
Abstract
Objective
To determine the relative risk of atelectasis after abdominal surgery associated with perioperative fraction of inspired oxygen.
Methods
Our meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD 42021270703). The PubMed, Cochrane Library, EMBASE, and Web of Science databases were searched for randomized controlled trials reporting the influence of perioperative fraction of inspired oxygen on the incidence of postoperative atelectasis in patients who had undergone abdominal surgery under general anesthesia. We used a random-effect model to calculate the relative risk of postoperative atelectasis. Subgroup analyses were performed according to age, ventilation strategy, surgical incision site, and surgery duration.
Results
Finally, we included 10 randomized controlled trials involving 3471 participants. Compared with the high fraction of inspired oxygen group (60%–100%), a reduced atelectasis incidence after abdominal surgery was observed in the low fraction of inspired oxygen group (20%–40%). Patients with an average age ≥60 years benefited more from a low fraction of inspired oxygen in terms of prevention of postoperative atelectasis compared with those with an average age <60 years (risk ratio: 1.47; 95% confidence interval: 1.14–1.90). Patients undergoing lower abdominal surgery benefited from a low perioperative fraction of inspired oxygen (risk ratio: 1.43; 95% confidence interval: 1.14–1.80).
Conclusions
A low perioperative fraction of inspired oxygen may decrease the risk of atelectasis after lower abdominal surgery performed under general anesthesia, especially in patients with an average age <60 years.
Introduction
Atelectasis is a postoperative complication observed in the majority of patients who undergo surgery under general anesthesia (GA) and can persist for several months.1–4 Surgical manipulations, especially during abdominal surgery, can move the diaphragm cranially and decrease pulmonary compliance, resulting in a high incidence of postoperative atelectasis.5–8 Three mechanisms may contribute to atelectasis development: gas absorption, lung tissue compression, and surfactant deficiency. 2 Moreover, atelectasis is considered the leading cause of several postoperative complications, such as pneumonia and hypoxemia, which hamper patients’ recovery.2,3
Various modalities have been proposed to ensure patient safety; among these, a high perioperative fraction of inspired oxygen (FiO2) is considered a promising option.2,9–14 A high-pitched beep of an oxygen saturation detector and elevated levels of oxygen saturation are desirable for clinicians. However, the existing high-quality evidence on the association between FiO2 and postoperative atelectasis is inconsistent.15–18 It remains debatable among clinicians whether a high perioperative FiO2 helps prevent postoperative atelectasis in patients who have undergone abdominal surgery. A set of international expert panel-based consensus recommendations on practical measures to prevent postoperative pulmonary complications was issued in 2019, which recommends a perioperative FiO2 ≤40%. 19 In 2020, Li et al. found that compared with a high perioperative FiO2, a low perioperative FiO2 was not associated with a lower incidence of postoperative atelectasis in patients who had undergone abdominal surgery under GA. 15 This contrasts the study results reported by Wei et al. who concluded that a high perioperative FiO2 induced postoperative atelectasis in patients who had undergone abdominal surgery under GA. 20 A high perioperative FiO2 could be considered acceptable because it improves the safety margin in the event of hypoxia and prolonged apnea. 16 However, a high perioperative FiO2 reportedly causes atelectasis due to gas absorption.2,9,21
Therefore, a comprehensive evaluation of the existing evidence regarding the association between perioperative FiO2 and postoperative atelectasis in patients who have undergone abdominal surgery is urgently needed. We aimed to extract data from randomized controlled trials (RCTs) regarding postoperative atelectasis in patients who had undergone abdominal surgery under GA to compare the effect of high versus low perioperative FiO2 and provide evidence that can guide clinical practice.
Methods
This meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD 42021270703). We conducted this systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 22 The PRISMA checklist is presented in Table S1.
Search strategies
The PubMed, Cochrane Library, EMBASE, and Web of Science databases were comprehensively searched for RCTs published before September 2025 that had investigated the influence of perioperative FiO2 on the incidence of atelectasis after abdominal surgery. In addition, the bibliographies of all included studies were checked for any potential additional publications of interest. Searches were rerun immediately before the final analysis to identify any additional studies that meet the inclusion criteria. The detailed search strategies for each database are presented in Table S2.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (a) RCTs; (b) studies investigating the influence of perioperative FiO2 on the incidence of atelectasis after abdominal surgery; (c) surgeries were performed among adults (aged ≥18 years); and (d) full text of the article was available. A perioperative FiO2 ≥50% was considered high and perioperative FiO2 <50% low.
