
Abstract
Background
This study examined disease-specific quality of life among people living with chronic hepatitis B virus infection in northern Ghana, where the condition remains highly endemic.
Method
Using a cross-sectional design, 264 individuals with chronic hepatitis B virus infection were recruited from 1 regional hospital and 3 district hospitals. Data were collected through structured interviews using the validated hepatitis B virus quality of life (HBQoL) instrument and analyzed using descriptive statistics and logistic regression.
Result
Participants had a mean age of 38 years (±16.5), with a nearly equal sex distribution. The overall global HBQoL mean score was 63.6 (±20.0), reflecting a moderate quality of life. Regression analysis identified age, hepatitis B virus profile, and the presence of complications as significant predictors. Each additional year of age increased the odds of better quality of life by 2.8% (odds ratio = 1.028, p = 0.002). Hepatitis B envelope antigen negativity was inversely associated with high quality of life (odds ratio = 0.344, p = 0.013). Additionally, the absence of hepatitis B virus complications was associated with lower odds of good quality of life in this population (odds ratio = 0.300, p = 0.001).
Conclusions
The findings suggest that psychosocial and clinical interventions should complement biomedical care. Addressing the unique quality of life challenges of people living with the hepatitis B virus is essential for holistic management in Ghana and similar settings.
Introduction
Hepatitis B virus (HBV) infection remains a major global public health concern and is one of the leading causes of chronic liver disease worldwide.1,2 An estimated 254 million people live with chronic HBV infection globally, 3 with the highest burden concentrated in sub-Saharan Africa and parts of Asia. 4 Ghana, similar to many countries in West Africa, is classified as highly endemic for HBV, with prevalence estimates in the general population ranging from 8% to 12% and beyond.5,6 In northern Ghana, the prevalence is particularly high, and socioeconomic inequalities, limited access to health services, and low awareness further compound the challenges of HBV prevention and control. 7
Despite the availability of an effective vaccine and evidence-based treatment options, 8 the burden of chronic HBV remains substantial. Many infected individuals are unaware of their status, and those who are diagnosed often face challenges related to stigma, limited access to antiviral therapy, and inadequate follow-up care. 9 In endemic communities where knowledge and awareness of HBV are often low, people living with the infection frequently struggle to access accurate information, timely diagnosis, and consistent clinical management.
Beyond clinical outcomes, living with chronic HBV has profound implications for individuals’ psychological and social well-being. 10 People diagnosed with HBV often report fear of disease progression, anxiety about long-term health outcomes, worry about infecting family members, and feelings of isolation due to the stigma attached to HBV.10–12 In many settings, misconceptions about HBV transmission can lead to discrimination at the community, workplace, and household levels, further undermining the quality of life (QoL) of those affected. 13
Although numerous studies in Ghana7,14–16 and across sub-Saharan Africa17–19 have documented the epidemiology, risk factors, and treatment gaps associated with HBV, relatively few have explored how the infection affects patients’ day-to-day well-being in a holistic sense.
According to the World Health Organization (WHO), QoL is defined as an individual’s perception of their position in life within the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. 20 The WHO views QoL as a broad, multidimensional concept that integrates a person’s physical health, psychological state, level of independence, social relationships, personal beliefs, and relationship to key features of their environment. Health-related QoL (HRQoL) is a narrower concept that focuses specifically on how health status, illness, or medical treatment affects a person’s ability to live well. In short, QoL represents the broader picture, whereas HRQoL reflects the health-focused component of that picture.21,22 As such, HRQoL is an important indicator for understanding the broader impact of chronic illnesses and for guiding the development of supportive care and patient-centered interventions.
Two well-documented approaches exist for measuring HRQoL: generic (or global) measures and disease-specific measures. 23 Unlike generic instruments, disease-specific HRQoL tools are more sensitive, responsive, and clinically relevant for capturing how a particular condition uniquely affects individuals’ daily lives, making them especially valuable for patient-centered care and research compared with generic instruments. 24 In the context of HBV, a disease-specific HRQoL measure incorporates key dimensions such as anxiety about viral replication, fear of infectivity, experiences of stigma, and feelings of vulnerability.25,26
Fu et al., 24 in their systematic review, reported fewer HBV HRQoL studies in sub-Saharan Africa than in Western countries. Most of these studies relied predominantly on generic HRQoL instruments to assess the well-being of people living with HBV.24,27,28 This reliance on generic measures risks overlooking critical HBV-specific concerns, resulting in an incomplete understanding of the true burden of the disease on patients’ lives. Consequently, the absence of nuanced, condition-specific insights limits the capacity of health systems to design comprehensive interventions that address not only the biomedical aspects of care but also the psychological and social challenges faced by people living with HBV, particularly in under-resourced endemic communities.
