
Abstract
Background
To investigate post-traumatic growth and psychological resilience in adolescents with systemic lupus erythematosus and identify predictors of post-traumatic growth to inform targeted interventions.
Methods
We conducted a cross-sectional analysis of patients aged 12–18 years using validated measures: Post-Traumatic Growth Inventory and Resilience Scale for Chinese Adolescents. Statistical analyses, including correlation tests, multiple linear regression, subgroup comparisons, and mediation analysis, were performed to examine the roles of clinical characteristics and resilience in post-traumatic growth development.
Results
Among 104 participants (mean age, 14.46 ± 1.81 years; 66.35% (69/104) females), both scales exhibited high reliability (Post-Traumatic Growth Inventory: α = 0.917; resilience: α = 0.859). Resilience was strongly correlated with post-traumatic growth (r = 0.504, P < 0.001). Significant predictive factors included disease duration >1 year (β = 11.66), positive family relationships (β = 10.59), and higher family income (β = 3.11) (all P < 0.01). Resilience mediated 22.09% of the relationship between disease duration and post-traumatic growth (P = 0.042).
Conclusion
Post-traumatic growth is achievable in patients with childhood-onset systemic lupus erythematosus, driven by resilience, familial support, socioeconomic stability, and disease chronicity. These findings underscore the need for holistic interventions integrating psychosocial and clinical care to promote positive adaptation in adolescents with systemic lupus erythematosus.
Introduction
Childhood-onset systemic lupus erythematosus (cSLE) represents a multisystem autoimmune disorder characterized by the production of pathogenic autoantibodies, notably antinuclear antibodies, which drive inflammatory damage across multiple organs. 1 Epidemiological studies in China have estimated the prevalence of systemic lupus erythematosus (SLE) at 30–70 cases per 100,000 individuals, with cSLE accounting for 10%–20% of all SLE cases and constituting 15%–25% of pediatric rheumatic diseases.1,2 Compared with adult-onset SLE, cSLE manifests a more aggressive phenotype characterized by heightened disease activity; increased renal, hematological, and neuropsychiatric involvement; and accelerated organ damage progression. These factors collectively contribute to substantially elevated risks of disease-related disability, mortality, and treatment burden.3,4 Consequently, cSLE imposes substantial socioeconomic burdens on affected families and healthcare systems. The chronic and unpredictable course of SLE also inflicts considerable psychological distress. In adult SLE patients, the illness experience can be profoundly traumatic, with a recent study reporting that 31% of patients met the criteria for post-traumatic stress disorder, which was strongly associated with poorer quality of life. 5 Similarly, adolescents with cSLE frequently experience anxiety, depression, and social isolation, with reported rates ranging from 6.7% to 59% for depression and from 34% to 37% for anxiety.6,7 These overlapping yet distinct psychological challenges profoundly affect the quality of life of SLE patients, underscoring the critical need for a deeper understanding of their psychological adaptation.
The emerging construct of post-traumatic growth (PTG), defined as positive psychological transformation following significant adversity, offers a critical counterpoint to the prevailing pathology-focused narrative in pediatric rheumatology.8,9 PTG manifests through five interconnected domains: deepened interpersonal relationships, recognition of new life possibilities, enhanced personal strength, spiritual awakening, and heightened appreciation of existence.8,9 This transformative process transcends mere resilience or recovery, instead representing a reconfiguration of identity and worldview forged through the struggle with trauma. Neurocognitive research suggests that PTG arises from “cognitive–emotional wrestling,” wherein shattered core beliefs undergo iterative reconstruction through deliberate rumination and narrative development. 10 Although extensively documented in adult cancer survivors (prevalence: 53%–95%) and trauma victims, its relevance to adolescents with chronic illness remains underexplored.11–13 Adolescence constitutes a “window of opportunity” during which illness experiences may be integrated into evolving self-concepts, potentially catalyzing growth trajectories unavailable to mature adults with established identities.8,14,15
Psychological resilience, defined as the ability to adapt positively to adversity, is a potential factor promoting PTG.16,17 Contemporary models conceptualize resilience not as a fixed trait but as a neurobiologically mediated process that collectively buffers allostatic load. 18 In the context of pediatric chronic illness, resilience operates across multiple ecological levels involving individual, family, and community. 19 Crucially, resilience functions as the essential scaffold upon which PTG develops, enabling individuals to engage with, rather than avoid, trauma-related distress, thus transforming threat into challenge.20,21 However, research on the relationship between resilience and PTG in adolescents with cSLE remains limited, as most psychological studies in this population have predominantly focused on negative outcomes such as anxiety and depression.4,7
