
Abstract
Fever of unknown origin is one of the most challenging clinical symptoms, with complex etiologies including infections, malignancies, and rheumatic immune diseases. Lymphoma is a common malignant tumor associated with fever of unknown origin, and its early diagnosis is often difficult because routine laboratory tests and imaging manifestations may fail to provide a definitive diagnosis. Here, we report the case of a patient with natural killer/T-cell lymphoma who primarily presented with long-term fever and pharyngodynia. The patient sought medical care at several hospitals and underwent multiple laryngoscopies and a biopsy of the tongue base. After >3 months from the time of initial presentation, the diagnosis was ultimately confirmed through the second biopsy of the tongue base. The case highlights the diagnostic challenges of lymphoma with atypical symptoms in the context of fever of unknown origin and underscores the role of infectious disease physicians in diagnosing noninfectious diseases related to fever of unknown origin.
Keywords
Introduction
Natural killer/T-cell lymphoma (NKTL) is a rare and highly aggressive subtype of non-Hodgkin lymphoma, which is predominantly found in Asian and South American populations.1–3 It is closely associated with Epstein–Barr virus (EBV) infection, and almost all patients with NKTL test positive for EBV DNA or EBV-encoded small RNA. 4 NKTL presents with diverse clinical manifestations and is primarily categorized into nasal and extranasal types. Nasal-type NKTL, accounting for approximately 80% of all NKTL cases, is localized to the nasopharynx and often presents with symptoms such as nasal obstruction, epistaxis, sore throat, and facial swelling, leading to frequent misdiagnosis as chronic rhinitis or sinusitis. The extranasal type, constituting 15%–20% of all NKTL cases, might involve the skin, gastrointestinal tract, lungs, testes, and other sites, manifesting as skin ulcers, abdominal pain, intestinal obstruction, or testicular swelling. 5 Additionally, patients commonly experience systemic symptoms such as fever, night sweats, and weight loss, which can lead to misdiagnosis as infectious or autoimmune diseases. This report describes the case of a patient with sore throat and fever who visited several hospitals over a period of 3 months, seeking medical care at various departments, such as the Departments of Otolaryngology, Tuberculosis, and Rheumatology. The patient underwent several laryngoscopies and a biopsy of the tongue base, all of which failed to establish a diagnosis. Upon admission to the Department of Infectious Diseases, further evaluation using positron emission tomography–computed tomography (PET–CT), a multidisciplinary discussion, and a repeat biopsy of the tongue base eventually confirmed the diagnosis of NKTL. This case highlights the diagnostic challenges of NKTL and emphasizes the importance of a multidisciplinary approach in identifying this rare and aggressive malignancy.
Case presentation
The patient was a woman in her early 60s, previously in good health, with no history of chronic diseases such as hypertension or diabetes. Approximately 3 months prior to admission, she developed a sore throat without any obvious triggering factors. There were no chills, fever, cough, sputum production, chest tightness, or chest pain. At that time, she did not pay much attention to the symptoms and did not seek treatment. Half a month later, the symptoms worsened, and the patient visited the Department of Otolaryngology in a comprehensive general hospital in Hangzhou. A video nasopharyngolaryngoscopy revealed dry and erosive mucosal lining in both nasal cavities with blood clots at the anterior end as well as pus and crusts in the middle and inferior nasal meatus, which were partially cleared. No obvious neoplasm was observed in the nasopharynx. There was follicular hyperplasia at the base of the tongue as well as ulceration with necrotic material on the laryngeal surface of the epiglottis. She was diagnosed with “epiglottic ulcer and chronic pharyngitis” and was treated with piperacillin–tazobactam as anti-infection therapy and methylprednisolone as anti-inflammatory therapy; however, the exact dosage was unknown. Her sore throat improved. Five days later, a repeat laryngoscopy showed follicular hyperplasia at the base of the tongue, ulceration with necrotic material on the laryngeal surface of the epiglottis, and congestion of the bilateral vocal cord mucosa with normal movement. Inflammation was considered to have been alleviated, and piperacillin–tazobactam was replaced by oral levofloxacin for 1 additional week before discontinuing treatment.
