
Abstract
A middle-aged (46 years old) woman had been experiencing recurrent upper abdominal distension, nausea, and belching over a 2-year period. She underwent extensive gastrointestinal evaluations, including endoscopy, chest computed tomography, and abdominal ultrasound; she was diagnosed with chronic gastritis and treated with omeprazole (20 mg bid) and mosapride (5 mg tid) for 1 month, with no symptom relief. For further diagnosis and treatment, she visited The Second Hospital of Longyan in April 2023. Further investigations, including brain imaging and video electroencephalography, revealed medial temporal lobe cavernous malformation associated with epilepsy. She subsequently underwent expanded medial temporal lobectomy for removal of the lesion and the surrounding epileptogenic cortex. Postoperatively, her gastrointestinal symptoms resolved completely. This case highlights the importance of considering medial temporal lobe epilepsy in the differential diagnosis of patients presenting with recurrent, short-duration gastrointestinal complaints that are not resolved with conventional treatments.
Introduction
Epilepsy is a brain disorder characterized by abnormal neuronal discharges in the brain, which manifest as transient neurological disturbances. Sensory, motor, and autonomic functions as well as higher brain functions including perception, emotion, cognition, and behavior may be involved in epilepsy. Typically, the disturbances are paroxysmal, stereotyped, and repetitive in nature. Medial temporal lobe epilepsy may be associated with prodromal symptoms such as abdominal discomfort, rising epigastric sensation, palpitations, and other autonomic symptoms as well as psychological responses such as fear and déjà vu. Prodromal symptoms are followed by oropharyngeal and/or hand automatisms, which are accompanied with reduced movement and increased contralateral muscle tone. We present our experience in treating a patient with epilepsy caused by medial temporal lobe cavernous malformation (CM). In this patient, seizures appeared with nausea, vomiting, and upper abdominal distension alone.