The present study addresses critical gaps at the intersection of developmental psychology, pediatric rheumatology, and cultural medicine. First, although investigations of PTG are increasing in oncology and trauma literature, autoimmune conditions—particularly those with childhood onset—remain conspicuously underexplored. The distinct illness trajectory of SLE, characterized by unpredictable flares, treatment toxicity, and lifelong morbidity, may uniquely shape growth processes compared with time-delimited traumas such as natural disasters. Second, existing pediatric resilience research predominantly involves Western cohorts, neglecting cultural mediators that may profoundly influence adaptation mechanisms. Within China’s collectivist framework, family interdependence and filial piety norms likely modulate resilience expression differently than Western individualism. Third, no prior study has concurrently examined socioeconomic determinants, relational factors, and psychological assets within an integrated PTG prediction model for adolescents with cSLE. This study aimed to provide insights into the psychological adaptation of cSLE patients and inform targeted interventions that enhance resilience and promote PTG. The findings are expected to contribute to the development of personalized nursing care strategies, ultimately improving the overall well-being and quality of life of cSLE patients.
Materials and methods
Study design and setting
A cross-sectional observational study was conducted between January and December 2024 at the Department of Nephrology and Immunology and the Department of Rheumatology and Immunology. The results were reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 22
Participants
Participants were recruited using convenience sampling. Eligible participants included adolescents with SLE aged 12–18 years who were either outpatients or inpatients at the study site.
The inclusion criteria were as follows:
Confirmed clinical diagnosis of SLE fulfilling the 2019 European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) classification criteria; Disease duration ≥ 6 months; Ability to complete questionnaires independently or with minimal assistance; Informed consent provided by both the patient and at least one parent or legal guardian.
The exclusion criteria were as follows:
Unwillingness to participate; Presence of comorbidities interfering with assessment (e.g. severe psychiatric or neurological disorders); Inability to understand or complete the questionnaires accurately.
Sample size estimation
The sample size was calculated based on multiple regression analysis with seven predictor variables, including age, sex, disease duration, peer relationships, family relationships, parental educational level, and psychological resilience. According to Cohen’s (1988) guidelines for a medium effect size (f2 = 0.15), a significance level (α) of 0.05, and a statistical power of 0.80, the minimum sample size was estimated to be 92. To account for potential data loss or incomplete responses, an additional 10%–15% was added, resulting in a target sample size of 101–106 participants.
Data collection instruments
Data were collected using structured questionnaires administered to both patients and their parents or guardians. The questionnaires included the following components:
Demographic and clinical characteristics
A self-designed questionnaire was used to collect information on patient sex, age, disease duration, peer relationships, family relationships, and family income.
PTG
PTG was assessed using the Post-Traumatic Growth Inventory (PTGI), which consists of 21 items across 5 dimensions: Relating to Others, New Possibilities, Personal Strength, Spiritual Change, and Appreciation of Life. Each item was scored on a 6-point Likert scale (0 = “I did not experience this change” to 5 = “I experienced this change to a very great degree”), with total scores ranging from 0 to 105. The PTGI has demonstrated high reliability, with a Cronbach’s α of 0.90, and has been widely used in studies involving adolescents with PTG.9,14
Psychological resilience
Psychological resilience was measured using the Resilience Scale for Chinese Adolescents (RSCA), developed by Hu and Gan. This scale comprises 27 items rated on a 5-point Likert scale (1 = “strongly disagree” to 5 = “strongly agree”). It has shown good reliability and validity, with a Cronbach’s α ranging from 0.83 to 0.85 in a sample of 713 middle- and high-school students in China. 23
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data or median with interquartile range (IQR) for non-normally distributed data. Categorical variables were presented as frequencies and percentages. Student’s t-test or Mann–Whitney U test was used to analyze continuous data. Spearman correlation and linear regression analyses were performed to examine the relationships between PTG and resilience. Multiple regression analysis was conducted to identify predictive factors influencing PTG. The mediation effects of resilience were tested using the ‘median’ package in R software. Statistical significance was set at P < 0.05. Statistical analyses were performed using IBM SPSS Statistics software (version 26.0; IBM Corp., Armonk, NY, USA) and R programming language (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria).
