
Abstract
Carotid web, a special vascular lesion, has been increasingly recognized as a significant etiology of ischemic stroke. Unlike traditional atherosclerosis, carotid web is a linear intraluminal protrusion with a free edge that oscillates with blood flow, leading to blood flow stagnation and thrombus formation. These pathophysiological features lead to the high risk of stroke recurrence and certain association with large-vessel occlusion. Given these, carotid artery revascularization has been recommended as an optional treatment for carotid web. We herein described a case of a patient with ischemic stroke and carotid web who eventually underwent carotid artery stenting after recurrent ischemic attacks during hospitalization. However, the patient developed status epilepticus postoperatively. Repeated magnetic resonance imaging revealed an enlarged infarction, whose location was consistent with the territory of the anterior cerebral artery. Regarding therapy, intravenous infusion of sodium valproate successfully terminated the status epilepticus secondary to stroke, providing an alternative when clinicians are concerned about the depression of diazepam. Subsequent oral antiseizure medications were required and newer-generation agents (e.g. levetiracetam, lacosamide, zonisamide, and topiramate) were increasingly recommended due to their neutral impact on secondary stroke prevention.
Background
Carotid web, an atypical intimal variant of fibromuscular dysplasia, is characterized by a fibrolamellar intimal flap protruding from the posterior wall of the internal carotid bulb into the arterial lumen. 1 Compared with traditional atherosclerosis, this distinct anatomical feature induces more pronounced alterations in local hemodynamics, leading to blood flow stagnation, thrombus formation, and subsequent ischemic events such as transient ischemic attacks (TIA) and ischemic stroke. 2 Currently, antiplatelet therapy remains the first-line treatment for stroke associated with carotid web. 3 However, medication therapy alone is associated with a high rate of stroke recurrence, ranging from 27% to 56% within 5 years.4–6 Therefore, carotid artery revascularization could be considered for patients experiencing multiple ischemic events associated with carotid web. 3
We herein reported a case of a patient with ischemic stroke and carotid web who experienced recurrent ischemic attacks after receiving dual antiplatelet therapy and argatroban anticoagulation. Following these recurrent events, the patient underwent carotid artery stenting (CAS). However, the patient developed status epilepticus postoperatively. By reviewing this case, we aimed to explore the potential causes of postoperative status epilepticus and concluded therapeutic recommendations in similar contexts.
Case presentation
A man in his early 70s presented with left lower limb weakness persisting for over 1 day and was admitted to the Seventh People’s Hospital of Chongqing in February 2025. At admission, he had grade III left lower limb muscle strength with a National Institute of Health Stroke Scale (NIHSS) score of 2. Immediate brain magnetic resonance imaging (MRI) revealed right frontal subcortical infarction (Figure 1(a)). Based on the admission NIHSS score of 2, dual antiplatelet therapy (aspirin (100 mg qd) and clopidogrel (75 mg qd)) was applied. On the fourth day of hospitalization, the patient experienced a decline in left lower limb muscle strength to grade II, with the NIHSS score increasing to 4, indicating early neurological deterioration. Argatroban was applied to prevent further deterioration, resulting in subsequent improvement of muscle strength to grade IV.7,8

Brain magnetic resonance imaging (MRI) findings. This first brain MRI was performed immediately at admission, and the diffusion weighted image (DWI) showed right frontal subcortical infarction (a). The second brain MRI was performed after the occurrence of status epilepticus, and the DWI revealed enlargement of the infarction (b).
On the sixth day of hospitalization, digital subtraction angiography (DSA) was performed, revealing a carotid web at the origin of the right internal carotid artery (Figure 2(a)). As DSA was recognized as the gold standard imaging modality for cerebrovascular disease, supplementary assessments such as ultrasound or magnetic resonance angiography were not performed. However, on the next day, the patient experienced transient left lower limb weakness during ambulation. Given the recurrent ischemic attacks despite dual antiplatelet therapy and argatroban anticoagulation during hospitalization, further carotid artery revascularization was considered. Therefore, CAS was performed on the 13th day of hospitalization after obtaining written informed consent from the patient and his family for the procedure. During the CAS procedure, a Spider FX Embolic Protection Device (SPD2-050-320; Nathan Lane North in Plymouth, Massachusetts, United States) was deployed at the distal end of the C1 segment of the right internal carotid artery. After measuring the arterial diameter, a self-expanding stent (EV3 Protégé stent; SEPX-8-6-40-135) was selected and deployed to fully cover the carotid web. Post-stent angiography confirmed complete resolution of the carotid web (Figure 2(b)). The whole system was subsequently withdrawn, and the protection device was inspected, revealing no captured thrombus. Given the optimal angiographic result, further postdilatation was not performed. Heparin anticoagulation was administered postprocedurally to prevent stent thrombosis after CAS (4000 IU q12h, lasting for 3 days).