Case report
Medical history
A middle-aged (46 years old) woman had been experiencing recurrent episodes of upper abdominal distension and nausea for the past 2 years. Each episode lasted for seconds and occurred dozens of times each day. During the seizure, her consciousness was clear; the seizure was unrelated to sleep, and her consciousness remained unaffected after the seizure. Gastrointestinal endoscopy, abdominal ultrasonography, and computed tomography (CT) of the chest suggested chronic gastritis. However, her symptoms did not improve with medical treatment. She had no family history of epilepsy.
Physical examination
The patient was right-handed. She was conscious and answered questions appropriately. Her both pupils were equal and reactive to light. The heart and lung examinations were normal. Her abdomen was soft and without tenderness or rebound tenderness. Bowel sounds were normal. Muscle strength and tone were also normal throughout the examination. Babinski test was negative.
Auxiliary testing
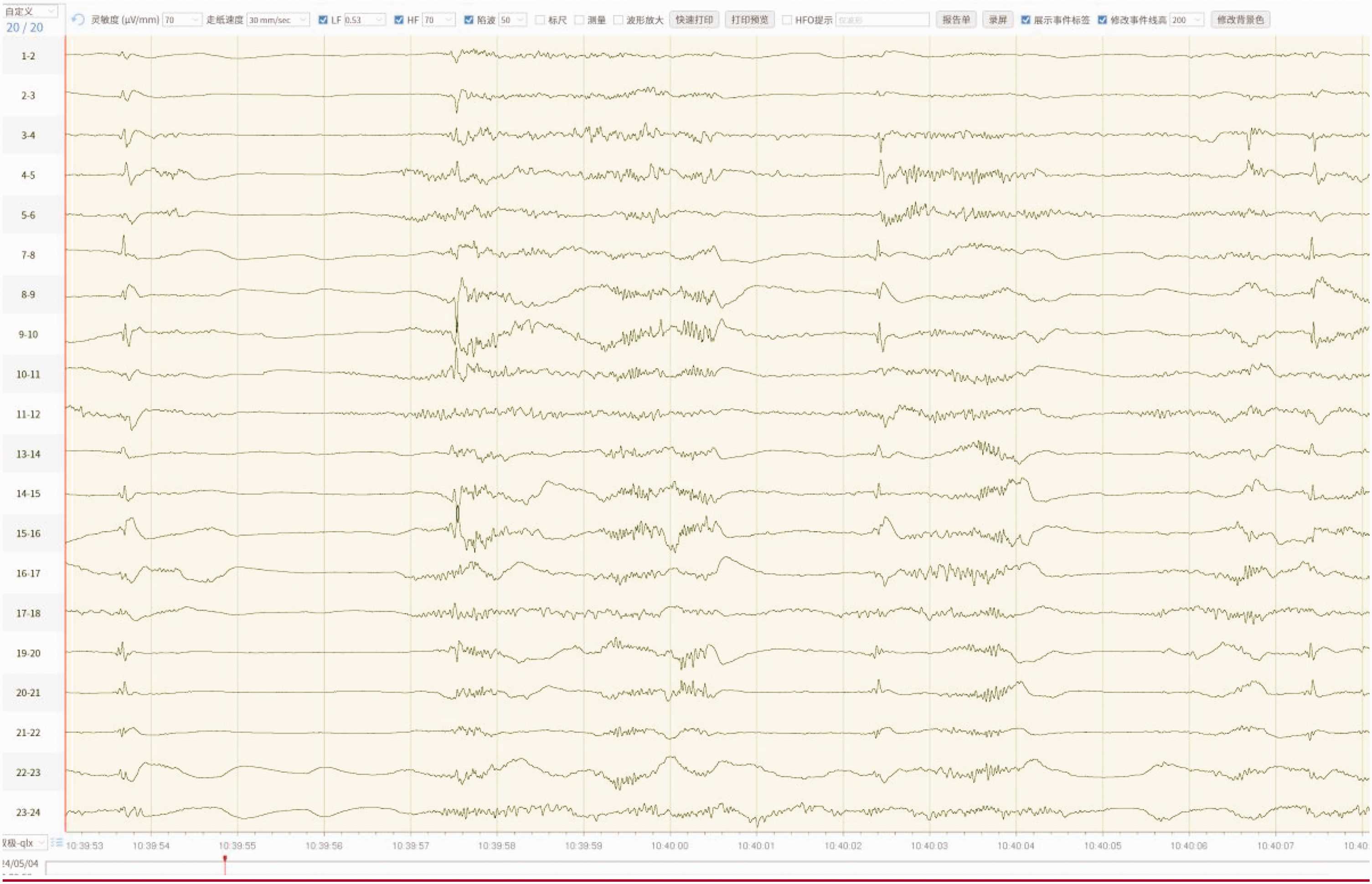
Head CT showed a high-density lesion in the right medial temporal lobe. Brain magnetic resonance imaging indicated that the lesion was a CM (Figure 1). Video electroencephalography performed during a seizure, which manifested as nausea, tachycardia, and a sensation of epigastric rising, showed significant sharp waves and spike-slow waves in the right frontal–temporal region lasting approximately 30 s (Figure 2). During the interictal period, recurrent low-amplitude sharp waves were observed in the right temporal region, frequently affecting the ipsilateral frontal region and contralateral temporal region (Figure 3).
