
Abstract
Retroperitoneal ectopic pregnancy is an extremely rare form of ectopic pregnancy that can be life-threatening due to severe intra-abdominal hemorrhage. Retroperitoneal ectopic pregnancy is frequently misdiagnosed because of its atypical location and nonspecific symptoms. To the best of our knowledge, no previous cases of ectopic pregnancy localized to the mesorectum have been reported to date. Here, we present the case of a woman in her mid-30s with retroperitoneal ectopic pregnancy localized to the mesorectum. The condition was initially misdiagnosed as gastroenteritis due to atypical symptoms, which resulted in delayed treatment. This study aimed to improve the clinical recognition of mesorectal ectopic pregnancy among physicians.
Keywords
Introduction
Ectopic pregnancy (EP) is a common gynecological emergency and the leading cause of maternal mortality in early pregnancy. Tubal pregnancy represents the most frequent type, while abdominal EP (AEP), such as hepatic pregnancy, is considerably rarer. 1 AEP is defined as the implantation of a fertilized egg within the peritoneal cavity. Retroperitoneal EP (REP), a distinct subtype of AEP, is exceptionally uncommon. 2 REP involves abnormal implantation in the retroperitoneal space and is often overlooked or misdiagnosed because of its nonspecific clinical presentation. 3 Given the abundance of major blood vessels and nerves in the retroperitoneum, rupture of the gestational sac can result in life-threatening hemorrhage.4,5 The reported incidence of REP is less than 1/30000 pregnancies, with only approximately 40 documented cases to date.6,7 Notably, no prior cases of EP localized to the mesorectum have been reported to date. Recently, we encountered a case of mesorectal EP at our hospital. Although advances in transvaginal ultrasound, β-human chorionic gonadotropin (β-HCG) testing, and laparoscopy have significantly improved the diagnosis and management of EP, rare implantation sites remain poorly understood. This knowledge gap often leads to delayed intervention, severe complications, and even maternal mortality.
Case report
The reporting of this study conforms to the Case Report (CARE) guidelines. 8 We have deidentified all patient details. In January 2025, a woman in her mid-30s presented to the gastroenterology department of a local hospital with a 2-day history of stomach discomfort at rest, accompanied by nausea and vomiting. The patient received an initial diagnosis of gastroenteritis and was treated with supportive measures. Her symptoms persisted for 2 weeks without significant improvement, prompting presentation to the emergency department of Tianjin Medical University Baodi Hospital with new-onset lower abdominal and lumbar pain. Her menstrual history revealed regular 30-day cycles. At presentation, she had stopped menstruating for 33 days without associated vaginal bleeding or abnormal tissue discharge. No prior pregnancy testing had been performed. Her obstetric history included two cesarean deliveries and four induced abortions. There was no history of assisted reproductive technology, prior ectopic pregnancies, or endometriosis. Additionally, she had no high-risk factors such as smoking or intrauterine device exposure. At admission, β-HCG measurements demonstrated a decline from 7675 mIU/mL on the first day to 6956 mIU/mL on the third day and 6632 mIU/mL on the fourth day (Figure 1). Transvaginal ultrasound revealed normal uterine morphology and bilateral adnexa without pathological findings. Abdominal computed tomography (CT) and magnetic resonance imaging (MRI) revealed an ovoid mass on the right side of the rectum (Figure 2). Based on these findings, the senior consulting gynecologist suspected a diagnosis of REP localized to the mesorectum. Following multidisciplinary consultation involving anesthesia, gynecology, colorectal surgery, and vascular surgery specialists, a laparoscopic procedure was performed to confirm the diagnosis and provide treatment. Written informed consent for treatment was obtained from the patient.

Changes in serum β-HCG levels over the course of treatment in this case. β-HCG: beta-human chorionic gonadotropin.

Imaging manifestations. CT and MRI (a, b, c, white arrows) revealed a well-circumscribed, thick-walled cystic mass in the mesorectum. The T1 fat-saturated sequence confirmed intralesional hemorrhagic components (d, black arrow). The sagittal T2WI image showed that the lesion had a well-defined hypointense capsule (e, blue arrow). CT: computed tomography; MRI: magnetic resonance imaging.
