
Abstract
A woman in her early 50s was admitted to our hospital with a right retroperitoneal tumor that had been detected >1 year ago. Imaging studies revealed a mass in the right middle and lower retroperitoneum, which involved the upper portion of the right fallopian tube and caused dilated hydronephrosis of the right renal pelvis and calyces. Initial diagnosis suggested benign intraventricular smooth muscle neoplasia. She underwent surgical resection of the right retroperitoneal tumor, along with thrombectomy of the right renal vein and inferior vena cava, as well as artificial revascularization of the right renal vein. Postoperative pathology confirmed retroperitoneal smooth muscle sarcoma. She received postoperative chemotherapy with ifosfamide and doxorubicin as well as anticoagulation therapy with rivaroxaban. One year later, follow-up imaging revealed multiple nodules in the right middle and lower abdomen, a blurred nodule in the tail of the pancreas, and a dilated pancreatic duct in the distal pancreas, raising suspicion of metastasis.
Keywords
Introduction
Primary retroperitoneal tumors are neoplasms that originate in the retroperitoneal space, developing within tissues abundant in adipose tissue, lymph, muscle, and fascia. The incidence of these tumors is low, accounting for only 0.07% to 0.20% of all systemic tumors. 1 Statistics indicate that approximately 60%–80% of all primary retroperitoneal tumors are malignant, with smooth muscle sarcoma, liposarcoma, and malignant lymphoma being the most prevalent tumors. 2 Smooth muscle sarcoma is classified as a soft tissue sarcoma, originating from smooth muscle tissue. Although it is relatively rare, it exhibits a high degree of malignancy and poor prognosis. It primarily arises from organs rich in smooth muscle cells, such as the uterus. Retroperitoneal smooth muscle sarcoma constitutes 21% of retroperitoneal soft tissue tumors. 2 Intravascular leiomyomatosis (IVL) is a rare form of smooth muscle neoplasia characterized by the growth of nodular masses of histologically benign yet potentially malignant muscle cells within the veins. 3 Retroperitoneal smooth muscle sarcoma originating from the ovarian vein is particularly rare. This report retrospectively analyzed the clinical diagnosis and treatment of a patient with retroperitoneal smooth muscle sarcoma arising from the right ovarian vein, which invaded the right renal vein and inferior vena cava. Additionally, it summarized the differences and similarities in the preoperative diagnosis, clinical characteristics, treatment methods, and outcomes of intravascular smooth muscle neoplasms and retroperitoneal smooth muscle sarcomas, integrating relevant clinical data and literature review to provide references for the standardization of diagnosis and treatment of both conditions in the future.
Case presentation
A woman in her early 50 s was admitted to our hospital for a right retroperitoneal tumor detected >1 year ago. In April 2021, she sought care at another hospital for low back pain, where positron emission tomography/computed tomography (PET/CT) revealed a soft tissue mass in the right retroperitoneal area with increased glucose metabolism, suggestive of a neoplastic lesion. Surgical treatment was recommended; however, the patient refused surgical treatment and was discharged without appropriate intervention. She returned to our hospital (Yunnan Cancer Hospital, The Third Affiliated Hospital of Kunming Medical University, Peking University Cancer Hospital Yunnan Hospital) in August 2022, reporting a worsening of her back pain that had begun 2 weeks before admission. She underwent radical mastectomy for breast cancer in 2016, followed by 8 rounds of postoperative chemotherapy and 16 rounds of radiotherapy. She also underwent cholecystectomy in 2012 at a local hospital. Upon admission, her physical examination revealed no significant abnormalities. Comprehensive evaluations, including blood cell analysis, tumor marker assessment, other blood tests, electrocardiogram, and echocardiogram, showed no notable irregularities.
