental design and interaction with nature; therefore, future research should aim to systematically describe therapeutic environments and quantitatively assess their influence on outcomes.
Participatory activities were more effective than observational activities
The type of activity was observed to influences the efficacy of HT. Of the 18 included studies, 17 employed participatory horticultural activities, which were consistently associated with improvements in depression, anxiety, and quality of life. The single observational study that involved walking in green spaces reported modest mood enhancement but did not demonstrate significant changes in standardized depression scores. Descriptive comparison suggests that participatory activities are more effective in reducing depressive symptoms than observational ones as studies involving hands-on tasks reported improvements across psychological indicators more frequently. Patients who engaged in activities such as planting and floral design tended to exert themselves more physically compared with those in observational settings where physical engagement was limited. Participatory tasks may strengthen physical functioning and improve overall health while offering emotional relief through enjoyment and immersion. 36
Moreover, patients with depression may experience several tactile sensations during hands-on tasks (e.g. handling plants of different textures and firmness), which could stimulate sensory and motor areas of the brain, potentially inducing comfort and emotional regulation.
Duration and frequency of intervention
The duration and frequency of horticultural interventions varied widely among included studies, ranging from 4 to 16 weeks in duration and from 1 to 3 sessions per week in frequency. Our descriptive synthesis suggests that an intervention period of 4–8 weeks with a frequency of once per week is beneficial as this duration allows participants to engage with plant growth cycles and maintain therapeutic interest. This observation aligns with results reported by Xu et al. 25 and Kuo et al. 27 who found significant effects, regardless of intervention duration. However, current evidence is insufficient to determine an optimal range, and further controlled studies are needed to validate these parameters. This timeline allows participants to observe a full plant growth cycle and develop a deeper connection with the activity. In contrast, excessively long durations may lead to aesthetic fatigue and reduced novelty, limiting continued improvement. Current evidence on duration–effect relationships remains limited, and further research with scientifically designed long-term interventions is needed.
Most sessions lasted 30–60 min. Extending the activity duration beyond 2 h did not appear to provide additional benefits. Notably, some studies have reported that even short-term gardening sessions can alleviate symptoms of depression and anxiety.
Study limitations
This review has certain limitations that should be acknowledged. First, only articles published in Chinese and English were included, which may have led to the omission of relevant studies in other languages. Second, although intervention settings varied across studies, including hospitals, nursing homes, university campuses, and community spaces, we classified them into two broad categories: medical institutions (e.g. hospitals, nursing homes, and rehabilitation centers) and community settings (e.g. university campuses, public parks, and local programs). This classification was based on the presence or absence of formal healthcare infrastructure. However, we recognize that this grouping may have oversimplified contextual differences and masked nuances in therapeutic delivery and support systems. Other potential factors such as participant sex and the background of the intervention providers (e.g. researcher, therapist, nurse, and horticulturalist) were not analyzed in depth. Future research should further explore the impact of these variables.
Conclusion
Based on an objective analysis of 18 selected studies, this scoping review suggests that HT possesses therapeutic potential for alleviating the symptoms of depression. However, due to variability in study designs, settings, and outcome measures, these findings should be interpreted cautiously. The reviewed literature highlights the possible benefits of diverse horticultural interventions, differing in environment, activity type, and duration.
Interventions delivered within medical institutions, including hospitals and nursing homes, were more consistently linked to improvements in depression-related outcomes compared with those implemented in community settings. This observation may be influenced by the structured environments and availability of professional support in institutional contexts. However, no statistical comparison was performed, and this finding should be interpreted cautiously.
Participatory activities, including planting, harvesting, and floral arrangement, were more commonly linked to reductions in depressive symptoms than observational approaches. These hands-on tasks may promote emotional engagement and sensory stimulation, contributing to therapeutic effects. Again, this conclusion is based on descriptive patterns rather than quantitative analysis.
Regarding environmental settings, interventions conducted in medical and care institutions yielded more effective outcomes. Participatory activities yielded better results than observational ones. In terms of duration, programs lasting 4–8 weeks tended to produce more favorable outcomes.
Nevertheless, rigorously designed studies should be conducted in the future to identify environmental conditions and therapeutic protocols that maximize the effectiveness of HT for depression. Future research should also focus on the standardization of intervention protocols and development of validated evaluation tools to guide clinical practice.
Footnotes
Acknowledgements
The authors would like to thank Shibei Hospital of Jing’an District and Shanghai Tenth People’s Hospital for their institutional support during the study.
This manuscript was language-polished using artificial intelligence (AI)–assisted tools.
Author contributions
The authors confirm contribution to the paper as follows: GONG Yuehua and Yan Liyan contributed to study conception and design; Yan Liyan performed data collection; GONG Yuehua, Shen Haijian, and Zhu Xiaoping were responsible for analysis and interpretation of the results; and Yan Liyan and Zhu Xiaoping prepared the draft of the manuscript. All authors reviewed the results and approved the final version of the manuscript.
Data availability statement
All data generated or analyzed during this study are included in this published article. Further details are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that they have no conflicts of interest to report regarding the present study.
Funding
This research was supported by the following grants: Health and Wellness Scientific Research Project (2025 HL04), Jing’an District, Shanghai; Medical Advantageous Specialty Development Program (2024ZB02), Jing’an District, Shanghai; and Key Supported Discipline Development at Shibei Hospital (2025SBFC01), Jing’an District, Shanghai; and Scientific Research Project of Shanghai Jing’an District Health Commission (2025 HL04).