Data collection procedure
Trained research nurses administered the questionnaires during outpatient visits or inpatient admissions. Participants completed the surveys privately, with clarification provided when necessary. Guardians independently provided socioeconomic and demographic data.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki (1975, as revised in 2024). The study protocol was approved by the Ethics Committee of Children’s Hospital of Soochow University (Approval number: 2024CS183). Written informed consent was obtained from all participants and their parents or guardians prior to participation. Confidentiality and anonymity of the data were maintained throughout the study.
Results
Participant characteristics
The final cohort comprised 104 cSLE patients, with a mean age of 13.46 ± 1.81 years. Female patients accounted for 66.35% (69/104) of the sample. Regarding disease duration, 48.08% of the participants had lived with SLE for more than 1 year. Most participants reported good peer relationships (58.65%) and positive family relationships (59.62%). Additionally, 53.85% of the families had a monthly income exceeding 10,000 Chinese Yuan (CNY). Detailed demographic and clinical characteristics of the study cohort are summarized in Table 1.
Clinical characteristics of the participants.
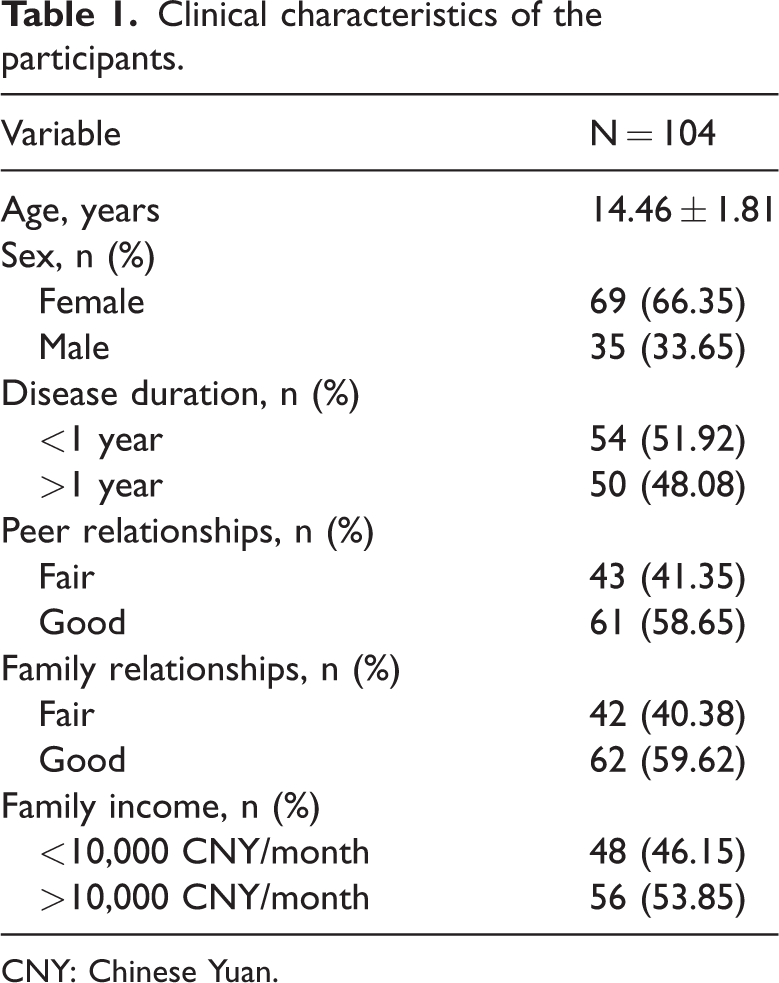
CNY: Chinese Yuan.
