
Abstract
Objective
This study aimed to evaluate the clinical outcomes of a new implant restoration approach for patients with limited interocclusal space in the posterior region.
Materials and methods
A total of 37 patients (19 females and 18 males) were enrolled in this study, receiving 62 implants. A locking taper implant (Bicon) was placed during the first-stage procedure, positioned >2 mm under the bone. An extraoral cementation technique was used to cement the crown and abutment. The survival and success rates of the implant restorations were evaluated based on plaque index, modified bleeding index, probing depth, marginal bone loss, and the patient’s subjective satisfaction.
Results
The success rate of the new implant restorations was 96.7% at the 1-year follow-up, with patients reporting satisfactory outcomes. Marginal bone loss and soft tissue changes were not significantly different at different depths of placement (p > 0.05).
Conclusions
The use of a locking taper implant along with appropriate prosthetic strategies may be an effective approach for the prosthetic rehabilitation of patients with limited interocclusal space and reduced occlusal vertical dimensions.
Introduction
Decreased occlusal vertical space and insufficient interocclusal space for a dental implant prosthesis are common clinical problems. According to Misch, 1 the interocclusal space should be ≥8 mm in vertical height. However, in the posterior region, the interocclusal space may be reduced due to factors, such as overeruption of opposing teeth in the edentulous 2 and wear of the occlusal surface of the natural dentition. 3 To restore the interocclusal space, several approaches have been used, including grinding or orthodontic intrusion of the opposing extruded teeth, alveolar ridge osteotomy, extraction for occlusal reconstruction, personalized abutment, and integrated abutment crown. However, each method has certain limitations. For instance, grinding of overerupted vital teeth is efficient and can create 1–2 mm of space; however, it may be associated with symptoms, such as dentine hypersensitivity or pulpitis.
Removal of the alveolar ridge should be considered only when sufficient bone height is present at the implant site. Posterior maxillary segmental osteotomy (PMSO) 4 may restore the occlusal curve of the missing teeth by moving the opposing tooth segment. However, the major disadvantages of osteotomy include technical difficulty, surgical trauma, and postoperative complications. Orthodontic intrusion of teeth is widely used in combination with the mini-implant nail anchor method, which creates a 2–4 mm restoration space by anchoring the posterior teeth, 5 thereby restoring the original restoration space and occlusal curve. However, this approach is technically challenging, requires a longer treatment duration, and is associated with risks such as root resorption and tooth torsion. 6 Personalized abutment may be considered for patients with limited interocclusal space. Bittner et al. 7 used wide-necked implants and personalized larger mesiodistal diameter abutments to reinforce anchorage. However, the fabrication of personalized abutment is more expensive, and occlusal forces act on the implant restoration. The University of California, Los Angeles (UCLA) abutment offers a straightforward and efficient solution for managing insufficient interarch space in implant prosthodontics. However, it is associated with a higher incidence of prosthetic complications, particularly abutment screw loosening and ceramic fracture. Additionally, it demands high precision in the fabrication of the implant–abutment connection interface and entails higher costs.8,9 Integrated abutment crowns can be used in scenarios where the abutment and crown are directly fabricated in the laboratory or bonded chemically. Occlusal surface screw holes have been used for screw retention or self-locking taper retention (i.e. Bicon implants). Although integrated abutment crowns have certain advantages, such as restoration of space and absence of residual adhesive, there are limitations associated with the use of a screw-retained implant–abutment interface. First, the screw hole destroys the integrity of the crown structure, which may lead to porcelain collapse. 10 Second, achieving passive emplacement is difficult, and there is an increased incidence of mechanical complications. Finally, due to microleakage and micromovement of the implant–abutment interface, 9 the interface may not be located deep under the bone.