Studies were excluded if they were duplicate publications, reviews, editorials, abstracts, comments, case reports, meetings, or animal experiments. We also excluded studies wherein patients had undergone surgery under local anesthesia, had only received oxygen postoperatively or for a short duration intraoperatively, or had received supplemental oxygen during their stay in the intensive care unit.
Data extraction
Two reviewers (Z.W. and M.J.) independently screened the articles based on their titles and abstracts, according to our eligibility criteria; they also evaluated the risk of bias in the included studies using Cochrane Collaboration’s tool for assessing the risk of bias in RCTs. They extracted data from the included studies following a prespecified protocol; any disagreements were resolved via consultation. The original data included characteristics of the included studies (first author, country, publication year, sample size, and patient age), intervention strategies, and outcomes (incidence of postoperative atelectasis and severity of postoperative atelectasis). We used a widely accepted formula to estimate the mean and SD values using the data described in the form of median (interquartile range) values. 23 The severity of postoperative atelectasis was evaluated using Wilcox severity scoring and lung ultrasound scoring system.24,25
Data synthesis
Data were analyzed using Review Manager (RevMan, version 5.4, Copenhagen, Nordic Cochrane Centre, the Cochrane Collaboration, 2014). Dichotomous variables were expressed as risk ratios (RRs) and 95% confidence intervals (CIs), while continuous variables were described as mean differences and 95% CIs. Cochran’s Q test and Higgins’ I2 statistical test were used to assess the statistical heterogeneity of the pooled results. If 0% ≤ I2 < 25%, the results showed no heterogeneity; if 25% ≤ I2 < 50%, the results showed a low level of heterogeneity; if 50% ≤ I2 < 75%, the results showed a medium level of heterogeneity; and if 75% ≤ I2 ≤ 100%, the results showed a high level of heterogeneity. Subgroup analyses were performed based on risk factors that might contribute to postoperative atelectasis (ventilation strategy, oxygen administration strategy, age, surgery duration, and surgical incision site). In addition, a sensitivity analysis was performed to detect the sources of heterogeneity by excluding specific studies.
Results
Study selection
We identified 1676 studies; of these, 618 were duplicates, and 1029 were excluded based on their titles and abstracts. Thus, 29 full-text articles were further screened, of which 9 were excluded due to lack of outcomes and 12 were excluded for reporting on patients who had undergone non-abdominal surgery. Finally, 10 studies15,16,20,26–32 that met the inclusion criteria were included (Figure 1). The characteristics of the included studies are presented in Table 1.

PRISMA flow diagram. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of the included studies.

PEEP: positive end-expiratory pressure; IVA: intravenous anesthesia; IA: inhalational anesthesia; FiO2: fraction of inspired oxygen; POD: postoperative day; CT: computed tomography; PACU: post-anesthesia care unit.
Study quality and risk of bias
The risk of bias assessment is presented Figures 2 and S1. A high risk of performance bias was observed in four studies16,27,28,30 because the anesthesiologists in these studies were not blinded to the trials; they were aware of the FiO2 target for each participant and made proper adjustments to achieve the target FiO2 levels. Three studies did not report whether the anesthesiologists assigned to perioperative management and the patients were aware of group assignment;26,29,31; thus, these studies were rated as having an “unclear risk” of performance bias. The anesthesiologists in the other three studies were also not blinded to the trials; however, they were not involved in the studies.15,20,32 Therefore, they were recorded as having a low risk of performance bias.