The patient underwent laparoscopic examination under general anesthesia. Examination of the pelvic cavity revealed a morphologically normal uterus with regular contours and intact serosal surfaces. The right ovary contained a 1.5-cm corpus luteum, while the left ovary and bilateral fallopian tubes appeared grossly normal without pathological findings. A 3-mm peritoneal defect was observed on the right side of the rectum, without active bleeding. Through this opening, a cystic retroperitoneal mass containing clot-like material was visualized. Based on preoperative assessment, the retroperitoneal lesion and the right ovarian corpus luteum were scheduled for resection. An incision was made in the peritoneum adjacent to the inner aspect of the right sacral ligament using an ultrasonic scalpel. The retroperitoneal lesion was carefully dissected using blunt and sharp techniques. The lesion was located slightly closer to the right rectal wall. To avoid rectal injury, the ultrasonic scalpel was used in close contact with the tumor surface. The cystic mass containing clot-like tissue was successfully removed. The mass had a moderately thickened wall with villous-like structures. The rectal muscle layer remained intact. A partially lobulated cystic cavity extending into the right posterior mesorectum was noted, containing a small amount of clear, blood-tinged fluid. Considering its proximity to the rectum and its vascular supply, the partially lobulated cystic cavity was left in situ. Hemostasis was achieved using bipolar electrocoagulation. Postoperative histopathological analysis confirmed that REP was localized to the mesorectum (Figure 3). The patient’s β-HCG level decreased to 1294 mIU/mL on the second postoperative day and further declined to 252 mIU/mL on the third day (Figure 1). After her condition stabilized, she was discharged. Two weeks later, her β-HCG level returned to normal. At the 4-month follow-up, no local recurrence was observed, indicating a favorable prognosis. The patient was reassured that a normal future pregnancy is possible.
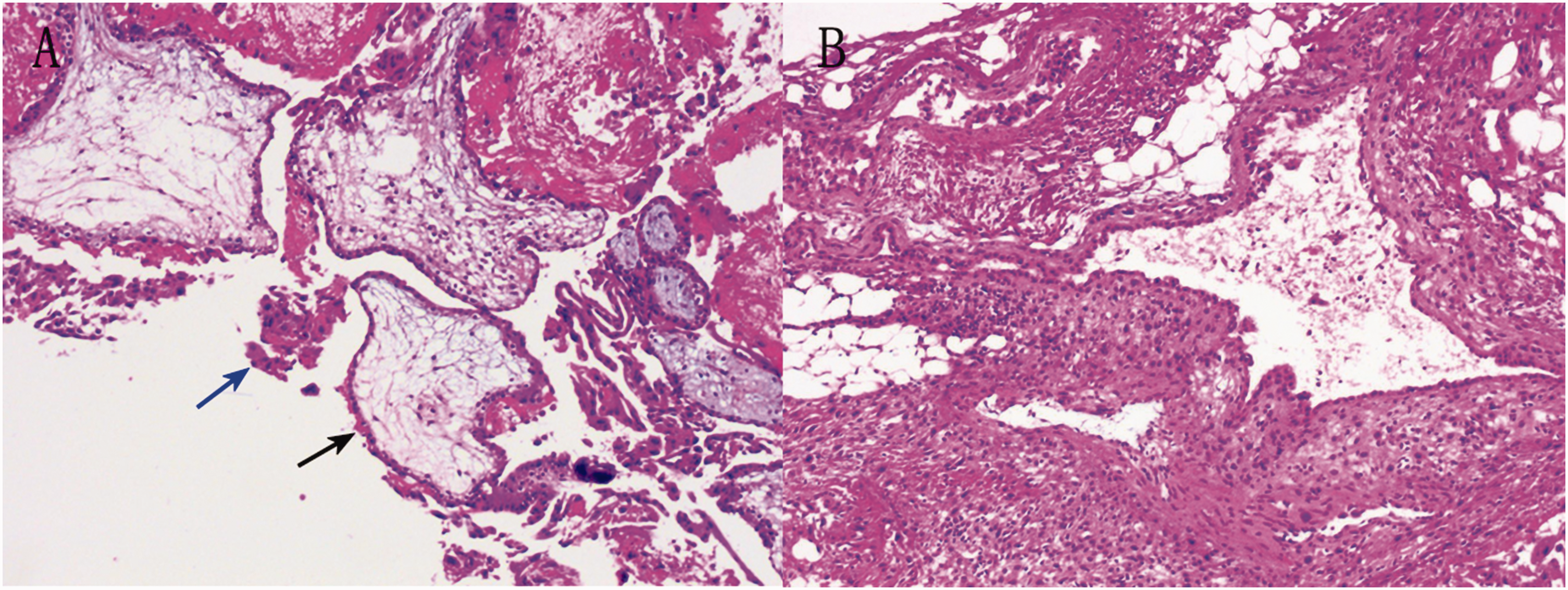
Pathological diagnosis. Hematoxylin and eosin staining; original magnification 40×. (a) Chorionic villi (black arrow) and trophoblastic cells (blue arrow) are visible and (b) a small amount of suspected decidual-like tissue is shown. Arrow colors are explained in the figure.
