
Abstract
Objective
The role of autologous bone grafting in medial open-wedge high tibial osteotomy remains controversial. This study compares the clinical and radiological outcomes of open-wedge high tibial osteotomy performed with and without autologous bone grafting.
Methods
This nonrandomized two-center prospective cohort study recruited 73 patients who underwent open-wedge high tibial osteotomy. The radiological union status was assessed using a modified van Hemert scoring system and modified Radiological Union Scale for Tibia score. Clinical measures included the International Knee Society Score, clinical union time, and postoperative complications with a minimum 1-year follow-up.
Results
Radiological union at 1 year was significantly higher in the graft group, with 80.0% achieving complete union across all five zones compared with 44.7% in the no-graft group (p = 0.002). However, no significant differences were observed in the postoperative International Knee Society Scores (168 ± 15.7 vs. 168 ± 14.6; p = 0.920), hip–knee–ankle angle correction (181° in both groups; p = 0.687), or clinical union time (10.2 ± 1.77 vs. 10.7 ± 1.35 weeks; p = 0.133).
Conclusion
Autologous iliac crest bone grafting significantly improved the radiological healing in open-wedge high tibial osteotomy without increasing the incidence of complications.
Introduction
In 2019, an estimated 528 million individuals were affected by osteoarthritis (OA), marking a 113% rise from 1990. 1 OA, particularly knee OA, is a progressive, multifactorial condition associated with significant pain and disability. 2 Knee OA accounts for approximately four of five OA cases worldwide, and its prevalence increases with aging and obesity. 3 Consistent with this global trend, 21% of individuals aged 35–45 years in Iraq have knee OA, with the prevalence rising up to 53% among those with a body mass index (BMI) >30 kg/m2. 4
Biomechanically, the knee joint is subject to considerable stress, with loads during routine activities exceeding several times the body weight. 5 This stress is disproportionately distributed across the medial and lateral compartments, based on the tibiofemoral alignment and activity type.6,7 Notably, approximately 75% of the load passes through the medial tibial plateau during a single-leg stance, predisposing the knee to early degeneration. 8 Consequently, the development of medial compartment OA is often accompanied by varus deformity, which exacerbates disease progression by further shifting the load medially.9,10
To treat this vicious cycle, high tibial osteotomy (HTO), specifically open-wedge HTO (OWHTO), has been considered a joint-preserving procedure of choice for young, active adults with isolated medial disease. OWHTO has certain benefits over closed-wedge HTO, including preservation of bone stock, more precise control of correction, and lower risk of neurovascular complications. 11 However, the long-term outcomes remain variable. Survival rates at 15–20 years postoperatively range from 40% to 85% and are influenced by patient-related factors such as advanced age, elevated BMI, and baseline functional scores. 12 Furthermore, the success of OWHTO depends not only on accurate alignment correction but also on optimal healing of the osteotomy gap.
The proximal tibial gap has fueled the ongoing debate regarding the need for and form of bone grafting. A meta-analysis by Han et al. 13 revealed a lack of superiority of any grafting modality in terms of radiological outcomes or stability of correction. Likewise, Mao et al. 14 noted that although autografts exhibited a superior bone union score compared with other techniques, they did not provide any benefit in terms of functional status or rate of complications at the 1-year follow-up. The current study prospectively compared the clinical and radiological outcomes between patients who underwent OWHTO with and without autologous bone grafts to support more informed surgical decision-making.
Methods
This nonrandomized prospective cohort study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 15 We prospectively enrolled patients undergoing medial OWHTO, with or without autologous bone grafting, for symptomatic medial compartment OA with varus alignment between July 2021 and 2024 at two orthopedic centers in Erbil City, Iraq.
Complete five-zone radiological union at 1 year was designated as the primary outcome, while secondary outcomes included the modified Radiological Union Scale for Tibia (mRUST) score, clinical union time, and International Knee Society Score (IKSS).
Study design and eligibility criteria
The inclusion criteria were as follows: (a) patients aged 18–60 years; (b) those with isolated medial compartment OA with varus deformity; and (c) a planned osteotomy gap ≤15 mm. Exclusion criteria were as follows: (a) history of high tibial osteotomy; (b) history of knee infection; (c) preoperative restricted knee range of motion (extension deficit >10° and flexion <100°); and (d) radiographic evidence of severe grade OA based on Kellgren–Lawrence scale in the lateral or patellofemoral compartments. 16
No formal a priori sample size calculation was performed. The sample size of 73 patients reflects all eligible cases meeting the inclusion criteria over the study period across two centers. Although the study was primarily powered to detect differences in radiological union, it may be underpowered for detecting less frequent secondary outcomes such as complications.