On 5 August 2022, the patient was admitted to the hospital and underwent a comprehensive upper, middle, and lower pelvic sweep, along with enhanced CT. Imaging revealed a right middle and lower retroperitoneal mass measuring approximately 5.3 cm × 4.4 cm × 10.1 cm (Figure 1). The lower edge of the lesion reached the level of the iliac vessel bifurcation, with the right ovarian vein appearing thickened and tortuous. The mass also involved the right renal vein and the adjacent inferior vena cava, partially displacing the right lumbar muscle and the lower horizontal segment of the duodenum from the right renal vein. These lesions encircled the adjacent ventral segment of the right ureter, resulting in dilated right hydronephrosis. Additionally, multiple nodules and masses in the uterus are likely uterine fibroids, while low-density foci in the bilateral adnexal regions are considered ovarian manifestations.

Preoperative enhanced CT of the abdomen. CT: computed tomography.
The patient was admitted to the hospital. An upper and middle abdominal scan was performed along with enhanced magnetic resonance imaging (MRI) on 11 August 2022. Imaging revealed an irregular mixed-signal mass in the right middle and lower retroperitoneum, characterized by a distinct boundary (Figure 2). The lesion exhibited a pushing growth and extended along the right ovarian vein and right renal vein, partially protruding into the inferior vena cava; it measured 4.0 cm × 5.4 cm × 14.2 cm. This finding was considered the most significant imaging manifestation of IVL. Additionally, the lesion involved the upper portion of the right ureter, leading to dilated hydronephrosis of the right renal pelvis and calyces.
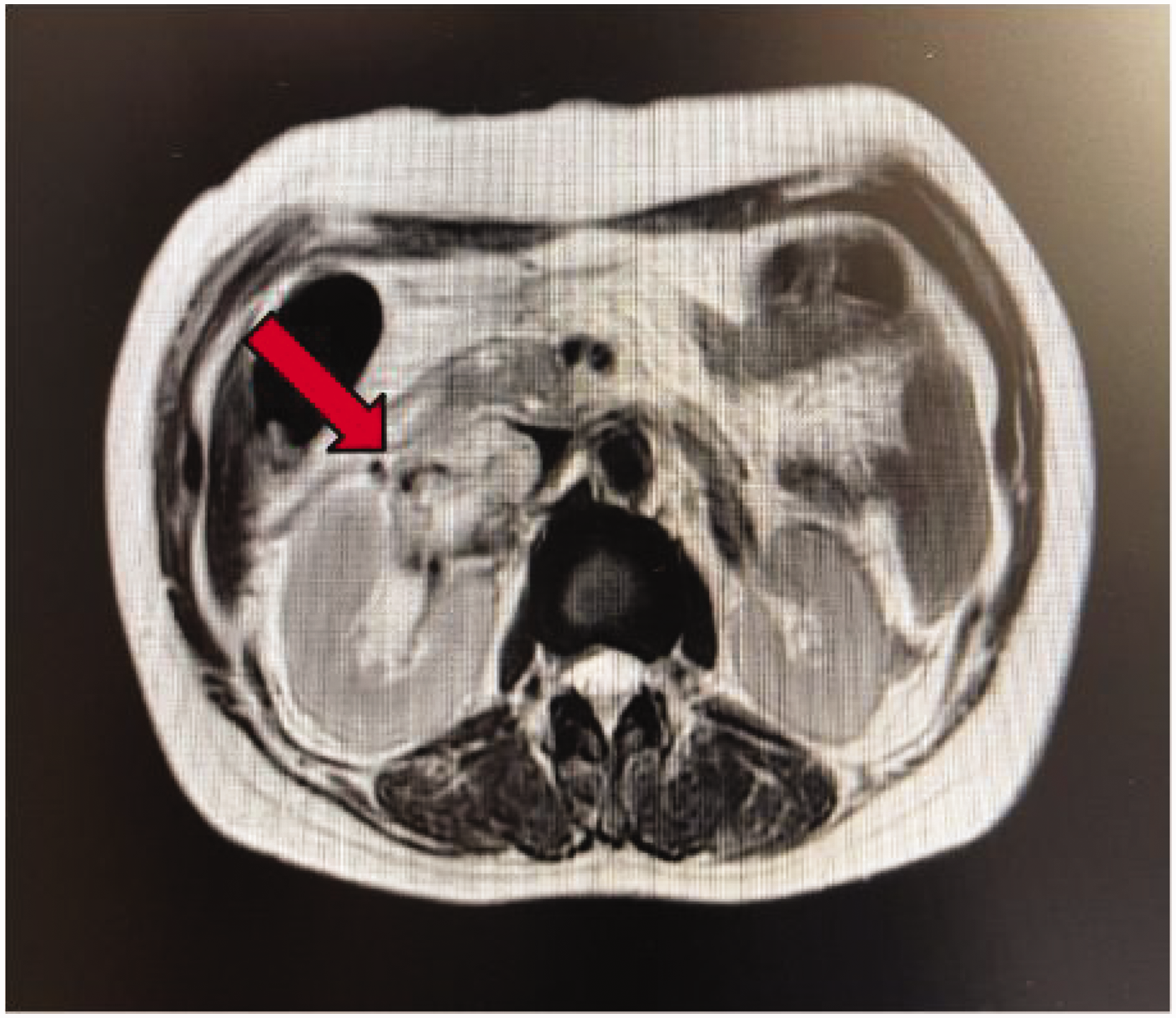