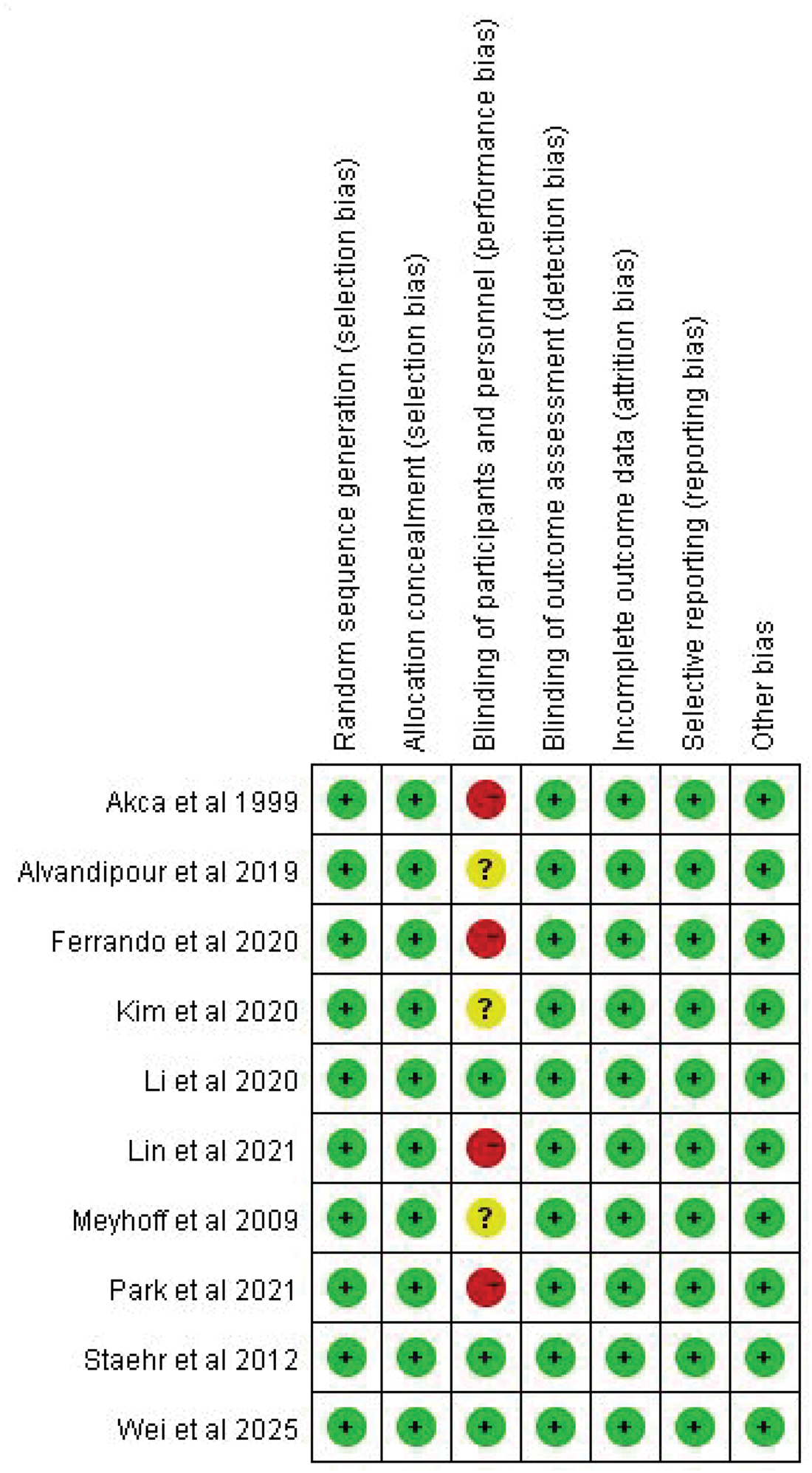
Risk of bias summary. Green, yellow, and red represent low risk of bias, unclear bias, and high risk of bias, respectively.
Outcome
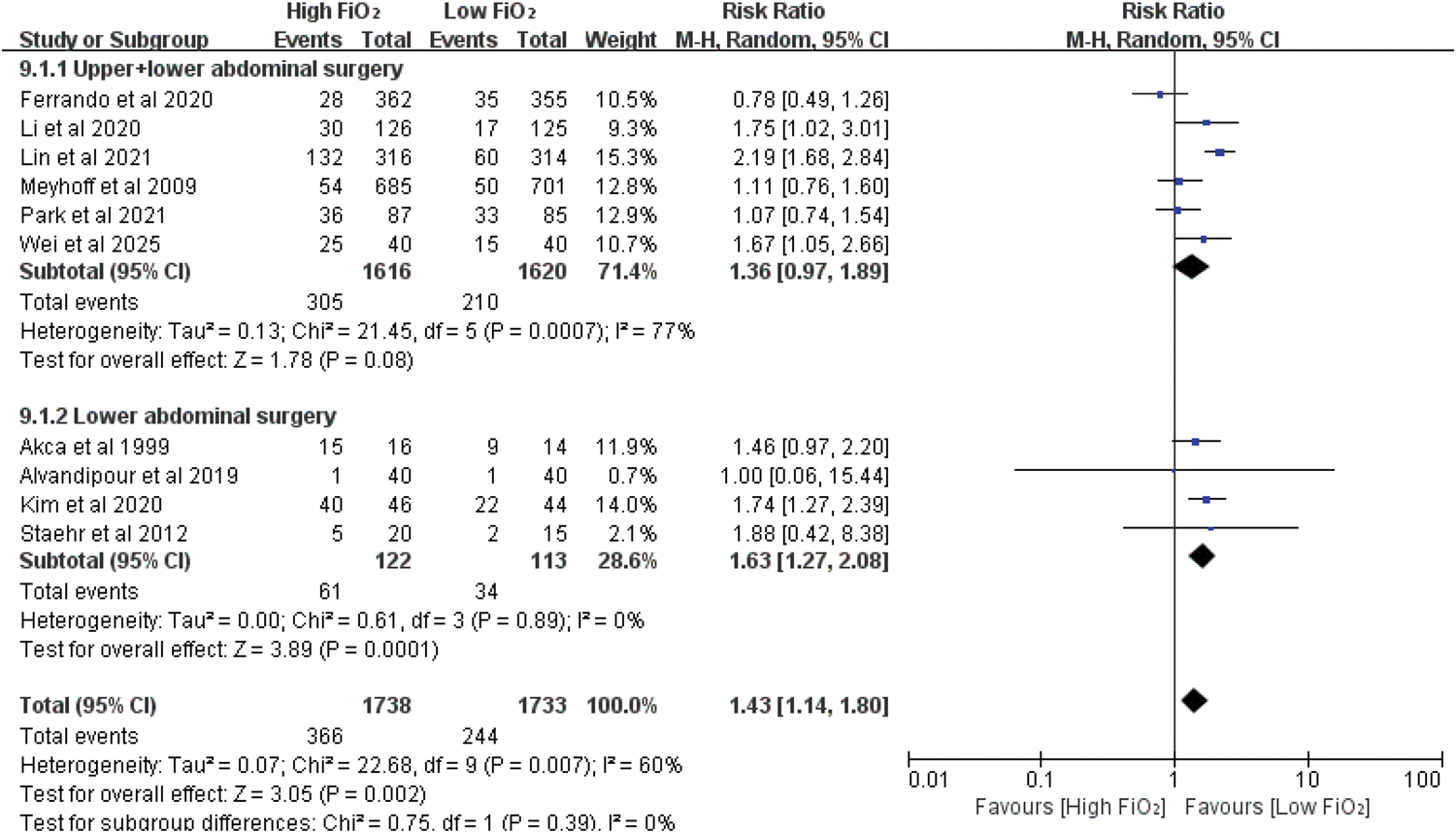
All 10 studies15,16,20,26–32 reported the incidence of postoperative atelectasis in patients who had undergone abdominal surgery under GA. The pooled results of the meta-analysis indicated that compared with a high perioperative FiO2 (60%–100%), a low perioperative FiO2 (≤40%) was associated with a significantly reduced incidence of atelectasis after abdominal surgery (RR: 1.43; 95% CI: 1.14–1.80; p = 0.002), with moderate heterogeneity (I2 = 60%, p = 0.007) (Figure 3).

Forest plot of the association between perioperative fraction of inspired oxygen and incidence of postoperative atelectasis.
Subgroup analyses
The use of positive end-expiratory pressure (PEEP) was reported in six studies.15,16,20,29,30,32 Patients in both high and low FiO2 groups did not benefit from intraoperative PEEP application in terms of prevention of atelectasis after abdominal surgery (RR: 1.35; 95% CI: 1.01–1.82; p = 0.04), with moderate heterogeneity (I2 = 56%, p = 0.04). The beneficial effect of a low perioperative FiO2 in preventing atelectasis after abdominal surgery was statistically significant when PEEP was not applied intraoperatively (RR: 1.54; 95% CI: 1.03–2.30; p = 0.01), with moderate heterogeneity (I2 = 68%, p = 0.02) (Figure 4).

Subgroup analysis based on the application of positive end-expiratory pressure.
Four studies involved patients with an average age of ≥60 years,16,20,28,30 other four studies involved patients with an average age <60 years,15,27,29,31 and the rest two were awaiting further classification because they involved patients aged 58–64 years.26,32 The incidence of postoperative atelectasis was significantly reduced by a low perioperative FiO2 in the subgroup of participants aged <60 years (RR: 1.64; 95% CI: 1.31–2.06; p < 0.0001), with no heterogeneity (I2 = 0%, p = 0.88). No significant difference was found in the subgroup of patients aged ≥60 years (RR: 1.35; 95% CI: 0.84–2.16; p = 0.22), with high heterogeneity (I2 = 84%, p = 0.0003) (Figure 5).