Wang et al. 11 proposed an unconventional protocol for the prosthetic management of patients with limited interocclusal space. The basic steps of the proposed method are as follows: (a) primary surgery to place implants deeply; (b) second-stage surgery and removal of the bone tissues that affect the crown emplacement using a sulcus reamer; (c) designing the crown with a subgingival edge, resulting in an abutment body height ≥5 mm; and (d) use of extraoral cementation technique to fit the abutment and crown. The researchers reported that this proposed strategy was simple, minimally invasive, convenient, and required no additional equipment or tools. Furthermore, the soft and hard tissue contours were preserved, and good sealing was achieved using the locking taper design, which could effectively reduce the probability of biological complications. However, these findings are based on one case report and require validation in further clinical cohort studies. Therefore, the present study aimed to evaluate the 1-year clinical outcomes of this new implant restoration strategy in patients with limited interocclusal space in the posterior region. To accelerate knowledge dissemination, this study was initially posted as a preprint on Research Square (DOI: 10.21203/rs.3.rs-225700/v1) prior to peer review. The current manuscript incorporated revisions based on expert feedback, particularly in the restoration protocol section. All data and conclusions remain consistent with the original preprint. 12
Methods
Study design and patient selection
This study was conducted in the Department of Implantology, Fourth Affiliated Hospital of Nanchang University, China, in accordance with the Declaration of Helsinki 1975, as revised in 2024 and was approved by the hospital’s ethics committee. All patients provided written informed consent prior to study enrolment. Patient data were deidentified to ensure anonymity. The reporting of the study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
13
A total of 37 patients were included, comprising 18 males and 19 females. The following inclusion criteria were applied to recruit patients for this study.
Patients were required to be in good general health with no chronic systemic diseases. Patients required dental implant treatment in the posterior maxilla. A cone beam computed tomography (CBCT) was performed with patient’s jaws in maximum intercuspation. Radiographic analysis revealed that the distance from the prospective occlusal plane to the alveolar bone crest was <7 mm. In the mandible, a minimum distance of ≥13 mm from the planned occlusal surface to the mandibular canal is required. In the maxilla, although the requirement is less stringent, the surgical site must be suitable to a maxillary sinus floor augmentation procedure, followed by implant placement either simultaneously or in a staged protocol.
Patients with a history of temporomandibular joint (TMJ) disorder, severe bruxism, oral ulcers, or precancerous lesions were excluded from the study.
In addition, intraoral examination and nonsurgical periodontal treatment were performed to ensure oral health. The aim of the study was explained to all patients and written informed consent was obtained from every patient.
Implant placement
For each patient, preoperative CBCT was performed to ensure that the implant placement space was ≥6 mm and the distance from the implant neck to the antagonist teeth was >7 mm. The depth of implant placement was recorded. Thirty minutes prior to the surgical procedure, each patient was premedicated orally with a sustained-release ibuprofen capsule (100 mg) and dexamethasone acetate tablet (2 mg). Chlorhexidine (0.12%) and iodophor were used for oral and skin disinfection, respectively.
All surgical procedures were performed under the supervision of an experienced oral surgeon using local anesthesia (4% articaine hydrochloride and 1:100,000 epinephrine; Pierrel; Milan, Italy). The implants were placed using the immediate or delayed placement techniques.
In the delayed implant placement approach, a full-thickness mucoperiosteal flap was raised at the alveolar ridge crest. The implant depth was determined using preoperative CBCT, and a cavity was drilled following the drilling sequence recommended by the manufacturer. The locking taper implants (Bicon LLC; Boston, MA, USA) were placed. The polyethylene healing plug was trimmed to the level of the ridge top, the harvested bone was placed, and the surgical site was sutured.
In the immediate implant placement approach, following minimally invasive tooth extraction as per the preoperative design, the implant hole was prepared. The locking tapered implants were placed, and the healing plug was trimmed to the level of the alveolar ridge on the buccal side.
In particular, the depth of the implant should be equal to or greater than the planned depth. Patients were prescribed amoxicillin (1500 mg three times a day for 5 days) and instructed to rinse mouth with 0.12% chlorhexidine three times a day for 7 days. Patients were called after 3 days to evaluate wound healing. The second-stage surgery was performed after 3 months in the delayed implant placement group and after 4 months in the immediate implant placement group. Following local infiltration, a crestal incision was made to remove the healing plug. The sulcus former was rotated on the guide pin to remove bone tissue that could affect the prosthesis. A temporary titanium abutment was installed to form the cuff.