Preoperative enhanced MRI of the abdomen. MRI: magnetic resonance imaging.
Preoperative renal function nuclear imaging showed no obvious abnormalities in the patient’s renal function.
The patient’s preoperative upper, middle, and lower pelvic sweep, along with enhanced CT, indicated that the retroperitoneal mass in the right middle and lower regions had a maximum diameter of approximately 10.1 cm. The lesion exhibited upward involvement of the right renal vein and the adjacent inferior vena cava, and it was poorly demarcated from the descending and horizontal segments of the duodenum as well as from the right lumbar muscle. Additionally, pelvic CT revealed multiple uterine nodules and masses consistent with uterine leiomyoma. Given the occurrence of intraventricular smooth myomatosis in middle-aged women with a history of uterine fibroids, the patient in this case was considered to be at high risk of intraventricular smooth myomatosis. As she had a history of primary malignant tumor, the tumor may have encased large blood vessels along its anatomical course, characterized by an irregular morphology. Furthermore, the presence of metastatic lymph nodes in the retroperitoneum could not be ruled out, leading to an unclear diagnosis that necessitated confirmation through postoperative pathology. Intraoperative exploration revealed that the tumor developed plastically along the right ovarian vein from the right parietal ovary, displacing the right upper ureter and partially adhering to the descending duodenum and right psoas major muscle. The tumor also exhibited superior invasion into the right renal vein and extension into the inferior vena cava, indicating the possibility of retroperitoneal smooth muscle sarcoma during the operation (Figure 3).

Intraoperative specimens.
