
Abstract
Objective
This study aimed to compare the clinical and angiographic outcomes of aneurysms with an incorporated branch treated using traditional endovascular coiling or a flow diverter device.
Methods
This single-center retrospective cohort study was conducted at Yixing People’s Hospital from January 2015 to December 2023. The final analysis included 63 aneurysms treated with a pipeline embolization device (with or without coils) and 69 treated with endovascular coiling (with or without traditional stents).
Results
Overall, 26 aneurysms (41.3%) in the pipeline embolization device group and 44 (63.8%) in the coiling group achieved complete or near complete occlusion (p = 0.009). At follow-up, 16 branches (25.4%) in the pipeline embolization device group and 12 (17.4%) in the coiling group were occluded (p = 0.523). The stent-assisted coiling subgroup showed a significantly higher aneurysm occlusion rate than the pipeline embolization device group (p = 0.004), whereas no significant difference in branch occlusion rate was observed between the two groups (p = 0.285).
Conclusions
For aneurysms with incorporated branches, stent-assisted coil embolization achieves a higher aneurysm occlusion rate than with pipeline embolization device treatment, without a corresponding increase in branch artery occlusion. If the incorporated branch is considered sacrifiable (its loss would not result in significant neurological deficits), stent-assisted coiling should be regarded as the preferred treatment option.
Introduction
Endovascular treatment of intracranial aneurysms quickly became widespread following the International Subarachnoid Aneurysm Trial, 1 and several related studies2–5 have demonstrated its better outcome in terms of survival free of disability compared with that observed in neurosurgical clipping. As endovascular coiling proved to be less effective for treating large or giant aneurysms, the pipeline embolization device (PED) emerged as an alternative endovascular treatment strategy for large or giant, wide-necked intracranial aneurysms. It was approved by the U.S. Food and Drug Administration in 2011. The PED exerts a flow-diverting effect that can reduce or slow aneurysmal flow, promote thrombosis, and provide support for the neointima. It has been shown to be efficient and safe in numerous studies.6–9
For aneurysms with an incorporated branch, which may alter the hemodynamics within the aneurysm, the effectiveness of endovascular coiling and pipeline embolization remains uncertain. Previous studies have reported that coiling 10 and pipeline embolization11–13 for treating such aneurysms were unsatisfactory. Although these studies reported inefficiencies for both strategies, most did not compare them. Moreover, no study has examined the fate of the incorporated branches.
In this study, we retrospectively reviewed aneurysms with an incorporated branch that were treated with endovascular coiling or PED and compared the two procedures to assess differences in safety, complications, clinical and angiographic outcomes, and the preservation of incorporated branches.
Materials and methods
This retrospective cohort study was designed to compare the clinical and angiographic outcomes of two endovascular treatment strategies (PED vs. endovascular coiling) for intracranial aneurysms with an incorporated branch. This study was granted exemption from ethical review by the Institutional Review Board (IRB) of Yixing People’s Hospital. Written informed consent was obtained from all patients. Our study was conducted in accordance with the Declaration of Helsinki 1975, as revised in 2024. Reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14 The treatment strategy was determined based on aneurysm size and complexity. PED is preferred in treating large, giant, and complex aneurysms. As PED requires dual antiplatelet therapy, it was not used in ruptured aneurysms.
Study population
Aneurysms with an incorporated branch treated with endovascular coiling or PED at our institution were retrospectively and consecutively reviewed between 2015 and 2023. Aneurysms with an incorporated branch were defined as those having one or more branches arising from the aneurysm neck or sac. Using our prospectively established database, we collected demographic data, clinical characteristics, procedural details, and angiographic outcomes to assess the therapeutic effects of the two treatment strategies. Patients without follow-up angiography were excluded. Ultimately, 63 aneurysms treated with PED (with or without coils) and 69 aneurysms treated with endovascular coiling (with or without traditional stents) were included in this study. All included aneurysms had a single incorporated branch.
The sample size was calculated based on a preliminary pilot study (n = 20), which demonstrated a 25% absolute difference in the primary outcome (aneurysm occlusion rate) between the PED and coiling groups. For a two-independent-sample comparison of proportions (aneurysm occlusion rate as the primary outcome), G*Power 3.1 software (version 3.1.9.7) was used to estimate the required sample size. With a type I error rate (α) of 0.05 and a statistical power (1–β) of 0.80, the minimum sample size required for each group was calculated to be 58. Accounting for potential loss to follow-up (e.g. 5%–10% attrition in clinical practice), the final enrolled sample size (63 in the PED group and 69 in the coiling group) exceeded the calculated minimum, ensuring adequate statistical power to detect the prespecified effect size.