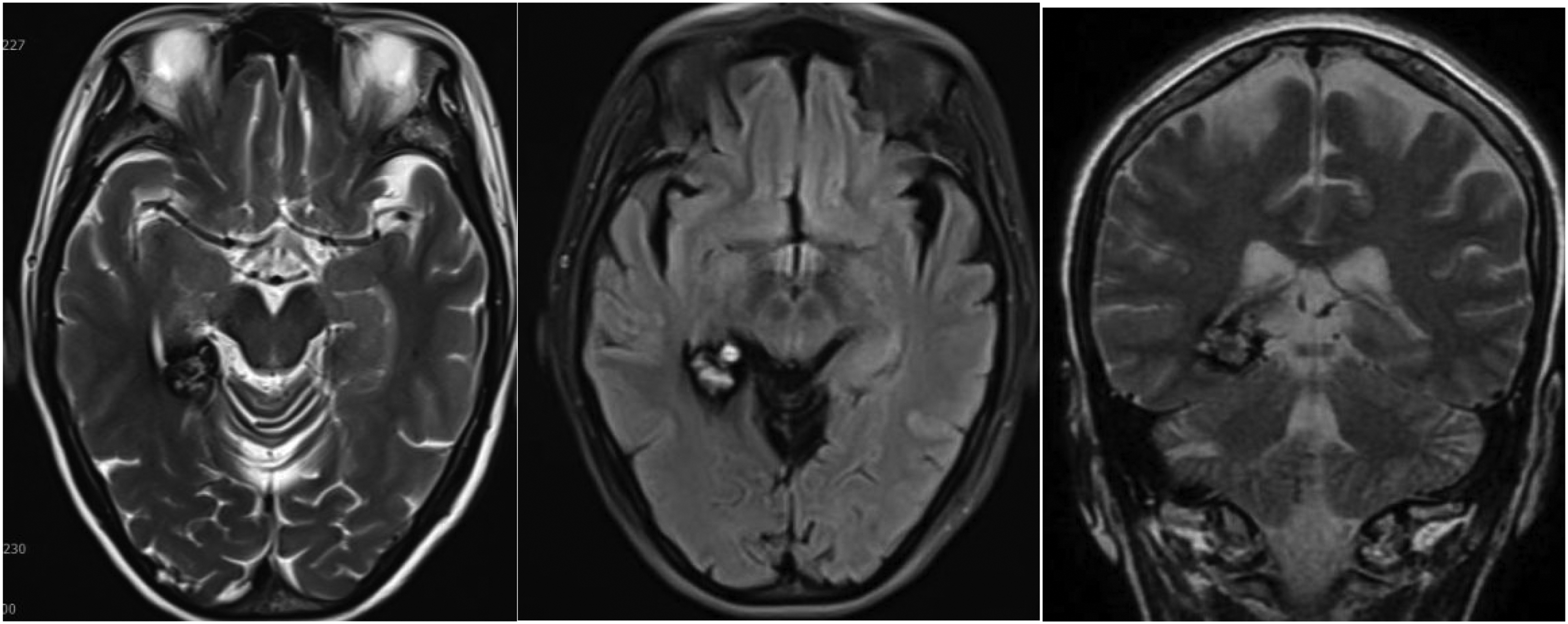
On T2-weighted imaging, T2-FLAIR sequences, and T2 coronal section, the lesion was characterized by mixed signal intensity in the center and low signal intensity in the surrounding area. FLAIR: fluid-attenuated inversion recovery.

Video encephalography during a seizure episode showing T4 and T6 spike waves and spike-slow complex waves.

VEEG monitoring suggesting recurrent low-amplitude sharp waves in the right temporal region, frequently involving the ipsilateral frontal region and contralateral temporal region.
Diagnosis
Two diagnoses were made: (a) epilepsy: focal onset, nonmotor onset, autonomic symptoms, and awareness and (b) right medial temporal lobe CM.