Two months prior to admission, the patient’s sore throat recurred, accompanied by fever with a maximum temperature of 39°C, which subsided after taking antipyretics. The fever mostly occurred in the afternoon to evening period, preceded by cold hands and feet, and was accompanied with mild cough. However, the patient did not receive any additional treatment. One month prior to admission, she visited another hospital, where physicians performed chest CT, revealing multiple areas of inflammation in the right lung. Therefore, physicians advised the patient to undergo bronchoscopy. However, bronchoscopy was difficult, and only significant congestion and edema of the epiglottis were observed, with pseudomembrane-like secretions and localized ulceration. “Epiglottic tuberculosis” was suspected, and the patient was advised to seek further treatment at a higher-level hospital. She then visited the tuberculosis department of another comprehensive general hospital. Laboratory tests including sputum smear, T-SPOT, tuberculosis DNA, mycobacterial identification and drug resistance testing were all negative, ruling out tuberculosis infection. A repeat laryngoscopy revealed follicular hyperplasia at the base of the tongue with ulcer-like new growth. A biopsy of the tongue base was performed, and targeted next-generation sequencing identified EBV (sequence count: 94,151) and Candida albicans (sequence count: 145). The pathological result of the tongue base biopsy indicated inflammatory tissue. Considering the inflammatory findings, the physician administered cefmetazole (2 g every 12 h) as anti-infection therapy. The patient’s fever and sore throat improved, and she was discharged.
After discharge, she experienced recurrent sore throat and fever. She returned to the first hospital for two repeat laryngoscopies, which showed results similar to those obtained previously. One week prior to admission, the patient visited the Department of Rheumatology and Immunology in the Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China. Blood tests showed the following results: white blood cell (WBC) count, 11.1 × 109/L (normal range: 4–10 × 109/L); neutrophil percentage, 84.4% (normal range: 50%–70%); C-reactive protein (CRP) level, 64.4 (normal: <10) mg/L; and ferritin level, 655 (normal range: 11–306.8) µg/L. Laboratory tests for anti-nuclear antibodies, anti-neutrophil cytoplasmic antibodies, immunoglobulins, and complement were unremarkable, which temporarily ruled out the possibility of rheumatologic or immunologic diseases. The patient was referred to the Department of Otolaryngology. A repeat laryngoscopy revealed multiple ulcers at the tongue base and throat, with ulcer-like neoplasm at the tongue base and absence of the epiglottis (Figure 1). Bacterial infection could not be ruled out, and the patient was treated with ceftriaxone (2 g every day) intravenously for 2 days before being admitted to the Department of Infectious Diseases of the Second Affiliated Hospital of Zhejiang University School of Medicine with the diagnosis of “sore throat; fever of unknown origin (FUO)” in January 2025.

Laryngoscopy results before admission: multiple ulcers were observed on the tongue base and pharynx, with an ulcer-like neoplasm visible on the tongue base, and the epiglottis was absent (the neoplasm is indicated by the red circle).
On the day of admission (Day 0), the patient still presented with sore throat and fever, with a maximum recorded body temperature of 39.1°C. Physical examination revealed a white coating on the tongue, multiple ulcers in the pharyngeal region, and an ulcer-like neoplasm at the base of the right side of the tongue (Figure 2). On auxiliary examination at admission, routine blood tests showed a WBC count of 6.2 × 109/L and hemoglobin level of 95 (normal: >110) g/L. The CRP level was 27.0 mg/L, and interleukin-6 level was 87.57 (normal: <7) pg/mL. The sedimentation rate was elevated at 27 (normal: <20) mm/h. The concentration of EBV DNA in the blood was 3.23 × 103 (normal: <1 × 103) copies/mL. No abnormalities were found in liver and kidney function tests. Chest CT showed a ground-glass nodule in the lateral segment of the right middle lobe, raising a suspicion of either an inflammatory nodule or a precursor glandular lesion. Prior to admission, the patient had received ceftriaxone as anti-infection therapy, which may have led to a decrease in the levels of inflammatory markers such as WBC count and CRP level. The infectious disease physician suspected that an infectious disease remained the primary consideration. After admission, treatment with cefmetazole (1 g every 8 h) was initiated as anti-infection therapy. Additionally, as EBV was detected in both the blood and tongue base tissue, ganciclovir (0.3 g every 12 h) was added as antiviral therapy. However, the patient continued to experience recurrent fever, and her sore throat showed no significant improvement.