To address this gap, the present study applied a validated HBV disease-specific HRQoL instrument to assess the well-being of people living with chronic HBV in endemic communities in northern Ghana. By focusing on HBV disease-specific aspects of QoL, this research aimed to generate more accurate and meaningful evidence on how HBV affects the daily experiences of affected individuals in these communities.
Methods
Study design
A cross-sectional design is well-suited for this type of research because it allows the researcher to measure HBV disease-specific QoL and examine associations between sociodemographic, clinical, and psychosocial factors and the QoL at a single point in time. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 29
Study area/setting
The study was conducted in the northern region of Ghana, which is one of the 16 administrative regions of the country. The region is predominantly rural and is characterized by dispersed settlements, limited infrastructure, and significant socioeconomic challenges compared to the southern parts of the country. The northern region faces persistent challenges related to poverty, limited access to quality healthcare, and lower levels of health literacy, all of which influence health-seeking behaviors and disease outcomes. 30 Available estimates show that the northern region has the second-highest prevalence of HBV infection in Ghana, with a reported prevalence of 21.6%. 7 The combination of low awareness, stigma associated with HBV, and constrained health system resources makes the northern region a critical setting for understanding the broader impacts of chronic HBV infection on QoL in an endemic context. The study was conducted in four health facilities in the northern region, namely Northern Regional Hospital, Gushegu Municipal Hospital, Karaga District Hospital, and Tamale West Hospital. All these health facilities have an approximate bed capacity of 50–150 and a daily outpatient department (OPD) attendance of 70–150. These secondary-level facilities provide 24-h services to clients and offer medical, surgical, obstetrics and gynecology and other specialist services. The main HBV-related interventions undertaken in these settings include voluntary testing and prevention of mother-to-child transmission of HBV, which are integrated into antenatal, delivery, and postnatal services.
Study population
The study population consisted of all individuals diagnosed with HBV infection and residing in the northern region of Ghana. The inclusion criteria were having received an official HBV diagnosis with an HBsAg-positive test result ≥12 months prior to the study, reporting to the selected hospitals for review or medication refills, and/or being admitted with HBV-related disorder. Patients who were coinfected with hepatitis C and D viruses, those who were coinfected with human immunodeficiency virus, and those who were unable to complete the questionnaires due to altered physical or mental health were excluded from the study.
Sample size estimation
The following Taro Yaman’s formula was used to estimate the sample size, assuming that the study sites would collectively record approximately 600 follow-up visits by individuals diagnosed with HBV, based on previous hospital records:
where N is the sample population, n represents the minimum sample size to be calculated, and e is the error of tolerance (0.05). Hence,
Sampling technique/sampling
Health facilities in the northern region were stratified into two categories: regional hospitals and district hospitals. The regional hospital was included by default, as it was the only facility within that stratum. In contrast, three district hospitals were randomly selected from the pool of multiple district hospitals in the region. The estimated sample was subsequently distributed proportionally across the facilities based on their respective patient caseloads or turn out. Within each selected facility, participants were recruited from gastroenterology clinics and general outpatient departments. An extensive review of health records was conducted to identify individuals with an HBV diagnosis, from which a facility-specific sampling frame was generated. Both inpatients and outpatients were included. A simple random sampling technique, specifically the lottery method, was used to recruit participants. Clinic registers containing patients’ names and contact details were used to contact individuals prior to their scheduled hospital appointments. For individuals unwilling or unable to return to the hospital, interviews were arranged at their homes for convenience, with prior notification. This approach ensured that every eligible individual attending the selected facilities during the data collection period had an equal opportunity to participate.