Treatment
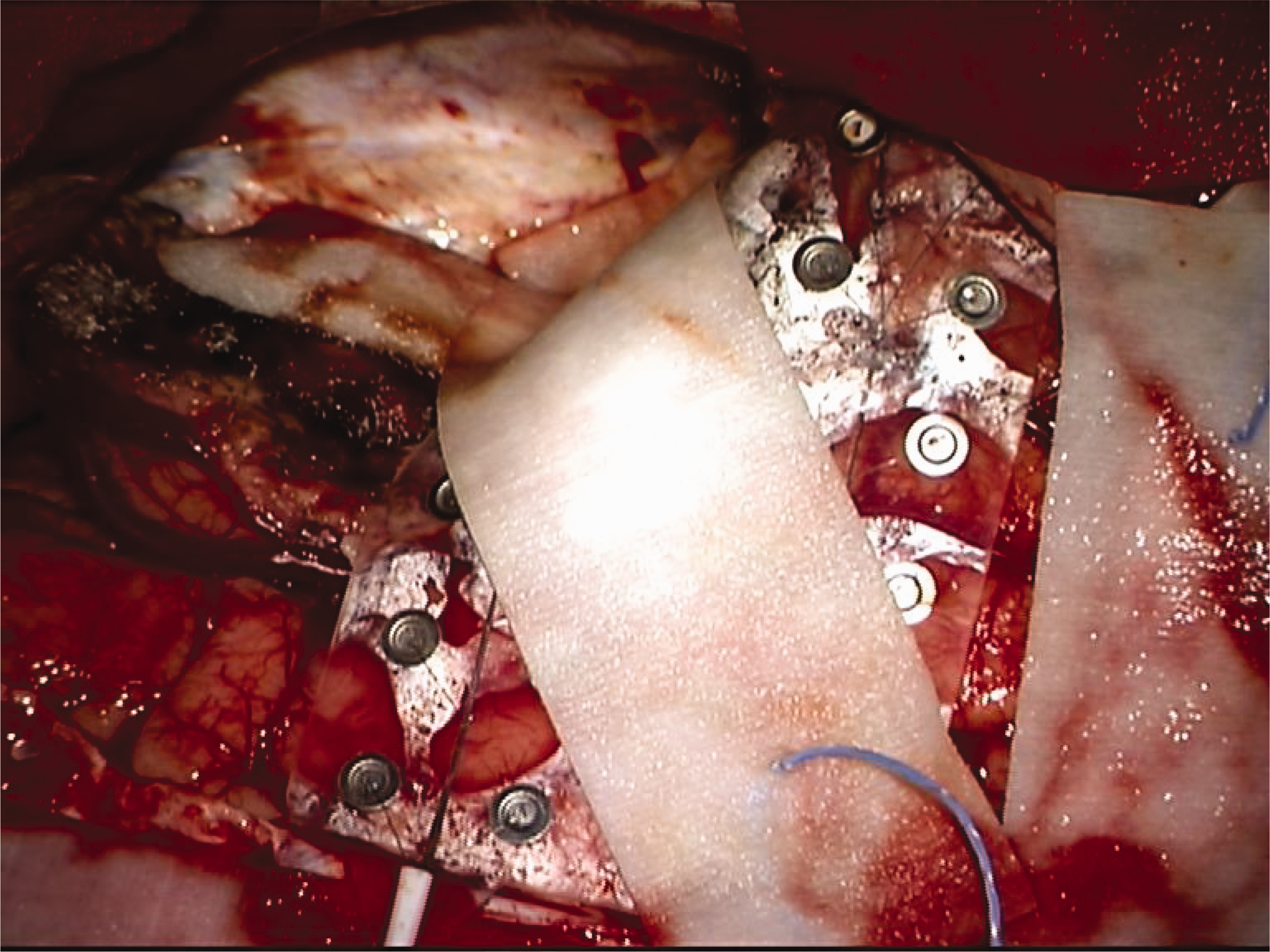
Symptoms improved, and the frequency of seizure decreased following pre-operative administration of sodium valproate. Temporal lobectomy was performed using intraoperative electrocorticography (ECoG) to guide resection of the CM and ipsilateral anteromedial temporal lobe (Figures 4–7). ECoG was performed using a 4 × 6 strip electrode.

A right frontotemporal craniotomy was performed to expose the frontal and temporal lobes and place electrocorticography leads on the brain surface.
ECoG (4 × 6) showing widespread electrical discharges in the monitored area. ECoG: electrocorticography.
Monitoring range of ECoG after right temporal lobe resection. ECoG: electrocorticography.

ECoG performed immediately after right temporal lobectomy showing disappearance of the electrical discharges. ECoG: electrocorticography.
Outcome
The patient recovered well after the operation and did not experience any further episodes of upper abdominal distension or nausea. Postoperative cognitive function has not shown any decline. Follow-up head CT indicated no bleeding in the surgical cavity and adequate resection (Figure 8). Histopathology of the surgical specimen was consistent with that of CM (Figure 9).