Physical examination on Day 0: A white coating was visible on the tongue, with multiple ulcers in the pharynx. An ulcer-like neoplasm was observed at the base of the right side of the tongue (indicated by the red circle).
The infectious disease physicians believed that the antibiotic treatment was not sufficiently effective both before and after the patient’s admission. Multiple rheumatology and immunology-related indicators were within normal ranges, prompting the need to investigate potential tumor-related conditions. Consequently, the patient was advised to undergo PET–CT. The PET–CT results (Day 4) indicated localized thickening of the mucosa and increased glycol metabolism in the soft palate, left lateral wall of the oropharynx, base of the tongue, and left anterior wall of the hypopharynx, suggesting tumor or infection (Figure 3). Additionally, lung PET–CT revealed a ground-glass nodule in the lateral segment of the right middle lobe, most likely an inflammatory nodule or glandular precursor lesion; chronic bronchitis; and multiple fibroproliferative foci in both the lungs. The physicians believed that these pulmonary findings were unrelated to the cause of the patient’s fever. Given that the patient’s blood and biopsy tissues tested positive for EBV and that PET–CT showed increased glycol metabolism in the throat, the infectious disease physicians considered tumor-related disease as the most likely diagnosis. A multidisciplinary consultation was conducted involving the Departments of Infectious Diseases, Hematology, Otolaryngology, and Oral Surgery. The consensus of the multidisciplinary team was as follows: although the initial biopsy of the base of the tongue revealed inflammatory tissue, the presence of EBV still necessitates consideration of a neoplastic process. Thus, a repeat biopsy of the base of the tongue was deemed necessary. The oral and maxillofacial surgeon performed a local anesthesia biopsy of the right tongue mass and adjacent tissue flap formation on Day 6 after admission. The pathological examination revealed that the dermis and intermuscular tissues showed sheets of cells with twisted nuclei, prominent nucleoli, and visible mitotic figures (Figure 4). Immunohistochemistry results (A1-01, Slide 1) showed the following results: CK-PAN(−), CD45(LCA)(+), CD20 (scattered individual positive cells), CD79a (scattered individual positive cells), CD3(+), CD5 (focally positive), EBER-ISH(+), Ki-67(70%), S100(−), HMB45(−), Melan-A(−), vimentin(+), CAM5.2(−), CD2(+), CD4 (partially positive), CD8 (scattered positive cells), CD56(−), granzyme B(+), TIA-1(+), ALK(−), CD30(80%+), CD19(−), CD10(−), PD-1(−), Bcl-6(+), and p53 (wild-type expression pattern). Combined with immunohistochemistry results, the findings were consistent with those of extranodal NKTL. The antibiotic and antiviral medications were discontinued, and the patient was transferred to the Department of Hematology for further examination and treatment (Day 14 after admission). The lymphoma did not show any involvement of the bone marrow. Enhanced magnetic resonance imaging (MRI) of the nasopharynx revealed diffuse thickening and abnormal signals in the soft palate, base of the tongue, left oropharynx, and lateral wall of the hypopharynx. After ruling out contraindications, brentuximab vedotin (BV) + gemcitabine–oxaliplatin (GemOx) chemotherapy regimen, consisting of 100 mg BV, 1 g gemcitabine, and 100 mg oxaliplatin, was initiated on Day 16 and administered every 21 days. The symptoms of fever and pharyngodynia improved, and the patient was subsequently discharged. Follow-up was conducted in the hematology department. A repeat enhanced MRI of the nasopharynx after 20 days post-discharge showed improvement in the diffuse thickening of the soft tissues, and the patient continued to undergo regular chemotherapy sessions. A timeline of investigations and interventions is provided in Figure 5.