Scale reliability and score distributions
Both the PTGI and RSCA demonstrated excellent internal consistency, with Cronbach’s α coefficients of 0.917 and 0.859, respectively. Item analysis confirmed that no individual items would substantially improve the overall reliability if deleted, supporting the robust psychometric properties of both instruments. The mean and median PTGI scores were 63.41 ± 17.90 and 66.00 (IQR: 54.75–75.50), respectively. Among the PTGI subscales, “New Possibilities” showed the highest relative score (0.65 ± 0.22), followed by “Spiritual Change” (0.62 ± 0.24). The mean resilience score was 88.24 ± 15.06, with a median of 86.00 (IQR: 78.75–93.75). The distribution of scores for each item in the PTGI and resilience scales is illustrated in Figure S1 and summarized in Table 2.
Descriptive statistics for PTGI and resilience scales.

PTGI: Post-Traumatic Growth Inventory.
Correlation between PTG and resilience
Spearman correlation analysis demonstrated a statistically significant positive association between PTG and resilience (r = 0.504, 95% confidence interval (CI): 0.343–0.634, P < 0.001). The correlation coefficients between all clinical characteristics and PTG, including its subscale dimensions, are comprehensively presented in Table 3. This association between PTG and resilience was further validated through linear regression analysis (R2 = 0.254, adjusted R2 = 0.247, P < 0.001).
Correlation between patient characteristics, PTG, and resilience.

P < 0.05, bP < 0.01.
PTG: post-traumatic growth.
Multiple linear regression analysis of PTG
Multiple linear regression analysis identified several predictive factors of PTG (R2 = 0.337, adjusted R2 = 0.296, P < 0.001). Specifically, a disease duration of >1 year (β = 11.66 (95% CI: 5.57–17.75), P < 0.001), good family relationships (β = 10.59 (95% CI: 4.16–17.02), P = 0.002), and family income of >10,000 CNY/month (β = 3.11 (95% CI: 5.79–18.12), P < 0.001) were positively associated with PTGI scores. Detailed results are presented in Table 4.
Multiple linear regression analysis of PTGI scores.
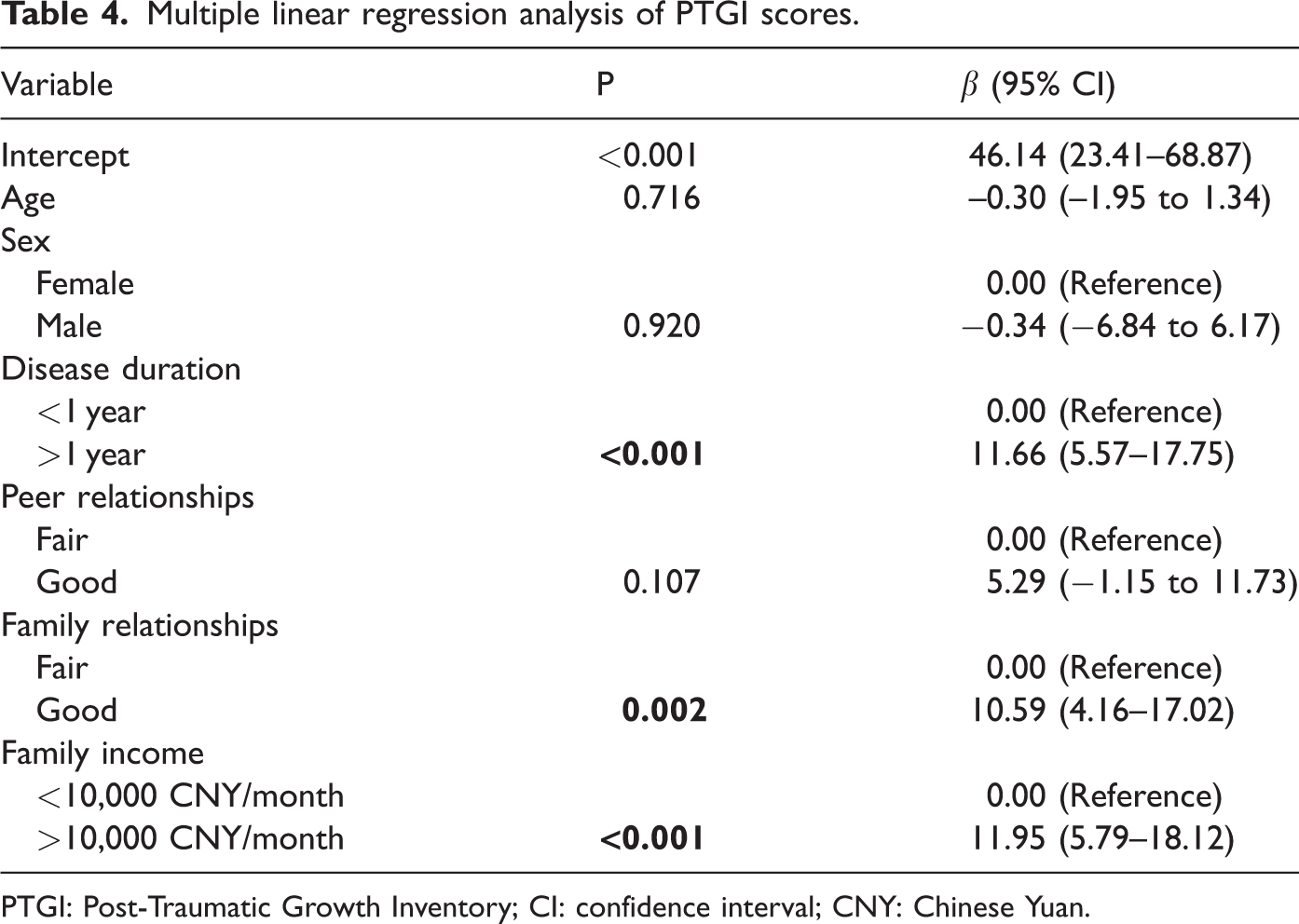
PTGI: Post-Traumatic Growth Inventory; CI: confidence interval; CNY: Chinese Yuan.
Mediating effect of resilience