IVL primarily occurs in women and is classified as a relatively rare disease characterized by the diffuse growth of smooth muscle tumors within the veins. Most of these tumors tend to be benign, and the onset is closely associated with uterine fibroids. CT typically reveals uterine enlargement, with isointense or slightly low-density mass shadows observed within the uterus or pelvic veins. The mass exhibits progressive enhancement during scan as well as venous enhancement, which can clearly delineate the extent of the tumor and its relationship with the surrounding blood vessels and organs. 4 However, smooth muscle sarcoma is a malignant tumor that arises from smooth muscle cells and can occur in various locations, including the retroperitoneum, uterus, and gastrointestinal tract. In the retroperitoneum, it may invade adjacent blood vessels, nerves, and organs. When the tumor is small, CT often shows a superficial appearance with uniform density. However, as the tumor grows, it may exhibit necrosis and hemorrhage, with significant enhancement observed during the venous phase. MRI findings typically reveal T1-weighted imaging with iso-low signals, T2-weighted imaging with iso-high signals, and extensive necrosis of the retroperitoneal mass, along with involvement of adjacent blood vessels, which is highly suggestive of this disease. 5
The preoperative diagnosis and evaluation for this patient are presented below. The preoperative diagnosis was stage III intraventricular smooth muscle neoplasia. Preoperative evaluation revealed the following: 1. the patient refused to undergo bilateral adnexa and hysterectomy; 2. the tumor involved the right renal vein, inferior vena cava, and right ureter, complicating kidney preservation; and 3. the tumor was poorly delineated from the descending and horizontal segments of the duodenum as well as right psoas major muscle, which posed a high surgical risk. In close collaboration with the multidisciplinary team (MDT), a surgical approach consisting of right retroperitoneal tumor resection, right renal vein and inferior vena cava thrombectomy, and right renal vein revascularization was undertaken. The right ureter was successfully detached; despite the tumor’s adherence to the duodenum and right psoas major muscle, it was completely resected along with the right renal vein. Artificial revascularization of the right renal vein was performed, successfully preserving the patient’s right kidney. The patient was discharged from the hospital 1 week postoperatively.