Data collection instrument
The study employed a structured questionnaire to data collection. The instrument comprised three sections: (a) sociodemographic and socioenvironmental factors (age, sex, marital status, and educational level); (b) clinical (treatment type, complication status, and viral replication status); and (c) the HBV disease-specific QoL (HBQoL) instrument. The HBQoL version 1.0 is a validated disease-specific instrument developed by Spiegel et al. 25 to assess the unique impact of chronic HBV infection on patients’ daily lives. The instrument consists of 31 items organized into 5 core subscales, along with an additional 4-item a priori–defined viral response subscale that captures patients’ concerns regarding treatment effectiveness and perceived infectivity. 26 The psychological well-being subscale includes eight items and demonstrates high internal consistency, with a Cronbach’s α of 0.90. The anticipation anxiety subscale comprises six items (α = 0.88), while the vitality subscale includes five items (α = 0.90). Stigmatization is measured using six items (α = 0.89), and the vulnerability and transmission concerns subscales each contain three items, with corresponding α values of 0.82 and 0.73, respectively. The viral response subscale contains four items and demonstrates an α value of 0.75. Overall, the HBQoL scale demonstrates excellent internal consistency (Cronbach’s α = 0.96) and strong test–retest reliability. Each item is rated on a 5-point Likert scale, and scores are linearly transformed to a 0–100 scale, with higher scores indicating better HBV-related QoL. By addressing dimensions such as anxiety about viral replication, fear of infectivity, perceived stigma, and feelings of vulnerability, the HBQoL instrument provides a more detailed and meaningful understanding of the lived experience of people with chronic HBV, offering richer insights for both clinical monitoring and research compared with generic QoL instruments.
The instrument was piloted within the Ghanaian context to assess cultural appropriateness, and its reliability was also evaluated. The reliability coefficient (α) of the subscales ranged from 0.91 to 0.97, with the overall α of 0.96. There was no need to translate the instrument into English, as the original instrument, developed and validated by Speigel et al., 25 was already in English.
Data collection procedure
Data collection was conducted over a defined period at the selected health facilities in the northern region of Ghana. Eligible participants were identified on a daily basis through outpatient attendance registers at each facility. After obtaining informed consent, trained research assistants administered the structured questionnaire via face-to-face interviews in a private setting to ensure confidentiality. Interviews were conducted in English or local languages where necessary, with translations provided to ensure that participants fully understood each question. Completed questionnaires were reviewed daily by the principal investigator to ensure completeness and consistency prior to data entry.
Data analysis
Completed data were entered into a secure database and cleaned to ensure accuracy before analysis. Descriptive statistics, including frequencies, percentages, means, and SD, were used to summarize participants’ sociodemographic, clinical, and psychosocial characteristics. Although HBQoL scores are considered continuous variables, they were binarized into low and high categories using the median split rule.31,32 Bivariate analyses were conducted using logistic regression to examine the associations between independent variables and disease-specific QoL outcomes. Variable selection for the multivariable model followed a two-step strategy. First, the predictors demonstrating a univariate association with QoL at a significance level of p < 0.25 were shortlisted. Subsequently, a combination of forward and backward stepwise selection techniques was applied to derive the most parsimonious model with the best overall fit. The multivariable logistic regression model examining the predictors of disease-specific QoL was statistically significant (χ2(6) = 62.843, p < 0.001). The model explained 21.2% (Cox and Snell R2) to 28.2% (Nagelkerke R2) of the variance in disease-specific QoL and effectively distinguished between participants with poor and good disease-specific QoL. Overall, the model correctly classified 71.2% of cases, including 80.3% of those with poor QoL and 62.1% of those with good QoL.
Variables significant at p < 0.25 in the bivariate analyses were entered into a multivariable logistic regression model to identify independent predictors of disease-specific QoL. Adjusted odds ratios (AORs) with corresponding 95% confidence intervals (CIs) were reported. All statistical analyses were conducted using SPSS version 23, with statistical significance set at p < 0.05.