Mediation analysis revealed that resilience partially mediated the relationship between disease duration and PTG, accounting for 22.09% of the total effect (P = 0.042) (Table 5). However, resilience did not demonstrate significant mediation effects for either family relationships (P = 0.370) or income level (P = 0.330).
Mediating effect of resilience on the relationship between patient characteristics and PTG.

PTG: post-traumatic growth; CI: confidence interval.
Group analysis of PTG scores
Subgroup analyses stratified by disease duration (<1 year (n = 54) vs. >1 year (n = 50)), family relationships (fair (n = 42) vs. good (n = 62)), and family income (<10,000 CNY/month (n = 48) vs. >10,000 CNY/month (n = 56)) revealed statistically significant differences in total PTGI scores across all comparisons (Figure 1). Specifically, PTGI scores were significantly higher among participants with longer disease duration (68.86 ± 16.08 vs. 58.37 ± 18.17, P = 0.0024), good family relationships (67.92 ± 16.10 vs. 56.76 ± 18.53, P = 0.0015), and higher family income (68.50 ± 15.34 vs. 57.48 ± 18.99, P = 0.0015). Analysis of PTGI subscales demonstrated significantly elevated scores (P < 0.05) in all dimensions for participants with >1 year disease duration, good family relationships, and >10,000 CNY/month family income relative to their respective counterparts, except for Spiritual Change and Appreciation of Life subscales between family relationship groups and the Personal Strength subscale across income strata (Table S1).

PTGI scores across different groups. (a) Disease duration. (b) Family relationships and (c) family income. *P < 0.05, **P < 0.01, *** P < 0.001. PTGI: Post-Traumatic Growth Inventory.
Discussion
This study represents the first comprehensive investigation of PTG and its psychological determinants in Chinese adolescents with cSLE. The findings challenge the prevailing deficit-focused narrative in pediatric rheumatology by demonstrating that PTG is not only achievable but also significantly influenced by resilience, familial support, socioeconomic stability, and disease chronicity. These results align with, but also extend, existing literature by highlighting unique cultural and disease-specific mediators of adaptation in a non-Western, resource-variable healthcare setting.