Prosthodontic treatment
The implant-level transfer impression was made 2–4 weeks following abutment installation. An implant-level impression was made using the closed-tray double-mix technique. The healing abutment was removed, and a transfer coping (Bicon LLC; Boston, MA, USA) was seated. A suitable stainless-steel tray was selected, and the impression was taken using an addition-type silicone impression material (Huge; Shandong, China). A shoulderless abutment (Bicon LLC; Boston, MA, USA) was then milled. The cemented portion of the milled abutment featured guiding planes and an antirotation design. A zirconia-based all-ceramic crown or a cobalt–chromium porcelain-fused-to-metal crown was fabricated. The separated single crown and abutment prosthesis was designed as a subgingival, semianatomical/nonanatomical cusp, where the height of the abutment body was ≥5 mm. The fabricated prosthesis was tested in the mouth to ensure good positioning of the abutment–implant and crown–abutment. The crown was cemented to the abutment using a glass ionomer cement (Fuji I, GC, Inc.; Japan) in vitro. Excess cement was then carefully removed, and the cement interface was polished well. The patients were called biannually for a follow-up examination and nonsurgical periodontal treatment. Clinical and imaging evaluations were performed 1 year postoperatively. Representative images of various clinical procedures are shown in Figure 1.

Representative images of various clinical procedures. (a) Preoperative CBCT analysis of the patient’s edentulous showing insufficient interocclusal space; (b) implant placement simulation; (c) deep implant placement (4 mm under the bone); and (d) postoperative CBCT showing a distance of >7 mm between the implant neck and opposite tooth. (e) In the second-stage surgery, sulcus former was rotated on the guide pin to remove bone tissues that affected restoration. (f–g) The margin of the restoration abutment was prepared to extend 4–5 mm subgingivally. (h) The crown and abutment were combined using the extraoral cementation technique, and the excess adhesive was removed. (i) All-ceramic crowns were used for implant restoration. (j) Image after 1 year. (k) Intraoral photo after 1 year and (l) Intraoral photo after 1 year. CBCT: cone beam computed tomography.
All CBCT images were taken in the intercuspal position using Carestream CS 9300 Select (Carestream Health, Inc.; France).
Follow-up and evaluation
Following 1 year of functional loading, the prostheses were evaluated according to the definitions of implant success, survival, and failure published by Misch. 14 Clinical indicators, including the modified plaque index (mPI), modified sulcus bleeding index (mSBI), and probing depth (PD) were reviewed and evaluated. All data were measured by the same dentist using a periodontal probe (15 UNC/CP-11.5B Screening Color-Coded Probe, Hu-Friedy; Chicago, IL, USA). In addition, mechanical complications, such as fracture or cracking of the implant or abutment, loosening of the abutment, and cracking of the crown, were recorded.
Radiographic evaluation was performed using Digimizer Image Analysis Software (V 4.5.1, MedCalc Software bvba; Ostend, Belgium). Images were calibrated according to the image length and true length of the implant. The distance from the first thread of the implant to the crest of the alveolar ridge was measured to determine the marginal bone level. Mesial and distal bone heights at the prosthetic insertion were recorded at the time of functional loading as ML(0) and DL(0), respectively, and the 1-year follow-up as ML(T) and DL(T), respectively. Average bone resorption was calculated as mesial marginal bone loss (MBL).



The imaging measurement was performed by an assistant blinded to the study design. All images were measured once every 2 days; each measurement was taken thrice, and the average value was recorded. The satisfaction survey was conducted according to the evaluation method of Pjetursson et al. 15 The visual analog scale, with scores ranging from 0 (very dissatisfied) to 100 (very satisfied) was used for statistical analysis.
Data analysis
The Statistical Package for Social Sciences SPSS v 24 software (IBM Corp., Armonk, NY, USA) was used to analyze the data. The Kolmogorov–Smirnov test was applied to assess the normality of the data. Descriptive statistics, including mean value, SD, and range, were presented. The predictive variables included patient age, sex, implantation site, bone type, restoration type, smoking status, timing of implant placement (immediate vs. delayed), implant depth, implant diameter, and implant length. Outcome variables included implant failure and marginal bone resorption. Chi-square test was used to analyze the relationship between independent variables and implant failure. Kruskal–Wallis test was used to determine the relationship between implant depth and mPI, mSBI, and PD. A generalized estimation equation was used to analyze the relationship between predictive variables and marginal bone resorption. A significance level of 0.05 was used for all statistical analyses.
Results
The demographic information of the study participants and characteristics of implants and prosthesis are presented in Table 1.
Summary of basic information.