Endovascular procedure
Patients treated with PED received dual antiplatelet therapy (100 mg/day acetylsalicylic acid and 75 mg/day clopidogrel) for 5 days prior to the endovascular procedure. Platelet function was assessed using thromboelastography, with a target platelet inhibition of 30%–90%. If the inhibition rate was >90%, treatment was suspended, and clopidogrel was withheld until the inhibition rate decreased to <90%. If the inhibition rate was <30%, clopidogrel was replaced with prasugrel. The procedure was performed under general anesthesia. Heparin (70 U/kg) was administered intravenously throughout the procedure. The size of the PED was determined based on the size of the parent artery and aneurysm neck, with the diameter slightly larger than that of the parent artery and the length sufficient to cover the neck of the aneurysm and ensure adequate adhesion. The number of PEDs deployed and the use of adjunctive coils were determined by the surgeon. Coil packing was generally stopped once obvious flow stasis within the aneurysm was observed. After the endovascular procedure, dual antiplatelet therapy was continued for 6 months, after which acetylsalicylic acid was continued lifelong.
Patients treated with coiling underwent the procedure under general anesthesia. Heparin (70 U/kg) was administered intravenously throughout the procedure. Stent-assisted coiling was preferred for patients with wide-necked aneurysms. The stents used in conventional therapy included Low-profile Visualized Intraluminal Support (LVIS™, Microvention; Tustin, CA, USA), Enterprise (Codman Neurovascular; Raynham, MA, USA), and Neuroform (Stryker Neurovascular; Fremont, CA, USA). When stent deployment was planned, patients received dual antiplatelet therapy (100 mg/day acetylsalicylic acid and 75 mg/day clopidogrel) for 5 days prior to the procedure. Coil packing was performed until the aneurysm was completely occluded or there was no space for additional coils. After the endovascular procedure, if a stent had been deployed, dual antiplatelet therapy was continued for 3 months, followed by acetylsalicylic acid for up to 6 months.
Follow-up
Patients who underwent PED treatment and endovascular coiling were followed up using digital subtraction angiography. The angiographic outcomes of aneurysms were categorized as complete occlusion, near complete occlusion (≥90%), or incomplete occlusion (<90%). The angiographic outcomes of branches were classified as patent or occluded. An aneurysm neck-type incorporated branch refers to a branch vessel whose ostium is completely or partially located at the aneurysm neck, with anatomical fusion between the root of the branch vessel and the aneurysm neck, such that the diameter of the aneurysm neck includes the width of the branch ostium. An aneurysm sac-type incorporated branch refers to a branch vessel whose ostium originates directly from the aneurysm sac wall, with its root having no direct connection with the aneurysm neck and attached solely to the dilated aneurysm sac.
All classifications were independently determined by two attending physicians with more than 5 years of clinical experience in neurointervention (neither participated in the treatment of the included cases). They made branch type classification for the three-dimensional digital subtraction angiography (3D-DSA) images of all cases based on the abovementioned criteria. During the assessment, there was no information exchange between the two physicians, and both were blinded to the grouping or prognosis of the cases. For cases in which the two evaluators provided inconsistent determination results (6 cases, accounting for 4.5% of total cases), a chief physician specializing in neurointervention (with more than 10 years of experience in aneurysm imaging evaluation) conducted a review as a third party. The final unified classification conclusion was reached after clarifying the branch type with the assistance of image post-processing techniques.
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) 21.0 software (IBM; Armonk, NY, USA). Continuous variables were presented as mean ± SD and analyzed using an unpaired independent sample t-test. Categorical variables were presented as frequencies and analyzed using the χ² test or Fisher’s exact test when the expected frequency was <5. A p-value of <0.05 was considered statistically significant.
Results
Patient demographics and aneurysm characteristics
The demographic data and aneurysm characteristics of the 132 patients are summarized in Table 1. Of these, 63 patients were treated with PED and 69 with endovascular coiling (with or without stent assistance). Patients in both groups had comparable age (p = 0.538), sex ratio (p = 0.649), dome-to-neck ratio (p = 0.997), and follow-up duration (p = 0.735). There were no significant differences in aneurysm size (p = 0.61) and neck size (p = 0.078) between the two groups.
Patient demographics and aneurysm characteristics for cases treated with pipeline embolization devices and coiling.

PED group included patients treated with a pipeline embolization device alone and those treated with PED in combination with adjunctive coils.
PED: pipeline embolization devices.