In this study, resilience demonstrated a positive correlation with PTG (R = 0.504, P < 0.001) and all five dimensions of PTG (Relating to Others (R = 0.466), New Possibilities (R = 0.437), Personal Strength (R = 0.444), Spiritual Change (R = 0.219), and Appreciation of Life (R = 0.497); all P < 0.05). These results suggest that resilience is a multifaceted construct that plays a crucial role in promoting PTG. One such mechanism is engagement in cognitive–emotional processing, which allows individuals to confront and integrate their traumatic experiences, thereby fostering growth. 24 Previous research indicated that resilience is more about emotional flexibility than maintaining a positivity bias. 25 This aligns with findings that emphasize the role of cognitive flexibility in enhancing PTG, as demonstrated in patients with severe sepsis, where resilience and cognitive flexibility were positively correlated with PTG levels. 26 The ability to engage with distress through effective coping strategies represents another pathway through which resilience promotes PTG. 27 Psychological flexibility and resilience were found to mediate the relationship between traumatic stress and PTG in a study conducted during the coronavirus disease 2019 (COVID-19) pandemic, highlighting the importance of adaptive coping in the face of adversity. 28 Furthermore, the role of resilience in promoting PTG is underscored by the finding that resilience can act as a buffer against post-traumatic stress, facilitating a focus on positive outcomes and appreciation for life. 29 Mediation analysis in the present study revealed that resilience partially explained the effect of disease duration on PTG (22.09%, P = 0.042), echoing findings in pediatric cancer but with distinct implications for SLE’s lifelong trajectory. 14 Unlike time-delimited traumas such as natural disasters, SLE’s cyclical nature may prolong the “cognitive–emotional wrestling” phase of PTG, wherein repeated stressor exposure paradoxically strengthens adaptation through iterative reappraisal.10,30 Notably, resilience did not mediate familial or socioeconomic effects (P > 0.05), suggesting that these factors operate via independent pathways.
The association between longer disease duration (>1 year) and higher PTG (β = 11.66, P < 0.001) highlights the role of time in the adaptation process. Living with cSLE necessitates continual adjustment, potentially fostering acceptance and the integration of illness into one’s identity, which are core to PTG.7,30,31 Adolescents in our cohort with longer disease duration reported higher scores in “New Possibilities” and “Personal Strength,” supporting the view of chronic illness as a potential “catalyst for maturity” during this formative life stage. 7 However, SLE’s unpredictability also poses challenges, as existential certainty is difficult to achieve. Patients with cSLE face a perpetual threat of disease flares, complicating the linear progression of PTG. 32 Clinicians should therefore frame PTG as a nonlinear, dynamic process rather than a fixed outcome.
Family relationships emerged as a strong predictor of PTG (β = 10.59, P = 0.002), reflecting the central role of familial support in collectivist cultures. Positive family dynamics likely buffer against illness-related stigma and isolation, providing a secure base from which adolescents can confront and make meaning of their condition.33,34 This aligns with the findings from studies on family communication patterns, which indicate that open and supportive communication can protect against depression and feelings of being unloved. 35 These findings underscore that strengthening family systems is not merely supportive but may be therapeutic, directly contributing to positive psychological outcomes and improved overall quality of life.
Socioeconomic status further modulated PTG, with higher income (>10,000 CNY/month) linked to greater growth (β = 3.11, P < 0.001). In China’s tiered healthcare system, financial security reduces barriers to biologics and outpatient care, mitigating allostatic load and freeing cognitive resources for adaptation. 36 However, cSLE may impose a significant financial burden on affected families, given the high rates of intensive care unit (ICU) admissions, multi-organ involvement, and prolonged hospitalizations observed in this population. 1 These findings highlight the need for policy interventions, such as expanded insurance coverage, to address socioeconomic disparities as a barrier to holistic patient care and psychological well-being.