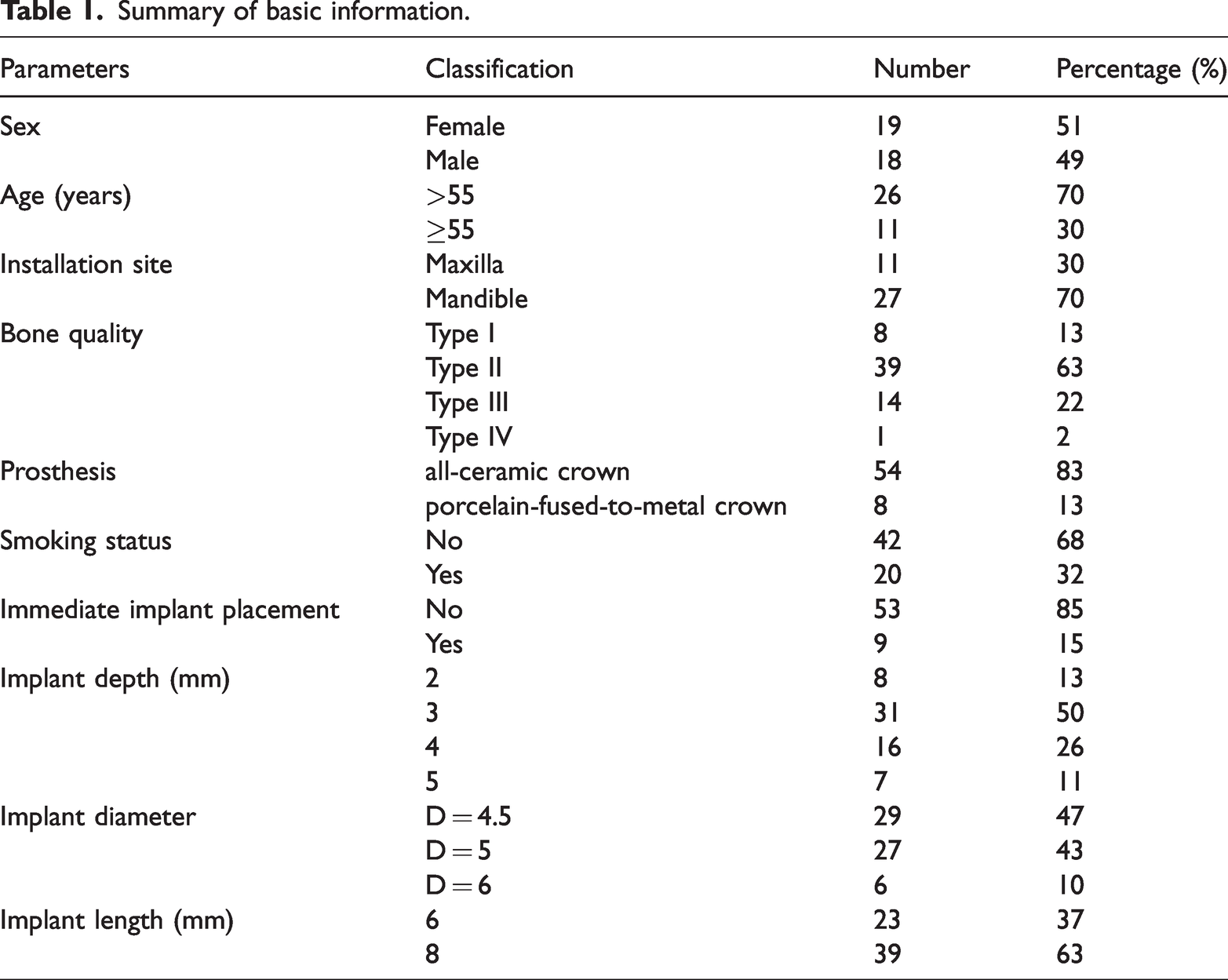
This study included a total of 37 patients (19 female and 18 male) who received 62 implants (Table 1). Overall, 35 patients (60 implants) met the success criteria, resulting in a success rate of 96.7%. One implant in one patient (male, 47 years old, tooth #36) failed following 1 month of loading, and another patient exhibited bone resorption around the implant (≤3 threads) at the 1-year follow-up. There were no mechanical complications during the follow-up period. All patients maintained good oral hygiene and periodontal health throughout the follow-up period. Only one patient reported signs of peri-implantitis. The clinical evaluation parameters of the 62 implants at the 1-year follow-up are presented in Table 2.
Summary of clinical parameters.