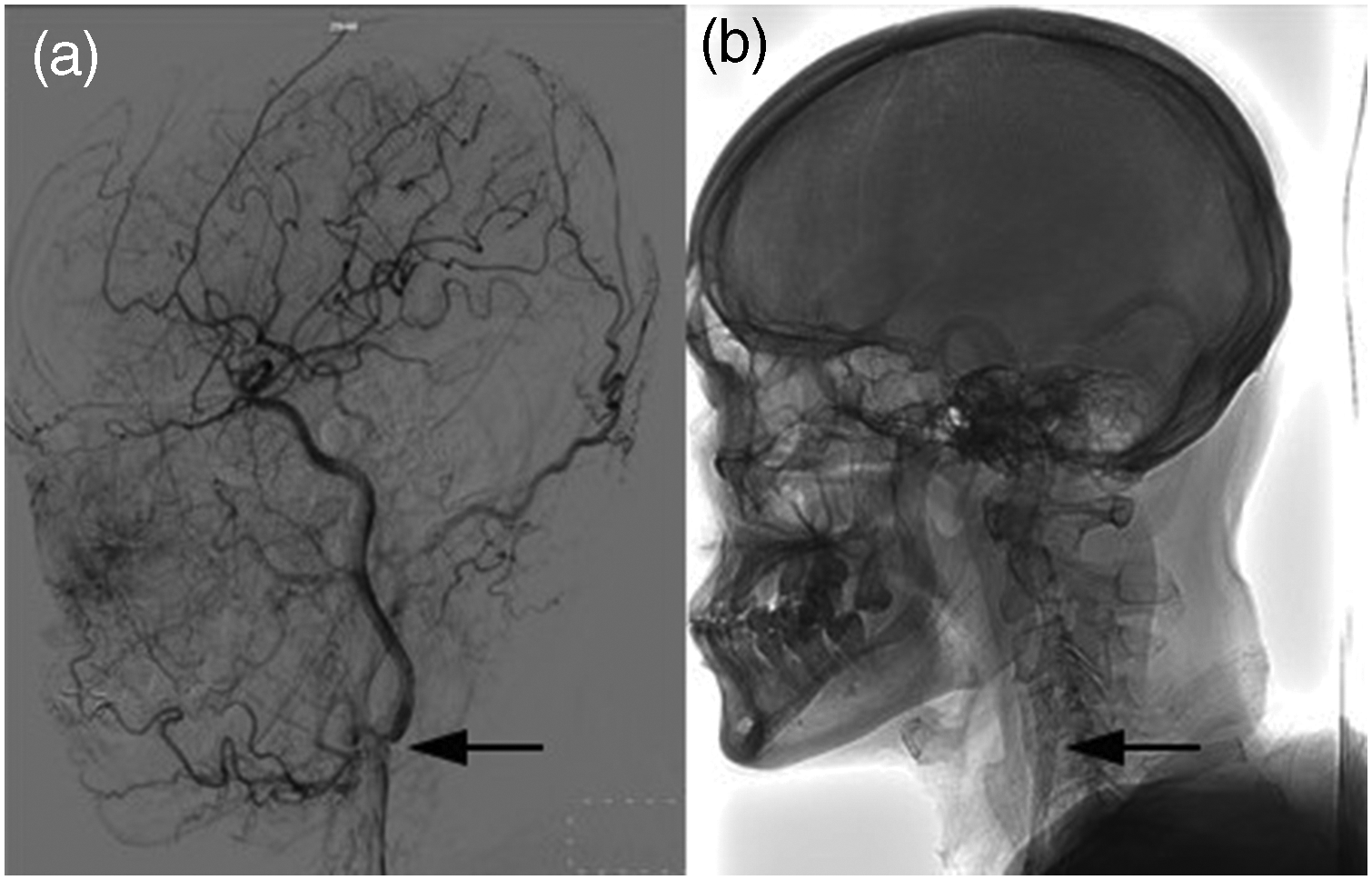
Digital subtraction angiography findings. Defects and residual contrast media were observed at the origin of the internal carotid artery, suggestive of carotid web (a). Carotid artery stenting was performed, and the carotid web disappeared subsequently (b).