The surgical specimen, as depicted in Figure 3, revealed a right retroperitoneal tumor characterized by two grayish-white masses measuring 13 cm × 8 cm × 5 cm. The cut surface appeared grayish-white and solid, exhibiting slight toughness and a mucous texture. Histological examination revealed that the tumor cells were spindle-shaped. Immunohistochemical analysis yielded the following results: CK (−), vimentin (+), SMA (+), desmin (foci +), actin (+), S100 (−), MDM2 (−), Bcl-2 (foci +), EMA (+), CD34 (vasculature +), CD99 (+), TLE1 (−), CD117 (−), DOG1 (−), SDHB (+), Ki-67 (+, approximately 50%), calponin (+), CD31 (vasculature +), FLI-1 (weakly +), CD68 (foci +), and CD163 (partially +). These findings, in conjunction with hematoxylin and eosin staining and immunohistochemistry results, are illustrated in Figures 4 and 5, suggesting a diagnosis of smooth muscle sarcoma. The patient was discharged from the hospital after 1 week of postoperative anti-inflammatory and anti-infective symptomatic treatment. Although the patient was advised to undergo postoperative chemotherapy, she expressed an inability to continue due to financial constraints. Consequently, she was discharged after being informed of her condition and accepted the potential consequences of forgoing further treatment.
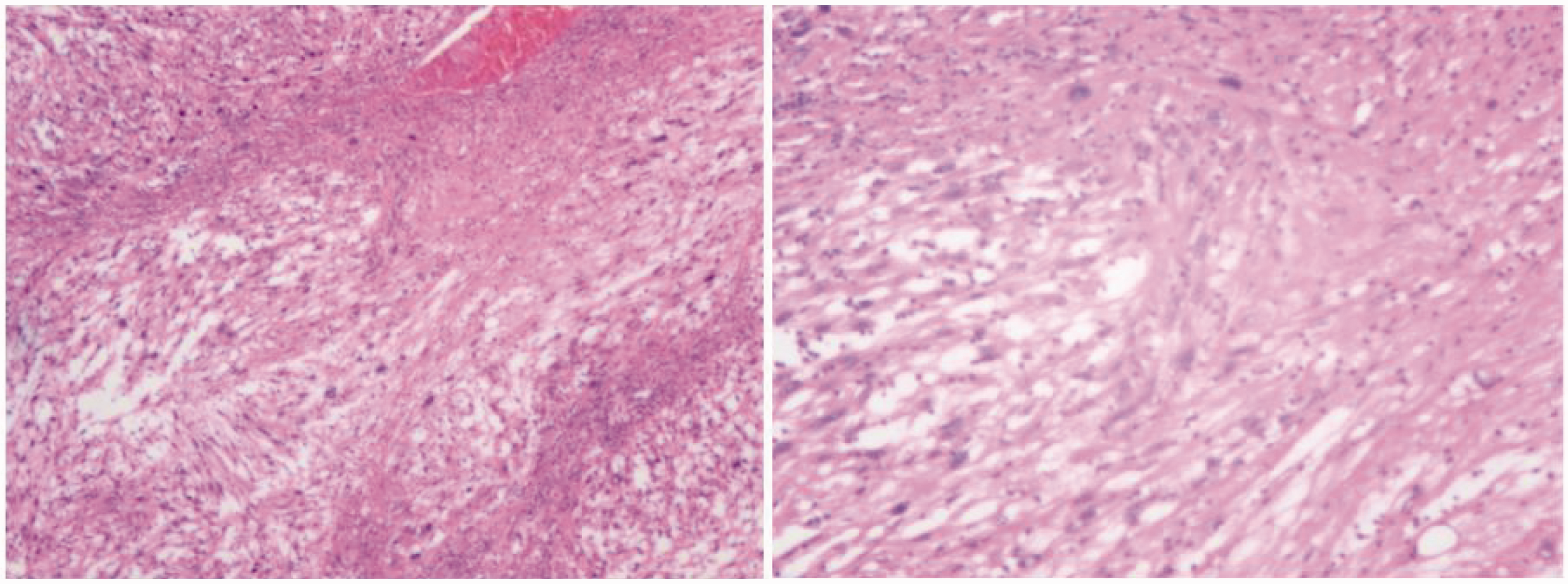
HE staining results on postoperative pathology. HE: hematoxylin and eosin.

Immunohistochemical findings on postoperative pathology.
In November 2023, the patient was re-evaluated at a local hospital, where pancreatic occupancy was identified. Consequently, she was admitted for a thorough examination, which raised concerns regarding the potential postoperative recurrence of retroperitoneal sarcoma. There were no absolute contraindications to chemotherapy, and the patient received chemotherapy with isocyclophosphamide (d1, 31.5 g) + doxorubicin hydrochloride (d1, 225 mg) on 28 November 2023. The chemotherapy process proceeded smoothly; however, the patient experienced significant digestive reactions and was subsequently discharged after receiving symptomatic supportive treatment. Upon admission, she was diagnosed with the following: (a) postoperative recurrence of malignant tumor in the retroperitoneal cavity; (b) secondary malignant tumor of the pancreas; (c) secondary malignant tumor of retroperitoneal lymph nodes; (d) hypertension; (e) a history of malignant breast tumor; and (f) right renal pelvic hydronephrosis. The medical team advised the patient to either maintain ureteral stenting tubes or undergo right nephrostomy to address the hydronephrosis. However, the patient and family members expressed their understanding of the condition, prognosis, and associated risks, ultimately refusing the recommended treatment. The patient requested to be discharged to a general hospital for management of hydronephrosis. The medical team reiterated the necessity of either indwelling ureteral stenting tubes or right nephrostomy, to which the patient and family acknowledged their understanding and firmly requested discharge. The final treatment outcome for this patient is subject to further follow-up.