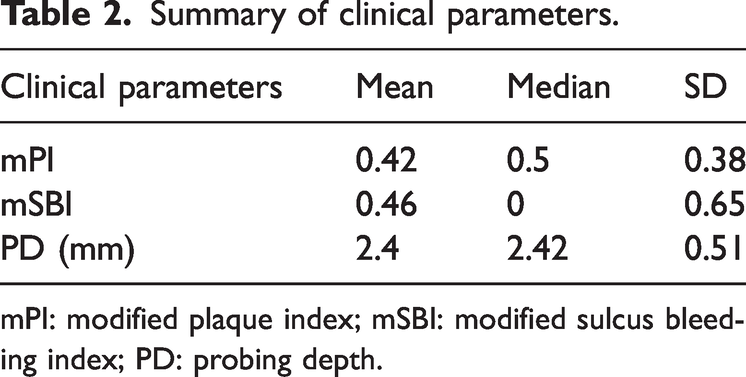
mPI: modified plaque index; mSBI: modified sulcus bleeding index; PD: probing depth.
Periodontal conditions did not show any statistically significant difference based on the placement depths under the bone (p > 0.05) (Table 3).
Relationship between different implantation depths and mPI, mSBI, and PD (mean ± SD).

mPI: modified plaque index; mSBI: modified sulcus bleeding index; PD: probing depth.
At the 1-year follow-up, the mean MBL was 0.14 ± 0.42 mm, and the mesial and distal MBL values were 0.18 ± 0.52 mm and 0.10 ± 0.42 mm, respectively. There was no statistically significant difference in bone resorption at the mesial and distal edges (T = −1.319, p = 0.192).
The generalized estimation equation was used to evaluate the potential risk factors affecting MBL of the implants (Figure 2). Among the various indicators analyzed, sex (p = 0.03), age (p = 0.04), bone quality (p = 0.01), and implant diameter (p < 0.01) demonstrated significant association with MBL.

Risk factor analysis for MBL using a generalized estimating equations model. MBL: marginal bone loss
At the 1-year follow-up, the satisfaction survey showed very high patient satisfaction rates for function and aesthetics (overall satisfaction, 96.86 ± 3.44) outcomes. For 95% of the implant sites, patients reported that the therapeutic effect of implant restoration met or exceeded their expectations. No patient complained of TMJ discomfort.
Discussion
The study investigated the clinical outcomes of an unconventional implant strategy for patients with limited interocclusal space in the posterior region. A total of 62 locking taper implants were placed deep under the bone, restored using an abutment crowns prosthesis, and followed-up for 1 year. The success rate of the implants was evaluated using various indices, including the mPI, mSBI, PD, and patient’s subjective satisfaction. At the 1-year follow-up, the implants demonstrated a high success rate (>96%), with an MBL of 0.14 ± 0.42 mm. No biological or mechanical complications were observed despite the increased placement depth.
Among the various indicators, MBL was significantly affected by sex (p = 0.03), age (p = 0.04), bone quality (p = 0.01), and implant diameter (p < 0.01). The differences in MBL related to sex, age, and bone quality may be associated with osteoporosis and decreased hormone levels in older female patients. 16 Nonetheless, MBL remained within an ideal range (according to the classical theory, MBL should be between 1.0 and 1.5 mm after the first year of functional load and <0.2 mm every year after that). 17 In this study, an increase in the implant diameter was associated with reduced MBL, highlighting the role of the implant diameter in stress dispersion, consistent with findings reported by Baldassarri et al. 18
Reduction of the interocclusal space or occlusal vertical dimension has been observed in dental patients who have lost their teeth periodically and did not undergo any oral rehabilitation. A common method to restore the interocclusal space is the simultaneous removal of the alveolar crest at the implant site. Although this approach is convenient and does not increase the number of procedures, it is associated with loss of bone and soft tissues in the vertical direction and unsatisfactory aesthetic outcomes. In addition, inconsistency of the soft tissues with the neighboring teeth may encourage food impaction and lead to peri-implantitis. 19
The implant restoration strategy used in this study has advantages at each stage. The surgical procedure is consistent with traditional procedures and techniques. The restoration of bone tissue was maximized by locking taper implants. There is evidence in favor of single-tooth restoration with 6-mm implants in the posterior region. 20 Therefore, this strategy is convenient and may be considered in cases where the distance between the jaw and the important anatomical structure is >13 mm.