Postoperatively, the patient experienced stiffness in the left lower limb for >10 min. Hence, it could not be bent, although it could still be lifted off the bed. According to the recommendation from the International League against Epilepsy, this condition was recognized as status epilepticus (tonic status). 9 Furthermore, 10 mg of diazepam (DZP) was administered to terminate this abnormal status. However, due to subsequent deterioration in consciousness (from awake to excessively sleepy) and oxygenation (oxygen saturation from 99% to <90%), DZP administration was discontinued, leading to the recovery of the abovementioned conditions. Given its lower risk of respiratory depression, intravenous infusion of sodium valproate (SV) was applied (20 mg/kg injection followed by 20 mg/kg/d infusion). 10 Following these interventions, the stiffness in the patient’s left lower limb resolved. However, its muscle strength declined to grade 0 and persisted for over 48 h without improvement. Therefore, repeated brain MRI was conducted, revealing an enlarged infarction, inconsistent with Todd’s paralysis, TIA, or reperfusion injury. Additionally, the infarct location was consistent with the territory of the anterior cerebral artery (Figure 1(b)). On the 16th day of hospitalization, intravenous SV infusion was discontinued and transitioned to oral administration of levetiracetam (0.5 g q12h) and SV (0.5 g q12h). Following rehabilitation therapy, his muscle strength improved to grade III at discharge. At the 3-month follow-up, he exhibited further neurological recovery, with left lower limb strength improving to grade IV and achieving a modified Rankin Scale (mRS) score of 1. No recurrent ischemic events or seizures were observed during this period. The presentation of this case conformed to the Case Report (CARE) guidelines. 11
Discussion
Perioperative seizures were not rare among patients undergoing CAS or carotid artery revascularization. A prospective multicenter study conducted across 14 hospitals reported that 16 patients (2.1%) developed seizures after CAS. 12 Similarly, another study reported 5 cases (0.6%) of seizures among 841 patients who underwent carotid endarterectomy (CEA). 13 In addition, several cases of perioperative seizures have been reported to date.14–17
However, for carotid web specifically, a low incidence of perioperative complications has been reported. A 2022 meta-analysis including 15 studies reported that 151 patients with symptomatic carotid web underwent carotid artery revascularization, and there was no significant intraoperative or postoperative mortality, ischemic or hemorrhagic stroke, in-stent thrombosis, or restenosis. During follow-up, only one patient who underwent CAS exhibited asymptomatic proximal stent stenosis, and another experienced an external iliac artery rupture. However, the authors also emphasized that the findings of this meta-analysis may be influenced by the limited sample size and potential publication bias. 5 In this study, we reported a rare case of status epilepticus occurring in a stroke patient with carotid web after CAS.
We summarized the potential reasons for perioperative seizure activity from the existing studies. First, cerebral hyperperfusion syndrome (CHS) is considered a common cause of seizures after carotid artery revascularization, which may be related to increased cerebral blood flow, impaired cerebral self-regulation, and baroreceptor dysfunction during surgery. Risk factors included decreased cerebrovascular reactivity, severe stenosis of the contralateral vessel, postoperative hypertension, and recent ipsilateral stroke.18,19 In addition, contrast-induced encephalopathy (CIE) is a potential cause of seizures after carotid artery revascularization, which may be related to the destruction of the blood–brain barrier. Zhu et al. 20 reported the case of a patient who developed seizures after CAS. Brain MRI indicated cerebral edema and meningitis, primarily considered as CIE. Subsequent antibody testing revealed positivity for anti–neurotoxin-3α antibodies. The authors hypothesized that the disruption of the blood–brain barrier caused by CIE allowed anti–neurotoxin-3α antibodies to migrate from the serum into the cerebrospinal fluid, resulting in autoimmune encephalitis and secondary seizures.
In our case, we inferred that the postoperative status epilepticus resulted from a new-onset anterior cerebral artery occlusion secondary to the carotid web. Comparing the infarction on both brain MRI scans, we found that the infarction had expanded, and its location was consistent with the territory of the anterior cerebral artery. As previously mentioned, symptomatic carotid web was associated with a high rate of stroke recurrence. Moreover, it could lead to large-vessel occlusion and was identified at the carotid bifurcation in approximately 2.5% cases of acute ischemic stroke caused by large-vessel occlusion. 21 Among stroke patients with large-vessel occlusion, those with carotid web had a significantly higher risk of recurrent stroke at 2 years compared with those without carotid web (17% vs. 3%). 22 The high risk of stroke recurrence and large-vessel occlusion associated with carotid web may be attributed to its unique anatomical characteristics. As mentioned previously, the carotid web presents as a linear protrusion into the arterial lumen with a free edge oscillating with blood flow. 1 This unique anatomical structure leads to blood flow stagnation, thrombus formation, ischemic events, and even large-vessel occlusion.2,21,22 However, stent thrombosis was excluded due to the dual antiplatelet therapy before CAS and heparin anticoagulation after CAS. Post-stent angiography confirmed the resolution of carotid web, and no thrombus was detected on the protection device. Thus, we inferred that the pre-existing thrombus immigrated to the right anterior cerebral artery, resulting in new-onset infarction. In conclusion, the unique anatomical and hemodynamic characteristics of carotid web eventually led to the new-onset cerebrovascular disease along with status epilepticus in our case.