Discussion
Smooth muscle sarcoma is a relatively rare malignant tumor, accounting for approximately 11% of all soft tissue tumors. 6 The rectum is the most common site for smooth muscle sarcoma, representing approximately 85% of colorectal smooth muscle sarcomas. In contrast, angio-smooth muscle sarcomas are less common and are characterized as tumors of mesenchymal origin with distinctive vascular invasive properties. 7 Ovarian venous smooth muscle sarcoma, a specific subtype of angio-smooth muscle sarcoma, is rarely reported worldwide. 8
This case report shares several critical similarities with the recent report by Imbriani et al., 9 who described a left gonadal vein leiomyosarcoma (LMS) managed with neoadjuvant chemotherapy and en bloc resection. Both cases involved middle-aged women presenting with nonspecific abdominal pain and hydronephrosis secondary to retroperitoneal mass compression, underscoring the insidious clinical presentation of gonadal vein LMS. Notably, Imbriani et al. highlighted the diagnostic challenge posed by overlapping imaging features between LMS and benign entities such as IVL, a dilemma also encountered in our case. However, although the patient in the previous case underwent preoperative biopsy, which confirmed LMS prior to chemotherapy, we could not establish a definitive preoperative diagnosis initially due to imaging ambiguity, reflecting the heightened complexity of differentiating vascular LMS from IVL without histopathological validation. The rarity of gonadal vein LMS, with only 17 cases being reported so far, 9 necessitates pooling insights across studies. Both cases reinforce the imperative for multidisciplinary collaboration to optimize surgical planning and adjuvant strategies, particularly in anatomically complex retroperitoneal tumors.
Given the rarity of both retroperitoneal smooth muscle sarcoma and intraventricular smooth muscle neoplasia along with the nonspecific nature of imaging manifestations during clinical diagnosis, the diagnostic process is often complicated with more common diseases. In this case, the initial CT and MRI findings primarily led to a diagnosis of IVL, largely because IVL is relatively well-recognized by clinicians and the patient had a history of uterine fibroids, which aligns with certain characteristics of IVL. 2 Additionally, PET/CT could not provide a definitive diagnosis. The imaging studies indicated that the tumor was growing along the blood vessels, resembling the presentation of IVL; however, it was not possible to accurately differentiate the benign characteristics of the tumor from the malignant ones. This underscores the importance of not relying solely on imaging findings for diagnosis in complex cases but rather integrating the patient’s medical history, clinical manifestations, and other diagnostic tools to arrive at a comprehensive assessment.
Although various preoperative tests suggest a diagnosis, definitive confirmation still relies on pathological examination. Primary retroperitoneal smooth muscle sarcoma exhibits a high degree of malignancy; however, the risk of needle tract implantation metastasis following a puncture biopsy is minimal; therefore, it is not advisable to forgo puncture. 10 In this case, the preoperative diagnosis was inconclusive, raising the question of whether we can improve the preoperative pathological biopsy method for such suspected cases.
Complete surgical resection of the tumor is essential for minimizing the risk of postoperative tumor recurrence and metastasis as well as for prolonging the patient’s life expectancy. 11 An MDT approach is recommended for preoperative discussions and is crucial during the surgical procedure. 12 Additionally, postoperative radiotherapy and other adjuvant therapies may be necessary, underscoring the importance of an MDT in ensuring surgical success and reducing the likelihood of tumor recurrence in the postoperative period. In the present case, the choice of surgical approach presented numerous challenges. Preoperative evaluation revealed several complications as follows: (a) the patient declined bilateral adnexa and hysterectomy; (b) the tumor involved the right renal vein, inferior vena cava, and right ureter, complicating kidney preservation; and (c) the tumor was poorly demarcated from the descending and horizontal portions of the duodenum and right psoas major muscle, increasing the surgical risk. These factors complicate the surgical decision-making process, necessitating a thorough consideration of the patient’s preferences, extent of tumor invasion, and feasibility and safety of the surgical intervention. Although laparoscopic surgery offers advantages such as rapid postoperative recovery compared with open surgery, a comprehensive evaluation of the tumor’s extensive nature and its challenging location is needed to guide the choice of surgical approach. 13 Finally, the surgical plan was established, consisting of right retroperitoneal tumor resection, right renal vein and inferior vena cava tumor thrombectomy, and right renal vein artificial revascularization, following an MDT consultation. The primary prognostic factors influencing postoperative overall survival and progression-free survival include age, tumor size, histological grade, pathological subtype, multifocality, and the performance of simultaneous resection. 14
Currently, the efficacy of neoadjuvant chemotherapy for this disease remains unclear, necessitating further investigation into chemotherapy regimens and patient selection criteria for this treatment modality. Additionally, there is currently no high-level evidence to substantiate the role of preoperative neoadjuvant therapy. Isocyclophosphamide and epirubicin are commonly administered as postoperative adjuvant chemotherapy; however, it remains uncertain whether chemotherapy confers benefits across all pathologic subtypes. Relevant studies have indicated that chemotherapy can cause severe adverse effects; moreover, the efficacy of radiation therapy remains unclear.15,16 Genetic testing of soft tissue tumors facilitates the identification of novel genetic abnormalities, which is invaluable for molecular diagnosis and potential targeted therapeutic strategies in sarcomas. 17 Given the high malignancy and poor prognosis associated with this tumor, long-term follow-up is imperative to monitor the patient for tumor recurrence.