Subgroup analysis by age.
Oxygen was administered both intraoperatively and postoperatively in five studies,26,27,30–32 while the other five studies only exposed patients to oxygen during the surgery.15,16,20,28,29 As depicted in Figure 6, patients in the low FiO2 group had a lower incidence of atelectasis after surgery when oxygen was only administered intraoperatively (RR: 1.66; 95% CI: 1.28–2.15; p = 0.0002), with moderate heterogeneity (I2 = 60%, p = 0.04). No significant difference was observed between the high and low FiO2 groups when oxygen was administered both intraoperatively and postoperatively (RR: 1.12; 95% CI: 0.86–1.47; p = 0.39), with low heterogeneity (I2 = 14%, p = 0.32) (Figure 6).

Subgroup analysis by oxygen administration strategies.
Four studies reported that patients who had undergone lower abdominal surgery benefited more from a low perioperative FiO2 in terms of prevention of postoperative atelectasis (RR: 1.63; 95% CI: 1.27–2.08; p = 0.0001), with no heterogeneity (I2 = 0%, p = 0.89)].27,29,31,32 Six studies involved both patients undergoing upper abdominal surgery and lower abdominal surgery, and the incidence of postoperative atelectasis was comparable between the high and low FiO2 groups (RR: 1.36; 95% CI: 0.97–1.89; p = 0.08), with high heterogeneity (I2 = 77%, p = 0.0007)] (Figure 7).15,16,20,26,28,29
Subgroup analysis by surgical incision site.
Three studies reported a mean surgery duration of ≥3 h,15,28,30 while a shorter mean surgery duration (<3 h) was observed in other three studies.20,26,29 No significant difference was observed between the high FiO2 and low FiO2 groups in terms of postoperative atelectasis incidence (RR: 1.47; 95% CI: 0.78–2.77; p = 0.24) (Figure 8).

Subgroup analysis by surgery duration.
Severity of postoperative atelectasis
Five studies reported the severity of postoperative atelectasis.16,20,27,29,32 However, owing to the inconsistent data format and a small sample size, we could not identify any clear data trends or detect important differences in the severity of postoperative atelectasis between the high and low FiO2 groups.
Sensitivity analysis
The heterogeneity significantly decreased after excluding the studies by Lin et al. and Meyhoff et al. because both these studies involved patients undergoing emergency surgery, a risk factor for postoperative pulmonary complications (I2 = 40%, p = 0.11) (Figure S2).33,34
Discussion
Our meta-analysis of 10 RCTs suggested that a low perioperative FiO2 (≤40%) significantly reduced the incidence of postoperative atelectasis in patients who had undergone abdominal surgery under GA, especially those aged <60 years and those undergoing lower abdominal surgery. PEEP did not help prevent atelectasis after abdominal surgery in either the high FiO2 (60%–100%) or low FiO2 (≤40%) group.
Three meta-analyses have reported the influence of different perioperative FiO2 levels on postoperative pulmonary function.17,18,35 However, they focused on patients undergoing different types of surgery; hence, the findings lacked specificity. In contrast, the conclusions about atelectasis were derived from results with high heterogeneity and very low-quality evidence, making them incapable of illustrating the influence of perioperative oxygen on atelectasis incidence.
To the best of our knowledge, this is the first systematic review and meta-analysis that focused on the influence of perioperative FiO2 on postoperative atelectasis incidence in patients undergoing abdominal surgery under GA. Moreover, the comprehensive subgroup analyses according to the risk factors for pulmonary complications after abdominal surgery and sensitivity analyses can help evaluate the robustness of our results.
Our study suggested that a low perioperative FiO2 (≤40%) is beneficial for preventing atelectasis after abdominal surgery. During clinical practice, concerns regarding the occurrence of hypoxemic events may prompt greater intraoperative oxygen administration. Moreover, a set of guidelines issued by World Health Organization in 2016 has recommended the maintenance of a high perioperative FiO2 (80%) to improve patient prognosis. 36 Thus, we should weigh the advantages and disadvantages of high versus low perioperative FiO2 levels.
Aging is strongly associated with a higher incidence of postoperative pulmonary complications.7,8 The present study showed that patients with an average age ≥60 years did not exhibit the beneficial effects of perioperative low FiO2 (≤40%) in terms of prevention of atelectasis after abdominal surgery. Age reflects the functional capacity of the body, and postoperative atelectasis results from target organ dysfunctions and poor physical condition of the patient.7,37 Therefore, further studies should focus on preventing postoperative atelectasis in patients aged >60 years.