Ethical considerations
Ethical approval for this study was obtained from the Ghana Health Service Ethics Review Committee on 28 October 2024 (approval number: GHS-ERC:085/07/24). Permission to conduct the study was also obtained from the management of the participating health facilities. The study was conducted in accordance with the Declaration of Helsinki (1975, as revised in 2024). Written informed consent was obtained from each participant after explaining the study’s purpose, procedures, potential risks, and benefits. Participants were assured of confidentiality and anonymity; data were coded, and no identifying information was included in any reports or publications. Participation was voluntary, and respondents were informed that they could withdraw from the study at any time without any consequence for their ongoing care. All participant information was deidentified to protect the privacy of the participants.
Results
Sociodemographic characteristics
A total of 264 respondents participated in the study. This yielded a response rate of 100%. This response rate was achieved because participants who declined participation or withdrew from the study were all replaced. The mean age of participants was 38 ± 16.5 years, indicating a relatively wide age range within the sample. Sex distribution was balanced, with 48.1% of respondents identifying as female (n = 127) and 51.9% as male (n = 137). In terms of marital status, just over half of the respondents were married (51.9%, n = 135), while 35.6% were single (n = 94). Regarding educational attainment, nearly half of the respondents (48.1%, n = 127) had completed tertiary education. Additionally, 20.8% (n = 55) had attained secondary education, 14.4% (n = 38) had basic education, while 16.7% (n = 44) reported having no formal education. About one-third of respondents (32.2%, n = 85) were self-employed, 28.0% (n = 74) were employed full-time, and 10.6% (n = 28) were part-time employees. The largest proportion of respondents (33.3%, n = 88) earned more than Ghana Cedis (GHC) 2000 per month, while 28.4% (n = 75) reported earning less than GHC 350 per month. Smaller proportions fell within intermediate income brackets: 9.8% (n = 26) earned GHC 350–800, 9.1% (n = 24) earned GHC 801–1200, and 19.1% (n = 51) earned GHC 1201–2000 monthly (Table 1).
Sociodemographic characteristics of participants.

GHC: Ghana Cedis.
Clinical and treatment-related characteristics of participants
Given that health insurance coverage is high in northern Ghana, most participants (92.4%, n = 244) were insured under the National Health Insurance Scheme. In terms of their HBV infection profile, 76.5% (n = 202) were classified as having chronic nonreplicating infection (hepatitis B envelope antigen (HBeAg)-negative), whereas 23.5% (n = 62) had chronic infection with active viral replication (HBeAg-positive). Viral load data showed that nearly half of the respondents (48.1%, n = 127) either did not have viral load results available or had not been tested. Additionally, 27.3% (n = 72) had low viral loads (<2000 IU/mL), 4.9% (n = 13) had moderate levels (2000–20,000 IU/mL), 12.3% (n = 33) had high viral loads (>20,000 IU/mL), and 4.5% (n = 12) had high levels (>20,000 IU/mL) per the WHO and European Association of Study of the Liver (EASL) viral load classification index. 33
Just under one-third (31.8%, n = 84) of participants reported having experienced complications related to HBV (cirrhosis, liver failure, and hepatocellular carcinoma), while the majority (68.2%, n = 180) reported no complications. Almost all respondents (98.1%, n = 259) had received some form of treatment for HBV, with 51.1% (n = 135) indicating the use of orthodox (conventional) treatment and 47.0% (n = 124) using herbal remedies; only 1.9% (n = 5) reported not receiving any treatment (Table 2).
Clinical and treatment-related characteristics of participants.

HBV: hepatitis B virus; HBeAg: hepatitis B envelope antigen.
Perceived health, social support, and living conditions
Most participants reported adhering to their medication, with 98.1% indicating that they take their medications as prescribed. Regarding perceptions of health, the majority of participants (58.6%) described their health status as good. Nearly all respondents (93.2%) reported having family support. In terms of stigma, most participants (69.3%) stated that they did not feel stigmatized. When asked about their overall QoL, the highest proportion (62.1%) rated it as good. The majority of participants (64.0%) indicated that they were able to pay for their medications themselves, and 79.9% reported having financial support. Most participants (84.5%) had access to clean water, and 81.1% described their living environment as clean (Table 3).
Perceived health, social support, and living conditions.