Discussion
EP occurs when a fertilized egg implants and develops outside the uterine cavity. 5 As a common gynecological emergency, EP is the leading cause of maternal mortality in early pregnancy. 6 The most frequent type is tubal pregnancy, followed by ovarian, abdominal, cervical, and broad-ligament pregnancies. REP is exceptionally rare; most cases of EP are reported between the abdominal aorta and inferior vena cava. 6 Other documented sites include the kidneys, pancreas, obturator fossa, pelvic retroperitoneum, and iliac artery. In our case, EP was localized to the mesorectum—a site not previously reported in the literature. Le and Nguyen 7 reported a case of EP localized to the right posterior rectal wall (Table 1). Although similar in location to our case, our patient’s lesion was specifically located within the mesorectum. MRI revealed a well-circumscribed mass with a distinct capsule, clearly demarcated from the rectum. The pathogenesis of mesorectal EP remains incompletely elucidated. Current literature suggests several potential mechanisms as follows: (a) secondary implantation of viable trophoblastic tissue following tubal rupture or spontaneous abortion; (b) lymphatic dissemination of the fertilized ovum; and (c) iatrogenic factors related to assisted reproductive technologies.5,14–17 The latter mechanism may involve tubal damage, leading to abnormal communications with the retroperitoneum. Notably, our patient’s history of two cesarean deliveries and four induced abortions may have predisposed the patient to pelvic inflammatory changes, potentially creating a pathway for trophoblastic invasion and subsequent mesorectum implantation.
Reports of REP localized to the mesorectum and rectal ectopic pregnancy.

β-HCG: beta-human chorionic gonadotropin; CT: computed tomography; GA: gestational age; GP: gravidity–parity; GS: gestational sac; MRI: magnetic resonance imaging; Mtx: methotrexate; US: ultrasound.
The clinical presentation of REP is nonspecific and varies according to the implantation site. 16 Although abdominal pain represents the most common symptom, some cases remain entirely asymptomatic. Symptom onset typically occurs when the growing pregnancy exerts a mass effect on adjacent structures. In cases of rupture, acute hemorrhagic shock may develop rapidly due to retroperitoneal bleeding. 17 Le and Nguyen 7 reported that the rectal pregnancy sac was initially overlooked during the first laparoscopy because of its atypical anatomical location (Table 1). The patient initially presented with epigastric discomfort, accompanied by nausea and vomiting, which subsequently progressed to lower abdominal and lumbar pain. Because of this atypical presentation, the initial working diagnosis was gastroenteritis. This case has highlighted a profound lesson: the clinical symptoms of REP localized to the mesorectum are not typical. A comprehensive evaluation including detailed medical history and menstrual cycle assessment is essential. Timely measurement of β-HCG levels combined with imaging studies, such as ultrasonography, CT, and MRI, is critical for establishing a definitive diagnosis.
The differential diagnoses include trophoblastic tumor, tailgut cyst, teratoma, epidermoid cyst, and extragastrointestinal stromal tumor. CT demonstrates high diagnostic accuracy in detecting pregnancy lesion rupture and identifying associated retroperitoneal hematomas. MRI offers superior soft-tissue characterization, providing exceptional value in delineating the anatomical relationship between the EP and surrounding structures and guiding optimal surgical planning. 18 In the current case, CT and MRI were crucial in identifying the lesion site and guiding subsequent treatment.