Procedural details and procedure-related complications
The PED was successfully deployed in all 63 procedures. Two aneurysms were treated with double PEDs and the remaining with a single PED. Adjunctive coils were deployed in 37 of the 63 procedures, and one aneurysm required balloon assistance. One patient (1.6%) in the PED group experienced a procedure-related complication (ischemic event). In this case, the aneurysm incorporated the ophthalmic artery and was treated with a PED–coil strategy. The patient developed headache, nausea, and vomiting upon awakening from general anesthesia. Magnetic resonance imaging revealed focal ischemia. The incorporated ophthalmic artery remained patent at immediate angiography and during latter follow-up. The ischemia area was not supplied by ophthalmic artery, therefore, we considered the focal ischemia to be unrelated to the incorporated branch. In the coiling group, 38 procedures were performed with stent-assisted coiling. No patients in this group developed procedure-related complications. The average packing densities in the PED and coiling groups were 9.46% ± 7.42% and 25.41% ± 13.79%, respectively. Packing density in the coiling group was significantly higher than that in the PED–coil group (p < 0.001).
Angiographic outcomes
The mean follow-up durations of the PED and coiling groups were 12.39 ± 1.12 months and 12.51 ± 1.47 months, respectively (p = 0.584). A total of 26 (41.3%) aneurysms in the PED group and 44 (63.8%) in the coiling group achieved complete or near complete occlusion (p = 0.009). At follow-up, 16 branches (25.4%) in the PED group and 12 branches (17.4%) in the coiling group were occluded (p = 0.523) (Table 2). In the comparison between the PED and stent-assisted coiling groups, the stent-assisted coiling group had a higher rate of complete or near complete occlusion of aneurysms (p = 0.004); however, there was no significant difference in terms of the rate of branch occlusion between the two groups (p = 0.617). (Table 3). In the comparison between the PED–coil and PED alone groups, PED–coil achieved more complete or near complete occlusions of aneurysms and branch occlusion (Table 4). Among the 27 occluded branches, 25 (92.6%) originated from the aneurysm sac and 2 (7.4%) from the aneurysm neck (p < 0.001) (Table 5).
Comparison of angiographic outcomes and procedure-related complications between the PED and coiling groups.

PED group included patients treated with a pipeline embolization device alone and those treated with PED in combination with adjunctive coils.
PED: pipeline embolization devices.
Comparison of angiographic outcomes and procedure-related complications between the PED and stent-assisted coiling groups.

PED group included both patients treated with a pipeline embolization device alone and those treated with PED in combination with adjunctive coils.
PED: pipeline embolization devices.
Comparison of angiographic outcomes and procedure-related complications between PED–coil and PED alone.

PED: pipeline embolization devices.
Origins of the occluded branches and their status at follow-up.

Discussion
Endovascular treatment of intracranial aneurysms with an incorporated branch is challenging, as the presence of incorporated branches may reduce the effectiveness of the coiling and PED treatments. Previous studies have reported poor outcomes in such cases. Trivelato et al. 13 reported that after PED deployment, complete occlusion was more common in aneurysms without an incorporated branch (84% vs. 40% at 6 months). They concluded that aneurysms with an incorporated branch are less likely to achieve complete occlusion at 6 months or 1 year after PED treatment. Moshayedi et al. 12 reported that only 13% of aneurysms with an incorporated branch achieved complete occlusion after PED treatment at a mean follow-up of 18.3 months, compared with 68% of aneurysms without an incorporated branch. Kawabata et al. 10 reported that 80.7% of aneurysms treated with coiling achieved near complete occlusion or displayed a neck remnant.
It is crucial for clinicians to compare the effectiveness of these two treatment strategies to determine the preferable approach for treating intracranial aneurysms with an incorporated branch. At the same time, preservation of incorporated branches must be considered, particularly when the branches have limited collateral circulation.
Our study demonstrated that, in the treatment of aneurysms with an incorporated branch, coil embolization achieved higher aneurysm occlusion rates than PED treatment; however, both groups showed comparable branch occlusion rates. When comparing the PED (with or without coil) group with the stent-assisted coiling group, we found that stent-assisted coiling resulted in higher aneurysm occlusion rates, with incorporated branch occlusion remaining comparable between the two groups. PED–coil treatment resulted in higher rates of complete or near complete aneurysm occlusion and comparable rates of branch occlusion compared with those observed with PED alone. To the best of our knowledge, this is the first study to directly compare the treatment effects of coiling and PED treatment as well as to focus on the patency of incorporated branches.