Preoperative planning
All patients underwent standardized full-length anteroposterior (AP) standing radiographs. Mechanical axis deviation, correction angle, joint line convergence angle, and osteotomy gap were assessed using Bone Ninja App (version 5.0) on iOS and GNU Image Manipulation Program (GIPM; version 2.10). Surgical planning included defining the cutting angle, lateral hinge position, and distraction parameters. Patients were assigned to one of the following two groups: no-graft group underwent OWHTO without grafting, while the graft group received an additional autologous iliac crest bone graft. Corticocancellous bone was harvested from the ipsilateral iliac crest in patients receiving autologous bone grafts. The graft material was shaped to fit the osteotomy gap and specifically positioned to support zones 4 and 5, enhancing central and posterior healing.
Group allocation
Patients were prospectively assigned to either the graft or no-graft group based on the operating surgeon’s preference. All procedures were performed by two independent surgical teams, each with more than 10 years of experience in osteotomy procedures, across two separate hospitals.
Surgical technique
The patient was placed in the supine position on the operating table, and a tourniquet was applied to the proximal thigh. An oblique medial skin incision was made, extending posteriorly just below the joint line and then directed anteriorly and inferiorly to a point just below the tibial tuberosity. The pes anserinus was identified and elevated. A biplanar medial OWHTO was performed using an oscillating saw and osteotomes. The osteotomy was initiated 3–4 cm below the medial joint line toward the tip of the fibular head. The medial wedge was gradually opened using a bone spreader until the desired correction (as determined via preoperative planning) was attained. In the no-graft group, no bone graft was used, whereas the graft group received an autogenous bone graft harvested from the ipsilateral iliac crest. The osteotomy site was stabilized using a TomoFix plate or an equivalent locked medial proximal tibial plate. Wound closure was performed in layers. Apart from mild pain at the iliac crest during the first 2 postoperative months, which did not require intervention, no complications were observed at the bone graft donor site.
Postoperative rehabilitation
The operated limb was elevated postoperatively. No prophylactic anticoagulation therapy was administered. Patients were allowed non–weight-bearing or toe-touch weight-bearing for 6 weeks, with free range of motion encouraged during this period. Gradual progression to full weight-bearing was initiated subsequently as per the patient’s tolerance.
Radiological outcomes
Standardized radiographic assessments were conducted using full-length AP standing radiographs of the lower extremity as well as AP and lateral knee radiographs, obtained at three time points: (a) preoperatively; (b) immediately postoperatively; and (c) at the 1-year follow-up. The AP standing radiographs of the lower extremity were acquired with the knee in full extension and the patella oriented forward at shoulder-width stance, ensuring consistent weight-bearing alignment across all images.
To evaluate the bone healing pattern within the osteotomy gap, a digitalized triangular template was superimposed on the AP radiographs, delineating the osteotomy margins. This triangle was subdivided into five equal zones, each representing 20% of the osteotomy length measured from the lateral apex toward the medial cortex. 17 Bone union progression was quantified by assessing the extent of callus filling within each zone, beginning from the lateral side and advancing medially. A minimum of 50% callus bridging within a zone was considered indicative of mechanical stability in that segment. 17
The modified van Hemert scoring system was employed to grade bone union within each of the five zones, providing a standardized, semiquantitative assessment of osteogenesis across the osteotomy interface. 18
Radiological bone healing at the osteotomy site was also assessed using an mRUST score adapted for OWHTO, evaluating bridging callus in four cortices (anterior, posterior, medial, and lateral) on the AP and lateral radiographs. A score of ≥11 was considered the minimum threshold for satisfactory bone union. 19
Radiological union was evaluated on standardized AP and lateral radiographs at 6 weeks, 3 months, 6 months, and 12 months postoperatively. Union was defined as bridging trabeculae visible across at least three out of four cortices. Particular attention was given to healing in zones 4 and 5 of the osteotomy gap, as these regions typically demonstrate slower consolidation and are critical for mechanical stability.