Intravenous LMS is a significant subtype of soft tissue sarcoma. Over the past few decades, the efficacy of treatments for soft tissue sarcoma has markedly improved. Nevertheless, the first-line pharmacological interventions remain centered around ifosfamide and anthracyclines. Palliative chemotherapy is predominantly employed, and there is currently no established standard for second-line or late-stage treatment. 16 Currently, the targeted therapies commonly utilized in clinical practice for soft tissue sarcoma primarily include antivascular targeted agents such as pazopanib and anlotinib 18 as well as specific molecular targeted therapies that target signal transduction pathways, including sirolimus, crizotinib, and tazemetostat.19,20 However, there are notable variations in the effectiveness of different targeted therapies for sarcomas originating from various tissues, which necessitates further molecular diagnostics.
Most patients with primary retroperitoneal LMS are asymptomatic in the early stages of the disease. Typically, they seek medical attention only when an abdominal mass is palpated or when the mass compresses adjacent tissues and organs, causing corresponding symptoms such as low back pain and hydronephrosis. However, clinical symptoms often manifest later, resulting in most patients being diagnosed at an advanced stage of the disease, leading to a poor prognosis. Clinically, both IVL and retroperitoneal LMS are relatively rare and exhibit similar features on imaging and other diagnostic examinations, complicating differentiation and potentially leading to the adoption of different treatment approaches. Therefore, when encountering patients with retroperitoneal tumors that present with IVL on imaging and other assessments, it is crucial to consider the possibility of LMS to devise the most effective treatment plan. 21
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251364059 - Supplemental material for A case report of retroperitoneal leiomyosarcoma originating from the right ovarian vein and invading the right renal vein and inferior vena cava
Supplemental material, sj-pdf-1-imr-10.1177_03000605251364059 for A case report of retroperitoneal leiomyosarcoma originating from the right ovarian vein and invading the right renal vein and inferior vena cava by Chengbin Lu, Leyu Zhang, Benmo Xu, Tianyu Li, Die Fan, Changyang Li, Yuanlong Shi, Xin Li and Bin Zhao in Journal of International Medical Research
Footnotes
Acknowledgments
We are grateful to the patient for participating in this study and providing permission for the publication of this case report.
Author contributions
Chengbin Lu and Leyu Zhang equally contributed to data collection and article writing. Benmo Xu, Tianyu Li, Die Fan, Changyang Li, and Yuanlong Shi checked the article and conducted literature review. Xin Li and Bin Zhao provided full guidance and supervision for article writing. All authors have read and approved the final manuscript.
Data availability statement
The original data presented in the study are included in the article or Supplementary Material. Further inquiries can be directed to the corresponding author.
Declaration of conflicting interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical statement and consent
After consultation with the Ethics Committee, the study was analyzed retrospectively and exempted from review.
Funding
This study was indeed supported by grants from the Kunming Medical University 2024 Graduate Education Innovation Fund (2024S341 and 2024S342).
Informed consent statement
Informed consent was obtained from the patient.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.