Descriptive statistics of disease-specific QoL domains among participants
Table 3 summarizes the descriptive statistics and internal consistency estimates for the various psychosocial constructs assessed among participants. The psychological well-being scale, which included eight items, had a mean score of 59.8 with a SD of 26.5. The anticipation anxiety scale consisted of six items and showed a relatively high mean score of 77.6 with a SD of 24.7. The vitality scale, made up of five items, had a mean score of 57.2 (SD = 28.4). The stigma subscale, comprising six items, had a mean score of 49.6 with a SD of 28.3. The vulnerability scale, which included three items, had a mean score of 76.7 (SD = 24.3). The transmission scale, consisting of three items, had a mean score of 71.7 with a SD of 28.7. The viral response subscale, with four items, had a mean score of 77.7 (SD = 25.6). Finally, the global score, representing an overall composite measure of these domains, had a mean score of 63.6 with a SD of 20.0. Overall, there was high internal consistency across all domains, with Cronbach’s α values ranging from 0.92 to 0.98 (Table 4).
Descriptive statistics of disease-specific QoL domains among participants.

QoL: quality of life; SE: standard error.
The bold text represents overall statistics for all the parameters in the table.
Comparison of means for clinical variables
As presented in Table 5, analysis of HBV disease-specific QoL scores showed that patients with active viral replication (mean = 79.28 ± 22.06) had higher scores than those with nonreplicating infection (mean = 58.82 ± 16.59; F = 61.17, p < 0.001), and that those with complications reported higher QoL (mean = 78.34 ± 18.28) than those without complications (mean =56.76 ± 16.79; F = 89.29, p < 0.001). Being on treatment was associated with improved QoL (mean = 64.29 ± 19.45) compared to no treatment (mean = 29.36 ± 18.38; F = 15.84, p < 0.001), with orthodox therapy showing the highest scores (mean = 69.05 ±20.17; F = 17.45, p < 0.001).
Comparing mean HBQoL scores by major clinical variables.

HBQoL: hepatitis B virus quality of life instrument; HBV: hepatitis B virus; HBeAg: hepatitis B envelope antigen.
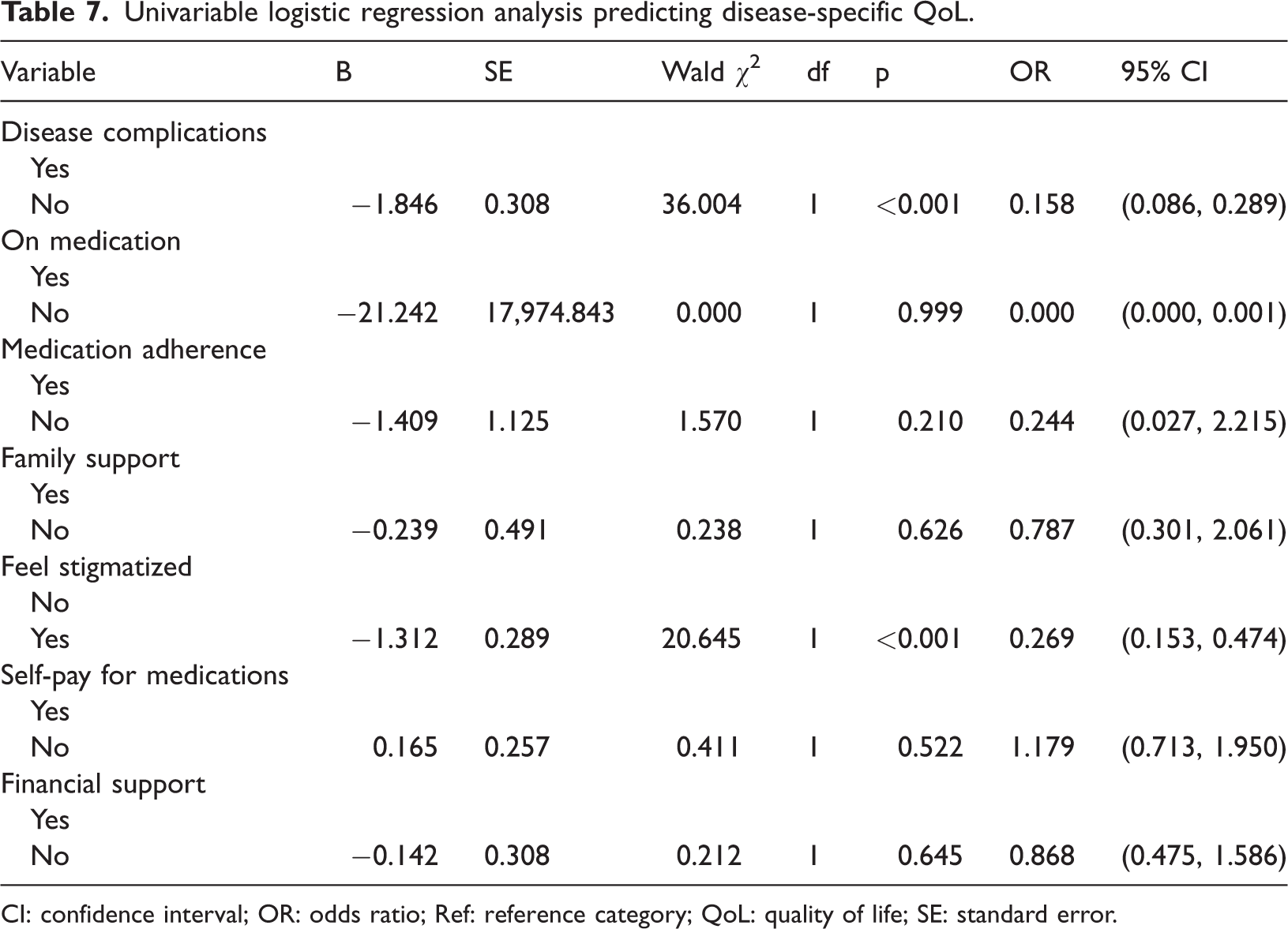
Univariable logistic regression analysis predicting disease-specific QoL