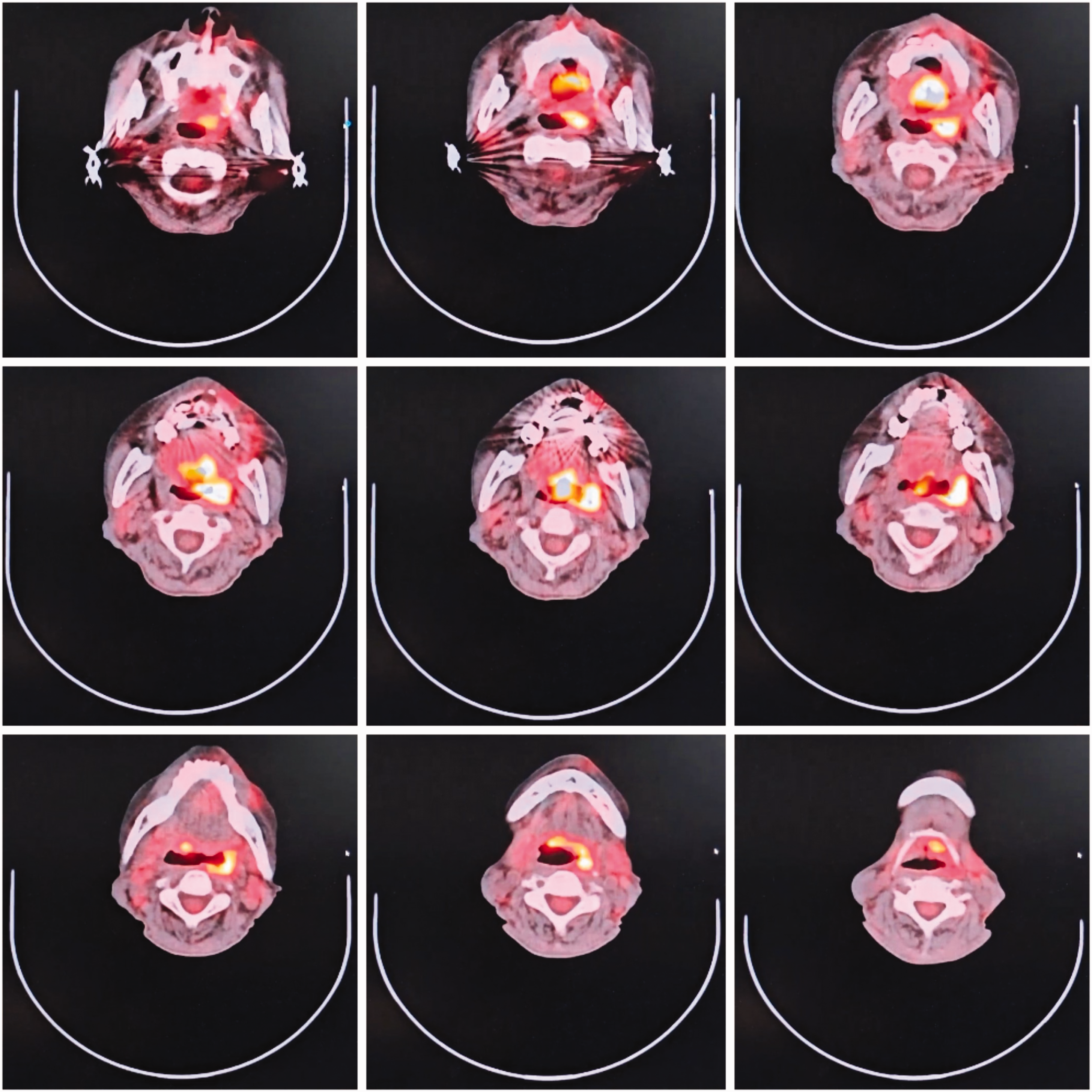
The PET–CT image on Day 4 showing localized thickening of the mucosa and increased glycol metabolism in the soft palate, left lateral wall of the oropharynx, base of the tongue, and left anterior wall of the hypopharynx. PET–CT: positron emission tomography–computed tomography.