The beneficial effects of lung-protective ventilation strategies, including PEEP, have been widely accepted by clinicians.38–40 However, the ideal level of PEEP during surgery has not yet been established. Our data showed that intraoperative PEEP application may reduce the beneficial effects of a low perioperative FiO2 in preventing atelectasis after abdominal surgery, based on a result with moderate heterogeneity. Thus, further investigations on the ideal level of PEEP and an optimal perioperative FiO2 level for prevention of postoperative atelectasis are urgently needed.
Filling the lungs with oxygen appears convincing, considering the difficulty in breathing and subsequent hypoxemia experienced after waking up. Our study suggested that only a low intraoperative FiO2 was beneficial for preventing atelectasis after abdominal surgery. However, current evidence regarding the influence of post-oxygenation on postoperative atelectasis includes several confounders, such as the presence of lung-protective ventilation and lack of blank controls.41–43 Therefore, the influence of post-oxygenation on postoperative atelectasis should be independently assessed in future studies.
Patients with lower abdominal surgical incision may experience a reduced incidence of postoperative atelectasis compared with those with an upper abdominal incision. 8 In our study, patients with lower abdominal incision benefited from perioperative low FiO2 (≤40%) in reducing the incidence of postoperative atelectasis. The upper abdominal incision is closer to the diaphragm than the lower abdominal incision; therefore, surgeries involving upper abdominal incision are more likely to cause cranial displacement of the diaphragm, and more remarkably, affect pulmonary function, resulting in a higher incidence of postoperative atelectasis.5–8
To evaluate the influence of individual studies on the overall effect and identify the sources of heterogeneity, we performed a sensitivity analysis by excluding specific studies. After excluding a study involving patients undergoing emergency surgery, the heterogeneity decreased considerably (I2 = 41%). 28 Notably, emergency surgery is a risk factor for postoperative pulmonary complications.33,34
Certain limitations of our study should be acknowledged. First, the incidence of postoperative pulmonary complications gradually increased with prolonged surgery duration. The odds ratio may rise up to 9.7 (4.7–19.9) when the surgery lasts for >3 h.7,8 However, the subgroup analysis by surgery duration in our study had a small sample size with high heterogeneity. Thus, further studies should focus on the association between surgery duration and the beneficial effects of perioperative low FiO2 (≤40%) for the prevention of atelectasis after abdominal surgery. Second, the definitions of postoperative atelectasis varied among the included studies. Data were captured at different time points after surgery, which may be another factor contributing to the moderate heterogeneity.
Conclusions
Moderate-quality evidence from the present meta-analysis suggests that a low perioperative FiO2 decreases the risk of postoperative atelectasis in patients undergoing lower abdominal surgery under GA, especially those with an average age <60 years.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251392431 - Supplemental material for A low perioperative fraction of inspired oxygen reduces the incidence of postoperative atelectasis in patients undergoing abdominal surgery under general anesthesia: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605251392431 for A low perioperative fraction of inspired oxygen reduces the incidence of postoperative atelectasis in patients undergoing abdominal surgery under general anesthesia: A systematic review and meta-analysis by Zuofeng Wang, Min Jiang, Cuiyuan Huang, Hengjing Zou, Yu Wen and Shan Ou in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605251392431 - Supplemental material for A low perioperative fraction of inspired oxygen reduces the incidence of postoperative atelectasis in patients undergoing abdominal surgery under general anesthesia: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605251392431 for A low perioperative fraction of inspired oxygen reduces the incidence of postoperative atelectasis in patients undergoing abdominal surgery under general anesthesia: A systematic review and meta-analysis by Zuofeng Wang, Min Jiang, Cuiyuan Huang, Hengjing Zou, Yu Wen and Shan Ou in Journal of International Medical Research
Footnotes
Acknowledgements
This study would not have been possible without the collaboration of all colleagues in our team.
Authors’ contributions
Z.W. and S.O. designed this study. Z.W. and C.H. searched all the databases independently and screened the articles based on their titles and abstracts according to our eligibility criteria. Y.W. and H.Z. performed data analyses. Z.W. prepared the manuscript. S.O. supervised all study processes and revised the manuscript. All authors have read and approved the final manuscript.
Data availability statement
All data are available upon request to the corresponding authors.
Declaration of competing interest
We declare that there is no conflict of interest regarding this study.
Funding
This study did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.