The results presented in Tables 6 and 7 showed that several factors were significantly associated with HBV disease-specific QoL. Older age was associated with increased odds of reporting a better QoL (odds ratio (OR): 1.040, 95% CI: 1.023–1.057). Participants with only basic education were less likely to report a good QoL compared to those with tertiary education (OR: 0.167, 95% CI: 0.068–0.408). Lower income was also associated with poorer QoL; participants earning less than GHC 350 (OR: 0.520, 95% CI: 0.277–0.974) or GHC 350–800 (OR: 0.321, 95% CI: 0.123–0.841) had reduced odds compared to those earning more than GHC 2000, while earning GHC 1201–2000 was associated with higher odds (OR: 2.305, 95% CI: 1.096–4.852). Participants with chronic nonreplicating infection had higher odds of reporting better QoL (OR: 5.307, 95% CI: 2.755–10.222). However, when these variables were controlled for in the multivariable model, the direction of association reversed, demonstrating that nonreplicating infection (HBeAg-negative) independently predicted lower QoL (AOR = 0.344)
Univariable logistic regression analysis predicting disease-specific QoL.

CI: confidence interval; HBV: hepatitis B virus; OR: odds ratio; Ref: reference category; QoL: quality of life; HBeAg: hepatitis B envelope antigen; GHC: Ghana Cedis.
Post Single individuals who are single following a separation or divorce.
Univariable logistic regression analysis predicting disease-specific QoL.
CI: confidence interval; OR: odds ratio; Ref: reference category; QoL: quality of life; SE: standard error.
Additionally, the absence of HBV-related complications (OR: 0.158, 95% CI: 0.086–0.289) and not experiencing stigma (OR: 0.269, 95% CI: 0.153–0.474) were associated with significantly better QoL.
Multivariable logistic regression analysis predicting disease-specific QoL
The logistic regression analysis showed that age, HBV profile, and the presence of disease complications were significant predictors of HBV disease-specific QoL among the study participants. After adjusting for other variables, age remained significantly associated with QoL, with each additional year increasing the odds of reporting better disease-specific QoL by approximately 2.8% (Wald χ2 = 9.49, p = 0.002; OR: 1.028, 95% CI: 1.010–1.047). Participants with a HBeAg-negative profile had significantly lower odds of reporting good QoL compared to those with a replicating virus (HBsAg-positive) (Wald χ2 = 6.15, p = .013; OR: 0.344, 95% CI: 0.148–0.800), indicating that nonreplicating infection was associated with lower disease-specific QoL.