Postoperative computed tomography showing complete resection of the lesion and no significant bleeding in the surgical cavity.

Histopathology indicating a cavernous malformation.
Discussion
CMs, also known as cavernous angiomas or cavernous hemangiomas, are vascular malformations characterized by abnormal dilated blood vessels, which can form in various organs, including the central nervous system (CNS). The reported prevalence of CNS CMs in the general population ranges from 0.5% to 1%; however, the true prevalence could be higher owing to the presence of asymptomatic patients. 1 Although the exact etiology of CMs remains unclear, genetic factors, particularly mutations in the CCM1, CCM2, and CCM3 genes, have been associated with familial cerebral CMs.2,3 Most cases are sporadic and result from complex interactions between genetic and environmental factors.3,4
Patients with CNS CMs may present with various neurological symptoms depending on their location, including seizures, focal neurological deficit, and headache. 2 Seizures are common in patients with cerebral CMs, occurring in approximately 20%–50% of patients; these can vary in type and frequency.2,5 Seizures located in the brainstem or spinal cord may present with more complex symptomatology, including ataxia, dysarthria, or motor weakness.
CMs located in the medial temporal lobe often manifest as medial temporal lobe epilepsy.6,7 Typical symptoms include prominent prodromal symptoms such as abdominal discomfort, rising epigastric sensation, and autonomic symptoms as well as cognitive seizure symptoms such as hallucination and déjà vu. After the prodromal symptoms, patients may experience stupor, fixation, reduced activity, and decreased consciousness accompanied with oroalimentary and ipsilateral hand automatisms as well as reduced movement and increased muscle tone in the contralateral limbs. However, medial temporal CMs rarely present solely with gastrointestinal symptoms. Such cases are prone to misdiagnosis, as illustrated in our case.
Medial temporal lobe CMs frequently present with epilepsy; therefore, a comprehensive treatment approach is required. Treatment options include pharmacological management, radiotherapy, and surgical intervention.2,6–8 However, antiepileptic medications only address the seizures, and radiation is associated with a high rate of recurrence. Therefore, surgery is preferred. For lesion-related epilepsy, the primary goal of surgery is excision of the epileptogenic focus. However, the focus frequently resides in the cortical areas surrounding the lesion. 9 Therefore, it is necessary to remove both the lesion and the surrounding brain region containing any epileptogenic foci.
Additionally, medial temporal lobe CMs may be associated with temporal lobe cortical dysplasia in the adjacent brain (referred to as type IIIC focal cortical dysplasia). 10 Therefore, the surgical plan typically involves simple resection of both the medial temporal lobe (hippocampus and amygdala) and lesion using ECoG guidance; alternatively, expanded temporal lobectomy involving resection of the lesion, medial temporal lobe, and anterior temporal lobe may be performed.6,7,11 For patients with a longer history of epilepsy and extensive electrical discharges observed on ECoG, the latter option is usually selected. In our case, this option yielded excellent results.
The main finding from this case is that medial temporal lobe epilepsy should be considered in patients with recurrent short-duration episodes of gastrointestinal symptoms that do not improve after conventional treatment. If the symptoms include seizures caused by CM, surgical intervention can achieve an excellent outcome.
Footnotes
Acknowledgments
Author contributions
Yangzong Wu and Congli Luo designed the work; Limei Zheng, Xiaoxin Chen, and Zhiquan Fan collected and analyzed the data; and Yangzong Wu, Shuting Hong, Qiangwang Wu, and Congli Luo drafted the work and substantively revised it. All authors have read and approved the final manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interest
The authors have no conflicts of interest to disclose.
Ethics statement
The patient provided informed consent for the treatment received and for the publication of this case report. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved for publication by the institutional review board. We have de-identified all patient details, and the reporting of this study conforms to the Case Report (CARE) guidelines. 12
Funding
This study was supported by the Science and Technology Innovation Health Joint Fund Project of Longyan City, Fujian Province, China No. 2021LYF17046.