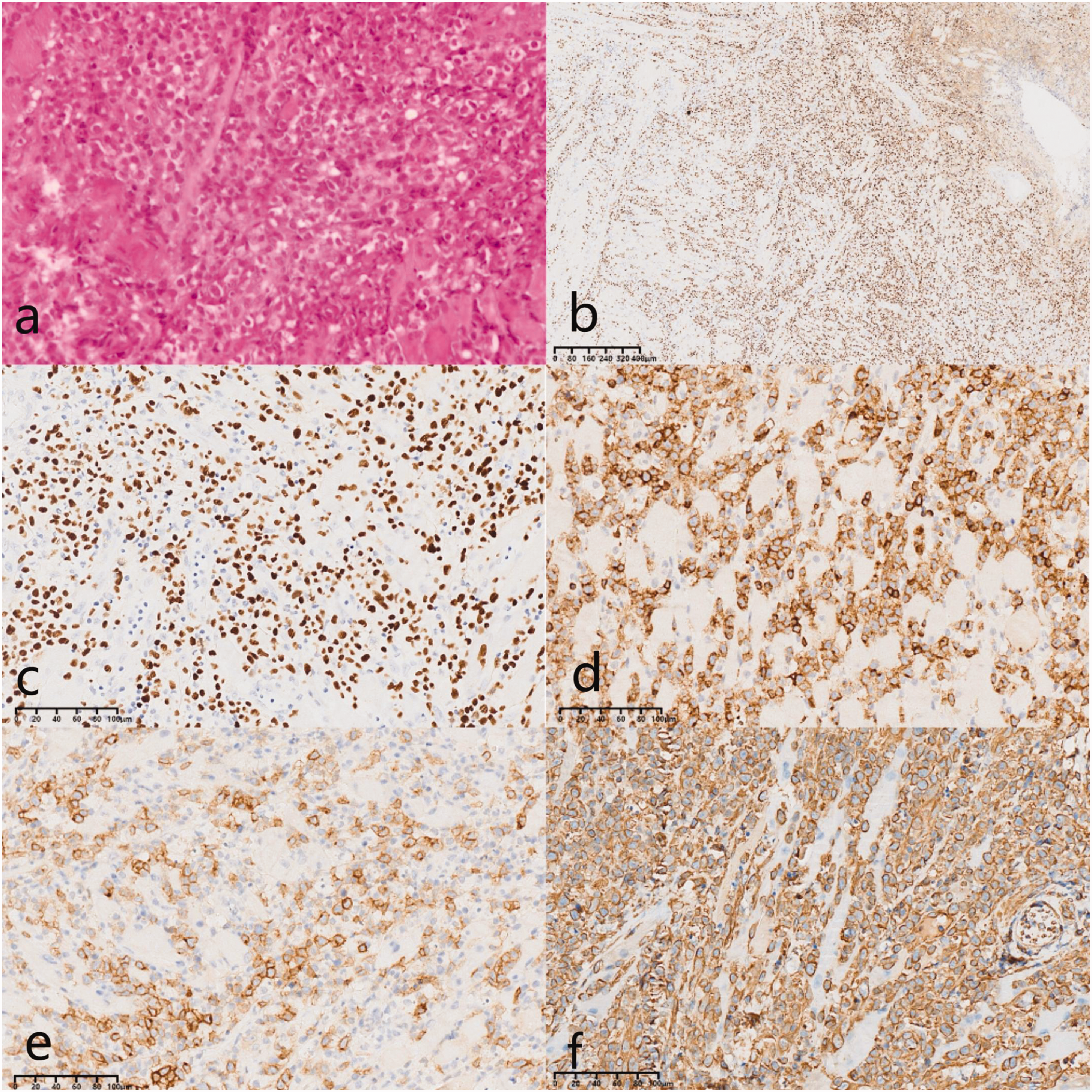
Pathology of tongue base biopsy on Day 6. (a) Right tongue base mass: sheets of convoluted cells with prominent nucleoli and visible mitotic figures were observed in the dermis and intermuscular tissue; (b) IHC image (EBER-ISH, 4.00×); (c) IHC image (EBER-ISH, 20.00×); (d) IHC image (CD2, 20.00×); (e) IHC image (CD30, 20.00×) and (f) IHC image (vimentin, 20.00×). IHC: immunohistochemistry.