Clinical assessment
Clinical outcomes were evaluated preoperatively and at designated follow-up intervals using the IKSS, a validated tool for assessing knee function and patient-reported outcomes. Clinical union was defined as the absence of pain and tenderness during examination, accompanied by the ability to ambulate without discomfort. This assessment was systematically performed at each follow-up visit.
All complications encountered during the perioperative and postoperative periods were meticulously recorded. Intraoperative complications included events such as lateral cortical breaches and unicondylar fractures, both classified as technical complications occurring during surgery. Postoperative complications monitored throughout the follow-up period included superficial and deep surgical site infections, deep vein thrombosis (DVT), hematoma formation, restricted range of motion, and loss of correction (LOC). LOC was specifically defined as a deviation exceeding 3° in the hip–knee–ankle (HKA) angle between the immediate postoperative and final follow-up radiographs, suggesting a loss of alignment correction in the lower limb.
Donor site morbidity was assessed clinically during routine follow-up visits. Patients were specifically questioned regarding pain, tenderness, infection, or sensory disturbance at the iliac crest. No major complications were recorded, and mild donor site pain resolved spontaneously within 2 months in all cases.
Standardization of surgical and assessment protocols
All procedures were performed by two independent surgical teams, each with extensive and comparable experience in OWHTO. The operative technique was standardized across both groups. Uniform preoperative planning, operative technique, fixation methods, and postoperative rehabilitation protocols were applied to all patients. Radiological union was assessed independently by two blinded musculoskeletal radiologists using validated scoring systems (modified van Hemert and mRUST). In case of disagreement, consensus was reached to minimize subjectivity.
Statistical analysis
All statistical analyses were conducted using Jamovi software (version 2.3; The Jamovi Project; Sydney, New South Wales, Australia). Descriptive statistics were reported as means, standard deviations, medians, and ranges for continuous variables and as frequencies and percentages for categorical variables. Group comparisons between the graft and no-graft groups were performed using independent samples t-tests or Mann–Whitney U tests for continuous variables as well as chi-square or Fisher’s exact tests for categorical variables, as appropriate. Statistical significance was set at p < 0.05.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Medical Research Scientific & Ethics Committee of the Kurdistan Higher Council for Medical Specialties, Kurdistan Regional Government–Iraq, Ministry of Higher Education and Scientific Research (Meeting Code: 896; Date: 22/06/2021). All participants were provided with written information regarding the study and gave written informed consent prior to participation. Confidentiality and anonymity were maintained throughout the study.
Results
Baseline characteristics
The baseline demographic and clinical characteristics were largely comparable between the graft (n = 35) and no-graft (n = 38) groups (Table 1). The mean age of the patients was slightly higher in the graft group than in the no-graft group (42.8 ±8.68 vs. 40.6 ± 11.8 years); however, the difference was not statistically significant. Female patients predominated in both groups (65.7% vs. 63.2%). Right-sided involvement was slightly more common in both groups (62.9% vs. 63.2%). BMI values were comparable between the two groups (27.1 ± 4.31 vs. 27.1 ± 4.52 kg/m2), indicating similar baseline body composition. Prior surgery and history of trauma were infrequent and similarly distributed. Notably, the prevalence of osteopenia was higher in the graft group than in the no-graft group (37.1% vs. 31.6%). Additionally, a greater proportion of patients in the no-graft group reported isolated medial knee pain (68.4% vs. 54.2%). The distribution of Kellgren–Lawrence grades revealed a trend toward milder OA severity in both cohorts, with grade I being the most frequent. Comorbidities such as heart disease, malnutrition, anemia, and renal or rheumatological conditions were absent across both groups.
Distribution of baseline demographic, clinical, and laboratory characteristics among study participants.

BMI: body mass index; DEXA: dual-energy X-ray absorptiometry; OA: osteoarthritis.
Radiographic and clinical outcomes
Both groups demonstrated similar improvements in alignment (Table 2), with no clinically meaningful difference in HKA post angles (graft group: 181° ± 1.05° vs. no-graft group: 181° ± 2.2°). Medial gap measurements were similar between the two groups (11.6 ± 2.13 mm vs. 11.6 ± 2.05 mm). Functional recovery, as measured by IKSS, demonstrated no observable difference postoperatively (graft group: 168 ± 15.7 vs. no-graft group: 168 ± 14.6), confirming equivalent outcomes in joint function and pain resolution regardless of graft use.
Summary of the radiographic and clinical characteristics (graft vs. no-graft groups).