PED treatment is generally considered superior to coiling for intracranial aneurysms; 15 however, the situation differs for aneurysms with incorporated branches because such aneurysms may not achieve complete occlusion after PED deployment (Figure 1). In contrast, coiling can achieve complete occlusion of the aneurysm and, in some cases, remodel the incorporated artery (Figure 2), likely due to the coil packing strategy. During endovascular coiling, coils were densely packed to exclude blood flow from the aneurysm sac. This dense embolization neutralizes the hemodynamic alteration caused by the incorporated branch. In contrast, during PED treatment, the coil packing process was stopped once obvious flow stasis in aneurysm sac was observed. Furthermore, 26 (41.3%) patients achieved obvious flow stasis in the aneurysm sac before coil packing; therefore, no coils were placed in these cases. The limited numbers of coils in the aneurysm sac may explain the lower efficacy observed in the PED group. Park et al. 16 compared retreatment rates between PED alone and PED–coil groups and found that adjunctive coil embolization resulted in a significantly lower retreatment rate than that with PED alone. However, increasing the number of coils may elevate the risk of incorporated branch occlusion and ischemic events. Park et al. 17 compared PED with or without adjunctive coil embolization and reported that PED with coil embolization was associated with higher neurological morbidity. Thus, the advantages and disadvantages of endovascular therapy should be carefully weighed. The overall occlusion rate of endovascular therapy for aneurysms with an incorporated branch remains unsatisfactory. We believe that the presence of incorporated branches prevents sufficient reduction of flow velocity in aneurysms, limiting aneurysm occlusion. This hypothesis warrants verification through computational fluid dynamic simulation in future studies. In a previous study, we18,19 investigated the hemodynamic influences of PED on covered branches and found that, although flow velocity in covered branches was not significantly changed, flow velocity in aneurysms significantly decreased after PED treatment. The hemodynamic conditions of branches arising from the aneurysm sac after coiling and PED deployment remain uncertain and warrant further investigation. Moreover, the suitability of endovascular treatment for aneurysms with an incorporated branch should be reconsidered. A comparative analysis of treatment outcomes of clipping and endovascular treatment is essential. Additionally, new techniques or devices may help improve aneurysm occlusion rates, highlighting the need for further exploration.

Aneurysm with an incorporated anterior cerebral artery treated with a pipeline embolization device (PED). (a) Right internal carotid angiogram shows a saccular aneurysm (arrow) with the anterior cerebral artery arising from the aneurysm sac; (b) fluoroscopic image shows the PED deployment site and (c) control angiography at 8-month follow-up shows incomplete aneurysm occlusion, with the anterior cerebral artery remaining patent.
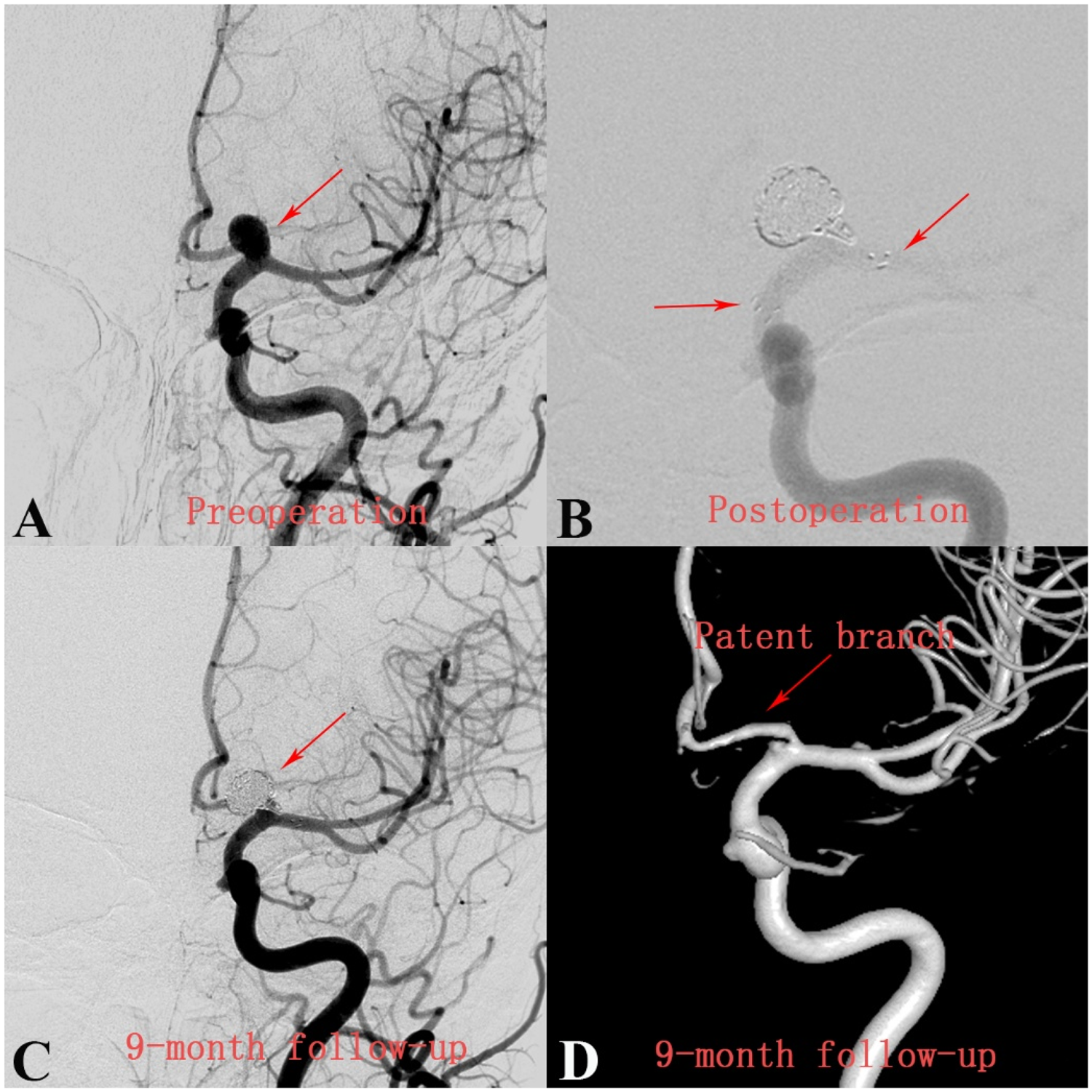