In this study, bone tissue was accurately removed in the second-stage operation, in contrast to the simultaneous bone removal during primary surgery. The authors believe that no healthy tissue should be removed, and the principles of prosthetic-driven deorganization should be followed to avail its advantages, such as minimal invasiveness when creating the restoration space and restoration of the bone tissues to support the soft tissues around the implant, including the mesial and distal, buccal, and lingual soft tissues. Therefore, there was no significant change in the vertical height of the soft tissues, and the amount of attached gingiva was maintained. The width of the attached gingiva can be further increased following the placement of the temporary abutment. The restoration of the soft tissue contour along with that of the adjacent teeth avoids problems such as food impaction.
In this study, the periodontal state around the implant restoration remained healthy and stable. Approximately 7% of the patients reported occasional food impaction, and the remaining patients found the prosthesis easy to clean, with no inflammation observed in the hard or soft tissues around the implant neck. External stimulation and bacterial invasion were minimized during primary healing and following crown repair. These prosthetic strategies provided better aesthetic outcomes, long-term stability, and results consistent with previous studies. 20
A simple and comfortable extraoral cementation technique was used for cemented retention in this study. The integrity of the occlusal surface was maintained, and the chances of mechanical failure were reduced. A major concern with cemented retention is the presence of residual adhesive, which can contribute to the development of peri-implantitis. 21 Various approaches, such as the rubber dam method 22 and copy abutment method 23 have been proposed to reduce the residual adhesive. However, these techniques are not suitable for subgingival prosthesis edge, and the adhesive may not be removed. In contrast, the extraoral cementation technique facilitated complete removal of the residual adhesive, thereby preventing any irritation to the soft tissues. In addition, the crown contact relationship was assessed during the crown trial process after the implant–abutment was fully seated, ensuring a complete bacterial seal at the implant–abutment interface. A locking taper implant was selected because it allows minimally invasive repair and provides a bacterial seal at the implant–abutment interface located deep under the bone. 24 Its unique plateau design allowed restoration of single-tooth spaces of 5 or 6 mm using a solid abutment, thereby minimizing the incidence of mechanical complications. 20 Other implant systems may also achieve a complete bacterial seal if restoration space is insufficient, as in the method proposed in this study. When placing the implant deep under the bone, it is important to note that the implant–abutment connection in screw retention can easily be obstructed by the bone tissues, making it difficult to achieve complete passive placement. In contrast, the abutment of a locking taper implant can be separated to facilitate clinical examination. In cases of crown fracture, screw-retained implant restorations offer the advantage of predictable retention and retrievability compared with cement-retained restorations. Moreover, the locking taper design of the implant–abutment interface allows us to knock in the reverse direction to dislocate the abutment from the implant, making prosthesis repair very convenient.
For soft tissue, this study achieved favorable outcomes in the removal of residual adhesive and complete bacterial closure at the implant–abutment interface. Some studies have suggested that alterations in the occlusal curve synergistically contribute to TMJ dysfunction when combined with other etiological factors.25,26 Notably, in the present study, patients (including those with suboptimal occlusal curves) reported no TMJ-related complaints during follow-up. This observation aligns with clinical findings indicating that restoration of the occlusal curve to ideal parameters does not necessarily translate into satisfactory masticatory function. 27 Particularly, in cases of partial edentulism, the TMJ system demonstrates remarkable resilience, remaining unaffected even when occlusal curve reconstruction is incomplete. However, the therapeutic viability of this approach in patients with severe occlusal curve disturbances remains unclear in the context of implant rehabilitation. To conclusively evaluate the proposed treatment strategy, further investigations with larger cohorts and extended follow-up periods are warranted.
In summary, the advantages of this strategy include minimal invasiveness, time effectiveness, low technical sensitivity, and no requirement of additional tools. In addition, this study reported high patient satisfaction, a wide range of indications, maximal tissue preservation, and stability of the soft and hard tissues around the implant.
Conclusions
The use of locking taper implants and adoption of appropriate prosthetic strategies may provide an effective treatment approach for the prosthetic rehabilitation of patients with limited interocclusal space and reduced occlusal vertical dimension.
Footnotes
Acknowledgment
We express our sincere gratitude to all patients for their trust and cooperation.
Authors’ contributions
HW-W designed the research. JQ-H, CQ-H, JM-G, and SG-G recruited the study participants as well as collected and managed the data. LC-Y analyzed the data. The article was written by XX and revised by WH-X.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest relating to this study.
Funding
This work was supported by the Pingshan District People’s Hospital Dean Fund Project (202220).