The absence of disease complications was also significantly associated with poorer QoL (Wald χ2 = 11.69, p = 0.001; OR: 0.300, 95% CI: 0.150–0.598), suggesting that participants without complications were substantially more likely to report lower HBV-related QoL than those with complications (Table 8).
Multivariable logistic regression analysis predicting disease-specific QoL.

AOR: adjusted odds ratio; CI: confidence interval; HBV: hepatitis B virus; Ref: reference category; QoL: quality of life; SE: standard error; HBeAg: hepatitis B envelope antigen.
Discussion
This study was conducted to assess HBV disease-specific QoL and its predictors among people living with chronic HBV infection in the northern region of Ghana using a validated HBV-specific QoL instrument.
The global HBQoL mean score of 63.6 ± 20.0 provides an overall indication of how participants in the present study perceived their well-being while living with HBV. This finding is similar to the mean score of 62.8 ± 19.5 reported in a study conducted in the United States of America, 25 but slightly lower than 66.1 ± 20.9 reported among people living with HBV in Iran. 26 The few Ghanaian studies that assessed HRQoL among individuals living with HBV relied on generic and qualitative procedures, making direct comparisons difficult, despite reporting low QoL scores.28,34
Unlike generic measures, the disease-specific QoL score obtained in this study captures key aspects such as anxiety about viral replication, fear of infectivity, stigma, and emotional challenges. This mid-range score suggests that although some areas of life remain stable, important psychosocial concerns persist. This highlights the need to integrate counseling, stigma reduction, and patient-centered education into HBV care to address both clinical and psychosocial needs and to guide targeted improvements in QoL in this high-burden context.
Age and HBV disease-specific QoL
The present analysis identified age as a significant predictor of HBV disease-specific QoL. The finding that HBQoL increased with advancing age aligns with previous studies, suggesting that older adults with chronic diseases may adapt more effectively to their health condition over time. 35 A study conducted among Ghanians also reported higher mean HRQoL scores in psychological, environmental, and social domains among older adults compared to their younger counterparts. 36 Older individuals often develop coping strategies that enable them to manage the daily realities of living with a chronic infection such as HBV. 37 They may also have more stable social support networks, better health literacy, and a stronger sense of acceptance and satisfaction with their health status compared to younger individuals, 38 who may experience greater disruption in their work, family roles, or social relationships due to HBV infection. 37
In Ghana and other African settings, health-related QoL among elderly individuals with chronic diseases such as HBV is closely tied to cultural values that emphasize care, respect, and belonging. Older adults often receive support from children and extended family members, which eases the financial and emotional burden of managing a chronic illness. 39 Their respected status within the community allows them to remain socially engaged, thereby reducing stigma and strengthening their sense of dignity. Spiritual and religious practices provide comfort and resilience, while traditional diets and active daily routines help maintain physical health. Together, these cultural practices create a supportive environment that enhances the well-being of elderly people with HBV. 40
Beyond social, family, and spiritual support, the positive association between age and HBQoL may indicate that older adults are more likely to engage with healthcare services, adhere to treatment, and maintain supportive relationships, all of which can mitigate the negative impacts of HBV infection on QoL. It is also possible that older adults have adjusted their expectations regarding health and well-being, leading to higher self-reported QoL despite the presence of a chronic condition. This underscores the importance of designing age-sensitive interventions that build on the strengths of older adults while ensuring that younger adults receive adequate psychosocial and clinical support to cope with the challenges of HBV infection.
Contrary to the findings reported in this study, older age has been associated with greater disease burden and complications in some settings, which may instead lower QoL. 41 In the context of HBV, older age may compound challenges to health-related QoL as the natural accumulation of molecular and cellular damage leads to declining immunity, reduced liver function, and increased vulnerability to disease progression. Beyond these biological changes, older adults with HBV may also experience psychological strain related to retirement, loss of social roles, or bereavement, which can intensify feelings of isolation and diminish resilience in coping with chronic illness. Stigma associated with HBV can further limit social interactions, adding to the restrictions that already accompany aging. Together, the combined effects of biological decline, psychological distress, and social constraints place older adults living with HBV at heightened risk of reduced QoL.