HKA: hip–knee–ankle; IKSS: International Knee Society Score.
Postoperative complications and surgical interventions
Both groups were subjected to identical fixation methods using locked plates. The incidence of superficial and deep surgical site infections was comparable between the two groups (Table 3). Notably, the incidence of mechanical complications, including lateral cortex fractures (8.6% vs. 5.3%) and LOC (5.7% vs. 7.9%), was low and comparable between the two groups. The use of postoperative drains was more common in the no-graft group (47.4% vs. 31.4%), but without a clear association with the infection or hematoma rates. Apart from mild pain during the first 2 postoperative months, donor site morbidity was not noted in any case.
Summary of postoperative complications, surgical interventions, and clinical outcomes among patients.

Radiological and clinical union outcomes
At 1-year postoperatively, complete radiological union (defined as bridging in all five zones) was achieved more frequently in the graft group (28/35; 80.0%) than in the no-graft group (17/38; 44.7%) (p = 0.002) (Table 4) (Figures 1 and 2). A mRUST score of ≥11 for OWHTO was achieved postoperatively between 8 and 16 weeks and between 10 and 20 weeks in the graft and no-graft groups, respectively. The graft group achieved clinical union at a mean duration of 10.2 ± 1.77 weeks, compared with 10.7 ± 1.35 weeks in the no-graft group. The median time was 10 weeks in both cohorts.
Frequency distribution of radiological union outcomes following osteotomy.

Df: degrees of freedom; CI: confidence interval.

Full-length standing anteroposterior radiographs of the lower limbs (open-wedge high tibial osteotomy (OWHTO) without autologous graft). (a) Preoperative image demonstrating right-sided varus malalignment in a patient with isolated medial compartment osteoarthritis and (b) postoperative radiograph of the same patient 1 year following medial OWHTO without autologous graft on the left side, showing restored mechanical axis alignment and stable fixation with a locking plate construct.

Full-length standing lower limb radiographs demonstrating mechanical axis correction following medial open-wedge high tibial osteotomy (OWHTO) with autologous bone graft. (a) Preoperative radiograph of a patient in the graft group, showing left-sided varus malalignment and medial compartment osteoarthritis and (b) one-year postoperative radiograph of the same patient following OWHTO with autologous iliac crest bone grafting, revealing restored mechanical alignment and satisfactory fixation.
Comparative outcome analysis