The findings advocate for a paradigm shift in the management of cSLE toward proactively fostering PTG as a pathway to enhance quality of life. Clinically, this involves integrating resilience-building interventions, such as cognitive–behavioral therapy, and family-centered support into routine care. In parallel, policy efforts should address socioeconomic disparities by expanding insurance coverage for mental health services and biologics, thereby reducing financial toxicity and creating a more equitable foundation for psychological adaptation. For clinicians, the primary implication is that fostering PTG—through building resilience, leveraging family strengths, and alleviating socioeconomic stress—is a viable and essential strategy to improve the overall quality of life for adolescents navigating the challenges of cSLE. Viewing these patients with cSLE through a lens of growth potential, rather than solely through pathology, can transform clinical practice and patient outcomes. Future research should prioritize longitudinal designs to unravel the temporal dynamics of PTG in cSLE, capturing how growth trajectories fluctuate with disease activity, treatment phases, and developmental milestones. Mixed-methods approaches could elucidate the cultural nuances of PTG, such as the role of filial piety or collectivist values, which may differ markedly from Western contexts. Comparative studies across diverse healthcare systems would further clarify the interplay between socioeconomic policies and PTG outcomes. Finally, intervention trials are needed to evaluate the efficacy of resilience-promoting programs, both at individual and familial levels, in fostering sustainable growth.
Although this study provides novel insights into PTG among Chinese adolescents with cSLE, several limitations warrant consideration. First, the cross-sectional design precludes causal inferences regarding the relationships between resilience, familial support, and PTG. Longitudinal studies tracking patients from diagnosis through disease progression are essential to establish temporal precedence and disentangle the bidirectional influences of these factors. Second, reliance on self-reported measures may introduce response biases, such as social desirability or recall inaccuracies, particularly in assessments of sensitive constructs such as family relationships or spiritual change. Future studies could benefit from multi-informant approaches and objective biomarkers of stress adaptation to triangulate findings. Third, the single-center recruitment strategy may limit generalizability to broader populations. Nationwide, multicenter studies would enhance representativeness and capture regional variations in socioeconomic and cultural mediators. Finally, although our mediation analysis suggested that resilience partially explains the effect of disease duration on PTG, unmeasured confounders, such as genetic predispositions or prior trauma exposure, may influence these pathways. Advanced causal inference methods, including propensity score matching or instrumental variable analysis, could strengthen the robustness of these conclusions.
Despite these limitations, this study lays a foundation for redefining psychosocial care in cSLE, emphasizing the transformative potential of adversity when met with resilience, support, and systemic equity. By bridging gaps between developmental psychology, cultural medicine, and clinical rheumatology, these findings support a more holistic vision of healing—one that acknowledges not only the burdens of chronic illness but also the capacity for growth within vulnerable populations.
Conclusions
This study represents a pivotal step in understanding PTG among Chinese adolescents with cSLE, challenging the conventional narrative of psychopathology by illuminating pathways to positive psychological adaptation. The findings demonstrate that PTG is not only attainable in this population but is significantly shaped by psychological resilience, supportive family relationships, socioeconomic stability, and chronicity of disease experience. The strong correlation between resilience and PTG underscores the importance of fostering adaptive coping strategies, while the cultural emphasis on familial bonds highlights the need for family-centered interventions in collectivist societies. Moreover, the socioeconomic disparities observed call for policy-level changes to mitigate financial toxicity and ensure equitable access to care.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251392439 - Supplemental material for Post-traumatic growth and psychological resilience in adolescents with systemic lupus erythematosus: A cross-sectional study
Supplemental material, sj-pdf-1-imr-10.1177_03000605251392439 for Post-traumatic growth and psychological resilience in adolescents with systemic lupus erythematosus: A cross-sectional study by Lijuan Pu, Wei Zhao, Keyue Zhang, Tianma Huang, Yiyue Jin, Yulan Pan, Xiaozhong Li and Zhongqin Hong in Journal of International Medical Research
Footnotes
Acknowledgments
Not applicable.
Author contributions
Lijuan Pu performed data analysis and wrote the manuscript. Wei Zhao performed data analysis. Keyue Zhang performed data curation and validation. Tianma Huang provided resources. Yiyue Jin, Yulan Pan, and Xiaozhong Li supervised the project. Zhongqin Hong conceptualized the study. All authors have read and approved the final manuscript.
Data availability statement
All data used in this study are presented in this article. Further inquiries can be directed to the corresponding authors.
Declaration of conflicting interests
The authors report no conflicts of interest related to this work.
Institutional review board statement
The study protocol was approved by the Ethics Committee of the Children’s Hospital of Soochow University (Approval number: 2024CS183). Confidentiality and anonymity of the data were maintained throughout the study.
Informed consent statement
Written informed consent was obtained from all participants and their parents or guardians prior to participation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.