Aneurysm with an incorporated anterior cerebral artery treated with stent-assisted coiling. (a) Left internal carotid angiogram shows a saccular aneurysm (arrow) with the anterior cerebral artery arising from the aneurysm sac; (b) fluoroscopic image shows the site of the stent and packed coil within the aneurysm; (c) control angiography at 9-month follow-up shows complete aneurysm occlusion and a remodeled anterior cerebral artery; and (d) three-dimensional model reconstructed from a digital subtraction angiography image shows the remodeled anterior cerebral artery 9 months after treatment.
Regarding the fate of incorporated branches, our results showed that coiling and PED treatment had comparable outcomes. Both approaches have advantages and limitations in preventing branch occlusion. PED diverts blood flow away from the aneurysm, but limited coil packing may not sufficiently reduce aneurysmal blood flow. In contrast, endovascular coiling with dense coils can slow aneurysmal inflow but lacks a flow-diverting effect. Consequently, both groups exhibited similar rates of branch occlusion. Our results also indicated that branches arising from the aneurysm sac are more prone to occlusion than those originating from the aneurysm neck. Although the overall branch occlusion rate did not differ significantly between the two strategies, we observed that when branches arose from the aneurysm neck, coiling could remodel the incorporated branch and achieve aneurysm occlusion (Figure 2).
This study has several limitations. First, only 63 aneurysms with an incorporated branch treated with PED and 69 treated with coiling were included, warranting future studies with larger sample sizes. Second, hemodynamic factors play a critical role in aneurysm and incorporated branch occlusion, highlighting the need for studies focusing on computational fluid dynamics. Third, significant differences in aneurysm size existed between the treatment groups. PED was preferentially used for larger or complex aneurysms (mean size, 9.1 mm vs. 7.9 mm in coiling group; p = 0.061), which may have contributed to the lower occlusion rate observed in the PED group. Future studies using propensity score matching are needed to reduce this bias. Finally, long-term follow-up results are lacking, and studies with extended follow-up are warranted.
Conclusion
This study compared the efficacy of coiling and PED in the treatment of aneurysms with an incorporated branch. Compared with PED, endovascular coiling, particularly stent-assisted coiling, may achieve higher rates of complete or near complete aneurysm occlusion without a significant increase in branch occlusion. Branches arising from the aneurysm sac may be more prone to occlusion than those originating from the neck. For aneurysms with an incorporated branch that is sacrifiable (i.e. its loss would not result in significant neurological dysfunction), stent-assisted coiling may be an appropriate treatment option. However, these findings are limited by the retrospective design and single-center sample and should be validated in multicenter prospective studies.
Footnotes
Acknowledgments
None.
Author contributions
Dadong Ding: Conceptualization, Data curation, Formal analysis, and Writing–original draft; Chao Wang: Methodology, Validation, Investigation, and Writing–review and editing; Da Wu: Supervision, Project administration, and Writing–review and editing. All authors have read and approved the final version of the manuscript.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no conflicts of interest. No financial or nonfinancial support was received from any third party for the conduct of this study.
Funding
None.