Radiological union at 1 year was significantly higher in the graft group (χ2 = 8.52, p = 0.014), with 80% achieving full union, compared with 45% in the no-graft group (Figure 3). However, the clinical union time did not vary significantly between the two groups (Welch’s t = 1.52, p = 0.133).
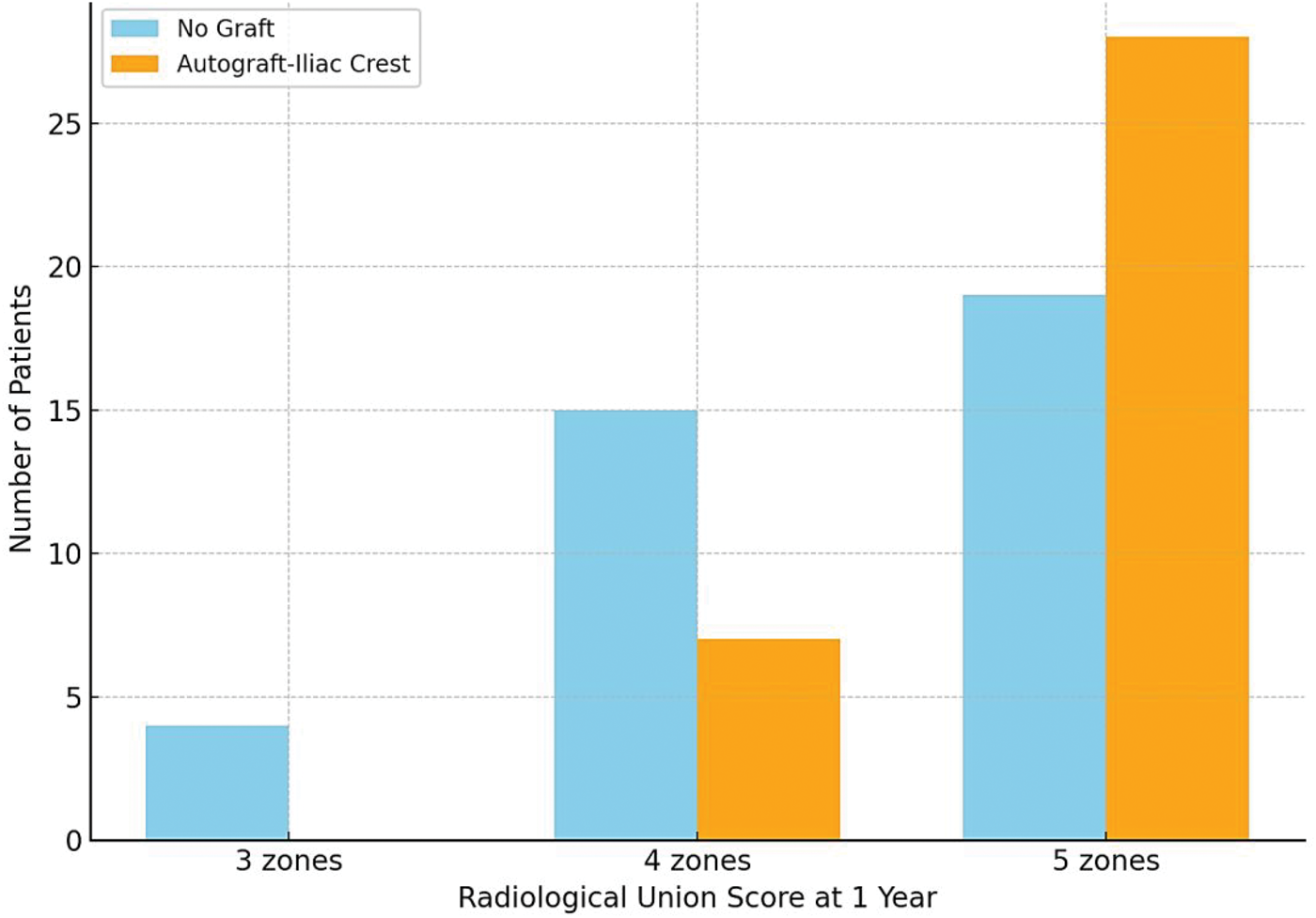
Bar plot illustrating the distribution of patients achieving radiological union across zones 3, 4, and 5 in the graft (autograft–iliac crest) versus no-graft groups.
No significant difference was observed in the HKA angle between the graft and no-graft groups (p = 0.687). Additionally, no statistically significant difference was observed in the IKSSs between the graft and no-graft groups (p = 0.920). No significant association was observed between graft use and the occurrence of superficial surgical site infections (p = 0.634).
A 2 × 2 chi-square test revealed a statistically significant association between graft use and radiological union at 1 year (χ2 = 9.58, p = 0.002). Patients who received autologous iliac crest grafts were significantly more likely to achieve complete radiological union (28/35; 80%) than those in the no-graft group (17/38; 45%).
Radiological union was also analyzed in relation to clinical and demographic variables (Table 5). Among these, the only statistically significant association was observed with graft type. Patients who underwent OWHTO with autologous iliac crest grafting demonstrated a significantly higher rate of complete radiological union than those in the no-graft group (80% vs. 45%; χ2 = 9.58, p < 0.01). No significant associations were observed between radiological union and other factors such as sex, surgical side, smoking status, previous trauma, previous surgery, or Kellgren–Lawrence OA grade.
Association between clinical and radiological factors and radiological union status.

OA: osteoarthritis.
Radiological union at 1 year was significantly more frequent in the graft group than in the no-graft group (80.0% vs. 44.7%; odds ratio (OR): 4.94, 95% confidence interval (CI): 1.74–14.07; p = 0.002). In contrast, the incidence of superficial infection was comparable between the two groups (17.1% vs. 13.2%; OR: 1.37, 95% CI: 0.38–4.95; p = 0.634). Clinical union time was slightly shorter with grafting (10.2 ± 1.77 vs. 10.7 ± 1.35 weeks); however, this difference did not reach statistical significance (mean difference: −0.5 weeks, 95% CI: −1.1 to 0.1; p = 0.128) (Table 6).
Comparative outcomes of OWHTO with and without autologous iliac crest grafting.

OWHTO: open-wedge high tibial osteotomy; OR: odds ratio; CI: confidence interval; IKSS: International Knee Society Score.