Cerebrovascular disease is a common cause of seizure activity, accounting for approximately 50% of new-onset seizures in the older population. Additionally, 2%–14% of patients with ischemic stroke may develop post-stroke epilepsy.23,24 Based on the temporal relationship, seizures occurring within 7 days after stroke are generally classified as early-onset seizures or acute symptomatic seizures, for which active antiseizure treatment is not typically recommended. Seizures occurring more than 7 days after stroke are classified as late-onset seizures, which is the definition of post-stroke epilepsy by the International League against Epilepsy, and formal antiseizure treatment is recommended. For status epilepticus, immediate antiseizure treatment is required, and DZP remains the first-line recommendation.25,26 However, the patient in our case experienced deterioration in consciousness and oxygenation following DZP administration, which was eventually replaced with intravenous SV infusion. This suggested that when clinicians are concerned about the excessive depression of DZP, intravenous SV infusion could be an alternative for terminating the status epilepticus secondary to stroke. Notably, Özdemir et al. 27 reported that among 19 patients treated with intravenous SV after diazepam administration, the status epilepticus secondary to stroke could be successfully terminated in 12 patients. Therefore, DZP–SV sequential therapy may represent a viable alternative in this context, although further investigation is required to validate its efficacy.
Subsequently, oral antiseizure medications were needed even when the abnormal status was terminated, 28 and newer-generation agents (e.g. levetiracetam, lamotrigine, lacosamide, zonisamide, perampanel, gabapentin, and topiramate) were increasingly recommended. 29 Enzyme-inducing antiseizure medications, such as carbamazepine, phenobarbital, and phenytoin, should be avoided due to the risk of increasing blood lipid levels and disadvantage in secondary stroke prevention. 30 Notably, statins have potential efficacy in reducing the incidence of post-stroke epilepsy. Moreover, intensive statin therapy (atorvastatin (40 mg qd) or rosuvastatin (20 mg qd)) was more effective than standard doses. 31 Potential mechanisms included anti-inflammatory actions on the vascular endothelium, inhibition of free radical generation, activation of gamma-aminobutyric acid (GABA)-ergic activity, and stabilization of cell membranes. 32 However, these findings remain to be confirmed through high-quality randomized controlled trials.
Conclusion
Carotid web represents a distinct etiology of ischemic stroke, characterized by a high risk of stroke recurrence and large-vessel occlusion, owing to its unique anatomical and hemodynamic characteristics, which may lead to more frequent carotid revascularization in clinical practice. In our case, a patient with carotid web experienced status epilepticus after CAS, inferred to be caused by the above characteristics. Combining the clinical practice and current studies, we found that intravenous SV infusion could terminate the abnormal status secondary to stroke. Subsequent transition to newer-generation oral antiseizure medications is preferred, given their neutral impact on secondary stroke prevention. We hope this case report could provide helpful suggestions for clinicians managing this rare complication in patients with carotid web. Further clinical application and prospective studies are warranted to validate our findings.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251386171 - Supplemental material for Status epilepticus of carotid web after carotid artery stenting: A case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605251386171 for Status epilepticus of carotid web after carotid artery stenting: A case report by Xiao-Jun Jing, Ling Yan, Hai-Zhen Hao, Bo Long, Peng-Cheng Wu, Jiao Wang, Xiao Yuan, Yong Tan and Xun-Jun Li in Journal of International Medical Research
Footnotes
Acknowledgements
None.
Author contributions
Xiao-Jun Jing: Conceptualization, Investigation, Writing–original draft. Ling Yan: Investigation. Hai-Zhen Hao: Investigation. Bo Long: Writing–original draft. Peng-Cheng Wu: Visualization. Jiao Wang: Conceptualization. Xiao Yuan: Conceptualization. Yong Tan: Supervision. Xun-Jun Li: Writing–review & editing.
Consent for publication
Written informed consent was obtained from the patient and his legal guardian for publication of this case report.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical approval
The case report involved the retrospective analysis of a single patient’s medical history, and the need for ethical approval was waived.
Funding
The authors report no funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.