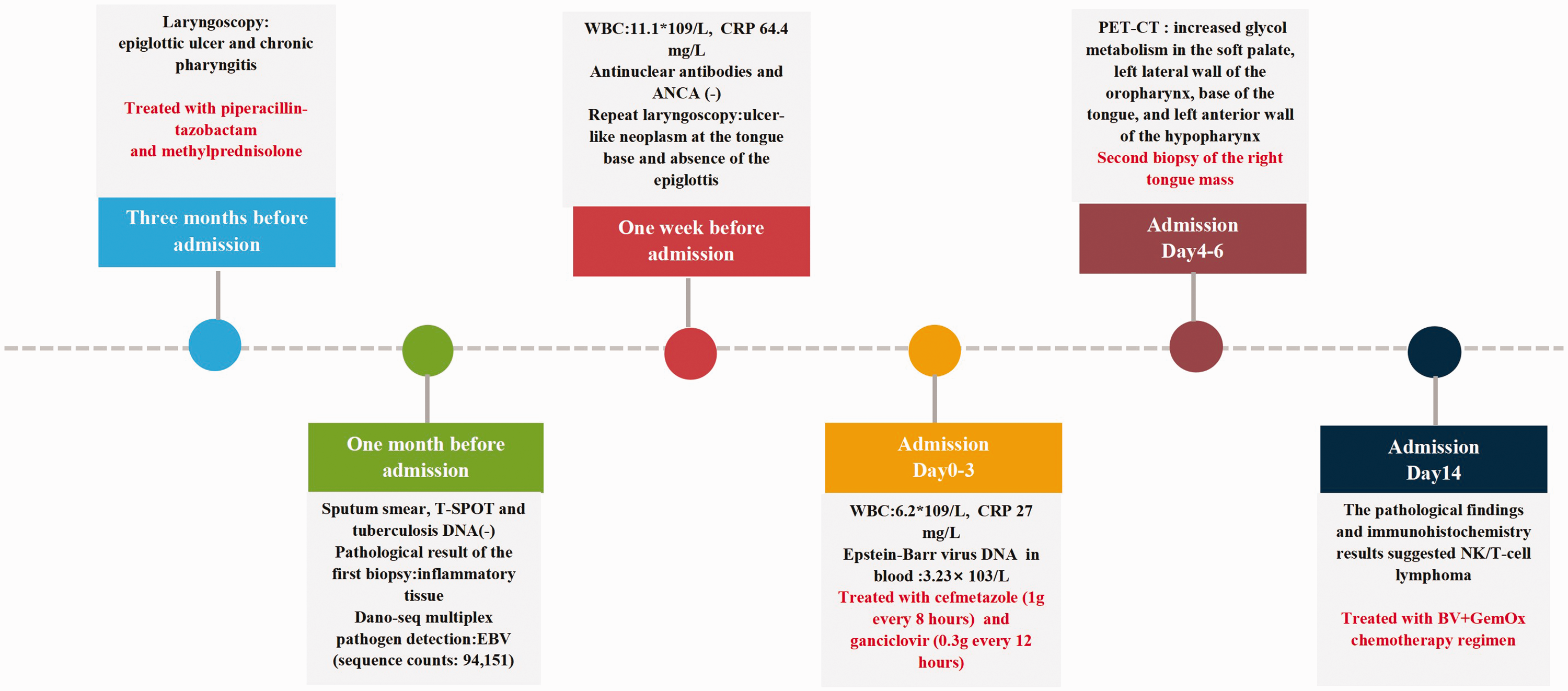
Timeline of investigations and interventions.
Discussion
FUO refers to a clinical syndrome characterized by a persistent body temperature higher than 38.3°C for more than 3 weeks, with the underlying cause remaining unclear after at least 1 week of thorough investigation. 6 This case is a classic example of FUO, presenting primarily with sore throat and fever. The patient sought multiple consultations in the Departments of Otolaryngology, Tuberculosis, and Rheumatology and Immunology; however, a definitive diagnosis remained elusive. A diagnostic and management algorithm for FUO was proposed in the literature.7,8 During the patient’s treatment at the external hospital, the physicians completed a thorough medical history inquiry, physical examination, laboratory tests, and imaging studies. They also performed a biopsy of the suspected area. The initial diagnostic and treatment process was generally in line with standard procedures. However, the biopsy results only indicated inflammatory tissue, and a definitive diagnosis could not be determined. Following the recommended algorithm, the patient’s clinical presentation was reevaluated, and the medical history was reviewed after admission to the Department of Infectious Disease. A blood EBV test was also performed, and fluorodeoxyglucose PET–CT was completed. After obtaining new evidence, including a positive blood EBV test and increased glucose metabolism at the base of the tongue on FDG PET–CT, a multidisciplinary discussion was conducted, and the decision to perform a second biopsy was ultimately taken. This decision involved significant challenges, wherein the attending physicians demonstrated not only their diagnostic and treatment capabilities but also their ability to collaborate effectively with other relevant departments and communicate clearly with the patient and their family, given the substantial risk of the second biopsy, which may yield negative results. The second biopsy achieved diagnostically conclusive results. We suspected that the initial biopsy might have only sampled superficial tissues, thus failing to obtain lymphoma-involved tissue. The second biopsy was performed after PET–CT, which provided the biopsy physician with clearer anatomical localization. Additionally, prior to the second biopsy, a multidisciplinary discussion was conducted, during which the likelihood of malignancy was emphasized. This enhanced the purposefulness and precision of the biopsy procedure for the operating physician.