Subgroup analysis
Stratified chi-square analyses revealed that the positive association between autologous grafting and complete radiological union was more pronounced in females (χ2 = 5.84, p = 0.016), where 78% of grafted cases achieved complete union compared with 43% in the no-graft group. A similar trend was observed (83% vs. 50%) among males; however, the difference did not reach statistical significance (χ2 = 3.17, p = 0.075), likely due to the limited sample size. Stratified analysis by surgical side revealed that autologous grafting was significantly associated with higher rates of complete radiological union in both the left (χ2 = 5.57, p = 0.018) and right knees (χ2 = 5.12, p = 0.024). In left-sided surgeries, 77% of patients who underwent grafting achieved complete union, compared with 31% in the no-graft group. Similarly, in right-sided procedures, 82% of grafted cases demonstrated union versus 50% without grafting. Stratification by smoking status demonstrated a significant association between graft use and complete radiological union in both smokers (χ2 = 4.22, p = 0.040) and nonsmokers (χ2 = 5.72, p = 0.017). Among smokers, 87.5% of patients who received grafts achieved complete union compared with 40% in the no-graft group. Among nonsmokers, the respective rates were 77.8% vs. 46.4%.
Discussion
The significance of this study lies in its contribution to resolving a long-standing debate regarding the need for bone grafting in OWHTO. Despite no observable differences in the functional scores or mechanical alignment correction, the markedly higher rate of complete radiological healing in the graft group underscores the biological benefit of autografts in promoting osteogenesis across the osteotomy site. These findings suggest that although grafting may not be indicated in all patients, it holds clinical value in cases where accelerated or more reliable bone healing is desired. However, the nonrandomized design and surgeon-based group allocation may introduce selection bias, limiting internal validity. Although baseline characteristics were comparable, unmeasured confounders cannot be ruled out. This limitation should be considered when interpreting the findings.
At 1 year, a substantially higher percentage of patients within the graft group exhibited complete radiological union in all five zones (80% vs. 45%) (p = 0.014), as evaluated using modified van Hemert scoring. This radiological benefit was not accompanied by any increase in the incidence of complications, further affirming the graft’s osteogenic efficacy and safety. These findings are supported by compelling data from a prospective, randomized controlled trial by Fucentese et al. (2019), 20 which demonstrated that autograft harvested from the iliac crest significantly enhanced osseous gap healing, as evidenced by high-resolution computed tomography. The study reported a healing rate of 91.5% at 12 months in the graft group vs. 59.1% in the control group (p < 0.001), establishing bone grafting as an independent predictor of enhanced bone formation. Similarly, Ulucaköy et al. (2020) 21 found that autologous grafting significantly shortened the union time, with earlier consolidation observed as early as in the sixth postoperative week in the graft group (p = 0.006). The lack of significant associations with demographic factors (e.g. age, sex, and smoking) suggests that the observed radiological advantage of autologous grafting may be broadly applicable across patient subgroups.
Postoperative IKSSs were identical between the two groups (graft group: 168 ± 15.7 vs. no-graft group: 168 ± 14.6; p = 0.920), and the HKA alignment correction was equally achieved (181° in both groups; p = 0.687). Zorzi et al. (2011), 22 in a randomized trial of 46 cases, reported no significant difference in the time to bone union or mechanical correction angle between grafted and non-grafted cohorts. Collectively, these data suggest that although autografting supports radiological consolidation, it does not provide a functional or alignment advantage in the short-to-mid-term, reinforcing the rationale for selective use of bone grafting in OWHTO.
Although autologous iliac crest bone grafting exhibits a modest influence on clinical union timing, our study observed a slight but not statistically significant reduction in the time to clinical union with the use of grafts. This observation aligns with the findings of Kang et al. (2022), 23 who emphasized that mechanical alignment and stability of fixation are more critical than grafting alone for accelerating functional outcomes. Furthermore, Palmer et al. (2024) 24 highlighted that rigid fixation and modern plating techniques, including biplanar osteotomy and locking plate constructs, already provide a stable healing environment that may diminish the additive clinical benefit of grafts in certain scenarios. Although bone grafts may support osteogenesis, the difference in soft tissue healing, load-bearing protocols, and individual biological variability may explain why their contribution to earlier clinical union is marginal.