REP localized to the mesorectum is extremely rare, with no specific treatment guidelines for surgeons. 19 Le and Nguyen 7 reported successful conservative management of both rectal EP and REP using methotrexate therapy and expectant approaches. 20 These findings hold particular clinical relevance for EP at atypical sites. Optimal treatment requires individualized decision-making based on the following: (a) gestational age; (b) gestational sac characteristics (size and location); (c) clinical presentation; (d) β-HCG levels; and (e) patient preferences. 21 Primary management approaches for mesorectal EP involve either meticulous surgical excision of the gestational mass to preserve intestinal integrity or medical therapy (typically methotrexate) to avoid iatrogenic bowel injury. The choice between these modalities depends on careful risk–benefit assessment (Table 1). 7 Conservative treatment is applicable when the condition is stable and there is no active bleeding.7,20 Upon hospital admission, we initially pursued expectant management rather than immediate surgical intervention due to the following reasons: (a) the β-HCG levels demonstrated a suboptimal decline (<15% over 48 h during the 4-day observation period); (b) the patient’s symptoms persisted without clinical improvement; (c) our multidisciplinary team (including gynecologists and radiologists) had limited prior experience with mesorectal EP and could not definitively exclude malignant pathology; and (d) the patient expressed strong preference for surgical intervention due to concerns about potential life-threatening hemorrhage. After careful consideration of these factors, we proceeded with surgical management. Previous studies have demonstrated that EPs frequently develop along major vascular pathways, posing substantial technical challenges for laparoscopic management.4,6,22 In our case, the lesion’s proximity to the rectal wall elevated surgical risks, particularly regarding potential injury to adjacent vascular and neural structures. Despite these challenges, the procedure was successfully completed through comprehensive preoperative planning, including detailed imaging assessment, multidisciplinary consultation, and contingency preparation for vascular complications. This case highlights the critical importance of meticulous surgical preparation for mesorectal EP and provides a valuable management framework for similar cases.
Mesorectal EP represents an exceptionally rare clinical entity associated with significant diagnostic challenges. A heightened clinical suspicion is essential, particularly when patients present with atypical symptoms and inconclusive ultrasound findings. In such cases, advanced imaging modalities (CT/MRI) become crucial for confirming the diagnosis of atypically located EP, assessing surgical risks and potential complications, and differentiating EP from neoplastic lesions in the mesorectum through combined assessment of β-HCG levels and radiologic features. Optimal management requires a multidisciplinary approach. Surgical resection may be feasible for well-demarcated lesions, as in our case, whereas cases with rectal wall involvement present greater technical difficulty. For hemodynamically stable patients without active hemorrhage, conservative strategies including methotrexate therapy or expectant management represent viable alternatives.
Conclusion
REP localized to the mesorectum is an exceptionally rare clinical condition. Its unusual anatomical location and nonspecific clinical presentation often lead to diagnostic delays or misdiagnosis. Maintaining a high index of suspicion for mesorectal EP is crucial, as advanced imaging modalities significantly improve diagnostic accuracy. A multidisciplinary team approach is crucial, with management strategies tailored to individual patient circumstances to best optimize reproductive and overall health outcomes.
Footnotes
Acknowledgments
We are grateful to the emergency department team, gynecology department team, anesthesiology department team, vascular surgery department team, and gastrointestinal surgery department team of Tianjin Medical University Baodi Hospital for their medical help. We also appreciate the pathological support provided by the Department of Pathology. We would like to extend our special thanks to all colleagues who contributed to this study.
Author contributions
Junpeng Liu: investigation, validation, visualization, writing–original draft, writing–reviewing and editing. Lianzi Liu: conceptualization, project administration, resources, supervision. Yue Yu: conceptualization, project administration, resources, supervision. Zhenwei Miao: Supervision, validation, writing–review and editing.
Data availability statement
The data supporting the findings of this study can be accessed from the corresponding author upon reasonable request.
Declaration of conflicting interests
None of the authors have any potential conflicts of interest.
Funding
This study was sponsored by Institutional Research Project of Tianjin Medical University Baodi Hospital (No. BDYYMS202405).
Patient consent form
Written informed consent was obtained from the patient for the publication of anonymized information.