FUO is complex and primarily includes infections, malignancies, rheumatic and immune diseases, and other rare etiologies. Infectious etiologies have consistently remained the leading cause of FUO. 9 However, their proportion among FUO cases has gradually declined in recent years, which may also be attributed to the improved and more rapid diagnostic capabilities for many infectious diseases. According to the literature, neoplastic diseases account for approximately 2%–25% of the causes of FUO. 7 Lymphoma is one of the most common causes of neoplastic fever.10,11 The early symptoms of lymphoma are often nonspecific, such as fever, nasal congestion, sore throat, and lymphadenopathy, which resemble those associated with infectious diseases or autoimmune diseases. The imaging manifestations of lymphoma may also overlap with those of other diseases, leading to a misdiagnosis. Although PET–CT has high sensitivity for lymphoma, 12 it is not routinely available in all medical institutions, and the cost of this test is relatively high. The diagnosis of lymphoma relies on pathological biopsy, but delays in diagnosis can occur due to inappropriate biopsy site selection, atypical pathological presentation, or incomplete immunohistochemistry. Certain lymphoma subtypes such as NKTL and angioimmunoblastic T-cell lymphoma are relatively rare, and insufficient awareness among clinicians can lead to missed or incorrect diagnoses, potentially resulting in delayed or inappropriate treatment.
EBV is recognized as a globally prevalent DNA virus. A majority of EBV-infected individuals exhibit no significant symptoms, while a minority may present with infectious mononucleosis. 13 This virus is also associated with lymphoproliferative lesions and malignant lymphomas. 14 This patient’s EBV DNA concentration in the blood was 3.23 × 103 copies/mL. In general, in patients with infectious mononucleosis, EBV is in the active replication phase, and the EBV DNA load in the blood significantly increases (usually >104 copies/mL). In patients with latent infection, the EBV DNA load in the blood gradually decreases (usually <103 copies/mL). In patients with nasal-type NKTL, the virus may be accompanied with lytic replication of EBV, resulting in higher local viral loads. Certainly, we still need to perform differential diagnosis for various EBV-associated lymphomas, which typically requires pathological analysis. Nasal-type NKTL is rare but highly aggressive. Compared with other lymphoma subtypes, it is characterized by extensive necrosis and angio-invasion, primarily manifesting at extranodal sites with a predilection for the upper aero-digestive tract. 14
A comprehensive knowledge base, an open diagnostic mindset, and multidisciplinary collaboration are key to improving the diagnostic accuracy and treatment effectiveness of FUO. Infectious disease physicians are the primary clinicians managing patients with FUO and are responsible for conducting a thorough evaluation, including medical history collection, physical examination, and laboratory tests. Therefore, infectious disease physicians must be familiar with the various conditions associated with FUO. Additionally, close collaboration with other departments, such as Departments of Oncology, Rheumatology, and Hematology, is essential for developing diagnostic and treatment plans, thereby enhancing diagnostic accuracy and treatment efficacy.
Conclusion
Effective management of FUO requires infectious disease physicians to possess comprehensive diagnostic skills, an understanding of both infectious and noninfectious causes, and the ability to collaborate closely with multidisciplinary teams to ensure accurate diagnosis and optimal treatment.
Footnotes
Acknowledgements
None.
Authors’ contributions
L.P. and Y.Z. collected the data and drafted the manuscript. H.Z. and X.W. revised the manuscript. All authors have read and approved the final manuscript.
Consent for publication
The patient provided written informed consent for any identifiable photographs and/or clinical information to be used in this study. The reporting of this study conforms to the Case Report (CARE) guidelines. 15 The patient also consented to all the treatments described in this case report. We have de-identified all patient details.
Data availability statement
Data will be made available on request.
Declaration of conflicting interests
The authors declare that they have no conflicts of interest.
Ethics approval
This work was approved by the Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (ethics approval no. (2025) No. (0426)).
Funding
This work was supported by the National Natural Science Foundation of China (No. 82200052).