Although autologous iliac crest grafting significantly improved radiological union in OWHTO, the overall complication rates remained low and comparable between the graft and no-graft groups. Notably, no statistically significant association was found between graft use and increased surgical site infections (p = 0.634), deep infections, or delayed healing, confirming the safety of autograft application. This is consistent with the findings by Guarino et al. (2023), 25 who reported that although complications such as lateral hinge fractures and infections are inherent risks in OWHTO, these did not significantly vary based on the grafting status or technique employed. Correspondingly, Predescu et al. (2021) 26 reported 2 cases of Takeuchi type 3 fractures and 1 case of delayed healing among 25 patients treated with patient-specific instrument-guided OWHTO without a case of deep infection. In particular, delayed healing could be attributed to excessive smoking rather than a procedural factor, affirming patient-specific risk for complications.
Subgroup analyses revealed that grafting conferred consistent radiological benefits across sex, surgical side, and smoking status, particularly among female patients and smokers. Additionally, patients who received grafts demonstrated reduced variability in clinical union across age groups. These findings suggest that autografting may offer particular value in patients at higher risk of delayed healing, such as older adults, smokers, or those with osteopenia.
A recent prospective study by Zehir and Alic (2023) 27 evaluated the functional and radiological outcomes of biplanar distal tubercle open-wedge high tibial osteotomy over a 5-year follow-up period. Their findings support the safety and long-term effectiveness of the technique, particularly in maintaining patellar height and avoiding patellofemoral joint complications. Although our study did not focus specifically on the patellofemoral outcomes, these results align with our conclusion that OWHTO can be optimized through surgical modifications and careful patient selection. Incorporating such data strengthens the evidence base supporting the evolution of HTO techniques to minimize morbidity and enhance joint preservation.
This study provides key information about the controversial use of bone grafts in medial OWHTO. The results demonstrated a significant radiological benefit from autologous iliac crest grafting, with no increase in complication rates, and no discernible functional benefit in terms of scores or restoration of alignment. Clinically, these findings support a selective grafting approach—reserving its use for patients at risk of delayed union rather than employing it in all cases. The strengths of this trial are its prospective design, standardized surgical technique, uniform follow-up, and comprehensive radiological assessment by both modified van Hemert and mRUST scoring systems.
Limitations
First, the relatively small sample size may have limited the statistical power to detect subtle differences in the secondary measures. Second, the study was nonrandomized, and group allocation was based on surgeon preference, which contributed to potential selection bias, limiting internal validity. Third, although the study was prospective, it lacked blinding of the outcome assessors, which could have introduced measurement bias, particularly in the radiographic scoring of union. Fourth, although the findings suggest comparable complication rates between the two groups, the conclusion regarding safety is constrained by the lack of systematic assessment of donor site morbidity following iliac crest harvesting. Moreover, the follow-up period was limited to 1 year, which may be inadequate for evaluating the long-term outcomes such as osteotomy survivorship, correction durability, or conversion to total knee arthroplasty.
Conclusion
This prospective study suggests that autologous iliac crest grafting in medial OWHTO enhances radiological union without increasing complication rates; however, it does not improve the functional outcomes or alignment. These findings support selective graft use in patients at risk of delayed healing, such as those with osteopenia or larger gaps. However, the lack of systematic donor site assessment and short follow-up limit broader conclusions regarding its safety and long-term benefit. Future research should evaluate whether improved radiographic healing leads to better joint preservation or reduced arthroplasty conversion. Until then, the decision regarding the use of grafting should be individualized based on patient-specific risk factors for delayed healing.
Footnotes
Acknowledgement
None.
Author contributions
Dedawan Namiq Rasul: Conception and design of the study; acquisition, analysis, and interpretation of data; drafting and critical revision of the manuscript; and approval of the final version; the author is accountable for all aspects of the work.
Availability of data and materials
The dataset of this research is available from the corresponding author upon reasonable request.
Consent for publication
The patient provided written informed consent prior to anonymous publication of their data.
Clinical trial registry
Not applicable.
Declaration of conflicting interests
The author declares no conflict of interest or competing interests.
Ethics approval and consent to participate
This study followed the tenets of the Declaration of Helsinki. Ethical approval was obtained from the Medical Research Scientific & Ethics Committee of the Kurdistan Higher Council for Medical Specialties (Meeting Code: 896; Date: 22/06/2021). Participants received study information and provided written consent.
Funding
The author did not receive any specific grant or financial support for the conduct of this study.