Effect of HBV profile
The study also found an inverse relationship between good HBQoL and HBeAg-negative profile; this observation is biologically unexpected. 8 Patients with nonreplicating infection often require less intensive medical monitoring and may not need antiviral therapy, 42 which can reduce the psychological and economic burdens associated with treatment. This finding may reflect psychosocial factors, such as anxiety, stigma, 11 or reduced medical attention, which could lead patients to feel uncertain or neglected. This highlights that in HBV, QoL is not only influenced by viral activity but also by psychological, social, and healthcare factors.
Impact of disease complications
Another significant finding was the strong association between the absence of disease complications and lower odds of favorable outcomes. This result is unexpected and counterintuitive, as disease complications are generally thought to worsen health outcomes and reduce well-being, particularly among individuals living with HBV. For example, Zhang et al. and other researchers have reported that HBV-related complications are associated with lower QoL scores.43–45 One possible explanation for this finding is that patients without complications may receive less medical attention, monitoring, or counseling compared to those with advanced disease, leaving them feeling uncertain about their health or unsupported. Additionally, the perception of being “stable” or asymptomatic may lead to reduced engagement with care, health-seeking, and preventive behaviors, 46 which could negatively influence their perceived QoL. Psychosocial factors, such as anxiety about potential future complications, 47 fear of disease progression, and concerns of premature mortality, can also contribute to anxiety and depression, further diminishing QoL.48,49
In summary, when individuals such as the participants in this study who have no complications feel stable or asymptomatic, they may engage less with care, reduce preventive behaviors, and underestimate future health risks, which can lower their HRQoL. Reduced vigilance and underlying anxiety about potential complications may further compromise their sense of well-being.
These findings suggest that in HBV disease management, QoL is shaped not only by the presence of clinical complications but also by the patient’s engagement with care, social support, and psychological well-being.
Strengths and limitations
A key strength of this study lies in its use of a validated disease-specific QoL instrument, which provides deeper insights into domains uniquely relevant to individuals living with HBV. The study also employed rigorous sampling procedures and robust analytical methods to identify predictors of QoL in an under-researched endemic region. Nonetheless, several limitations should be acknowledged. As a cross-sectional study, causal inferences cannot be established. The reliance on self-reported data introduces the potential for recall and social desirability bias. Restricting inclusion to patients who had contact with selected health facilities may have introduced selection bias, and the findings may not be generalizable beyond similar rural or semiurban endemic communities. Finally, the study was unable to account for the duration of infection or the level of treatment duration and adherence, both of which could have influenced the QoL scores.
Conclusion
This study demonstrates that QoL among people with HBV in northern Ghana is shaped by both clinical and psychosocial factors. Older age was associated with better outcomes, likely due to adaptation and cultural support, while paradoxically, nonreplicating infection and absence of complications were associated with poorer QoL, reflecting the role of healthcare engagement and psychosocial concerns. Treatment, particularly orthodox medical care, was strongly associated with improved well-being. These findings highlight the need for patient-centered, age-sensitive interventions that integrate effective clinical care with counseling, stigma reduction, and social support to improve the lives of people living with HBV.
Footnotes
Acknowledgment
We acknowledge the staff of the four selected hospitals for their support, and our participants who voluntarily participated in this study.
Author contributions
F.N.O.O: Conceptualization, Methodology, Data collection, Data Analysis, Writing, and Original draft preparation. V.E.S.-D.: Methodology, Supervision, Writing, and Original draft preparation, Supervision, editing, reviewing. L.L. and A.A: Supervision, writing original draft, editing, and reviewing. A.D.W.: Supervision, Writing original draft, and reviewing. M.C.A.: Writing original draft and reviewing. A.M.D.: Data Curation & Formal Analysis.
Availability of data and material
The data are available from the corresponding author upon reasonable request.
Declaration of competing interest
The authors have no financial or nonfinancial interests to declare.
Ethical considerations
The study received ethical approval from the Ethics Review Committee of the Ghana Health Service (GHS-ERC:085/07/24). Permission was obtained from the Directors of the selected health facilities in the northern region before conducting the study. All participants provided written informed consent before participation. Interviews were conducted in a private setting, and participants’ identities were kept anonymous by not disclosing their real names.
Funding
This research received no specific grant from funding agencies in the public, commercial, or nonprofit sectors.