
Abstract
Depression, dementia, and delirium comprise the “3 Ds” of mental illness diagnoses in the older population. Depression is a common condition. Older adults may passively deal with depression, may not adhere to their prescribed drug schedules, and may be prone to unexpected side effects. A 70-year-old man with depression was brought by his family to the clinic with a 2-month history of depressed mood and poor drug compliance. After being diagnosed with depression, mirtazapine treatment was started. The following day, his family members suspected that the use of psychiatric drugs had caused acute urinary retention; hence, they brought him back to the emergency department. The emergency physician diagnosed the patient with benign prostatic hyperplasia and admitted him to the psychiatric ward after urinary catheterization. This case illustrates the effects of mirtazapine on urinary function in older individuals, particularly those with a history of benign prostatic hyperplasia. Although low-dose short-acting benzodiazepines and non-benzodiazepine hypnotics (Z-drugs) have been used to reduce the anticholinergic cognitive burden, mirtazapine inevitably induces acute urinary retention in older males with benign prostatic hyperplasia. Thus, the possibility of acute urinary retention caused by mirtazapine, particularly in patients with benign prostatic hyperplasia, cannot be ignored.
Introduction
Geriatric depression, dementia, and delirium comprise the so-called 3 Ds of mental illness diagnoses in the older population, with the fourth diagnosis being delusions. Older individuals with depression passively deal with the condition and may not take prescribed drugs regularly. Moreover, the vulnerability and fragility of this population increase the risk of unexpected drug-related side effects. 1 Mirtazapine is an antidepressant that is widely used to treat depression in older people owing to its sedative and orexigenic effects. Tools such as anticholinergic calculators are frequently used to estimate the accumulation of these drugs. Importantly, lithium use is associated with an increased risk of reduced urinary concentration ability, hypothyroidism, and hyperparathyroidism. 2
Acute urinary retention (AUR) is defined as the sudden inability to urinate or empty the bladder. Chronic urinary retention (UR), which refers to gradual enlargement of the bladder over a prolonged period, has been reported in older men.3–4 AUR occurs more commonly in older men with a history of benign prostatic hyperplasia (BPH). 5 A study showed that 10% of men aged >70 years and 33% of men aged >80 years experience AUR. 6 This condition is relatively rare in women, with an annual incidence of 1 in 100,000 and a male-to-female ratio of 13:1. 7 The most common drugs that cause UR are anticholinergic and sympathomimetic agents. 8 Approximately 10% of AUR cases are attributable to concomitant medication use, with anticholinergic drugs such as antidepressants, antipsychotics, and benzodiazepines being the most common medication, followed by opioids and anesthetics, α-adrenoceptor agonists, detrusor relaxants, and calcium channel antagonists. 3 The anticholinergic activity of multiple drugs is measured using the anticholinergic cognitive burden (ACB) scale. The use of the ACB scale is necessary for reducing the use of potentially inappropriate medications in older patients.
Sympathetic nerve stimulation increases urine storage capacity (inhibiting urination), whereas parasympathetic nerve stimulation inhibits urine storage (promoting urination). In addition, the central micturition pathway is regulated by serotonin and dopamine. Serotonin activates sympathetic nerves and inhibits the parasympathetic pathway to enhance urine storage, thereby inhibiting urination. Dopamine can inhibit or promote urination depending on the receptors on which it acts. D1 receptors inhibit bladder contraction and enhance urine storage, whereas D2 receptors promote urination. 3 Particular attention has been given to the side effects of anticholinergic and adrenergic antagonists such as clozapine. 9 The anticholinergic activity of several drugs, such as low-potency typical antipsychotics (e.g. chlorpromazine and the “pines” of atypical antipsychotics), can cause UR.
Antipsychotics are mainly metabolized in the liver via the cytochrome p450 pathway. The use of selective serotonin reuptake inhibitors can increase the serum levels of antipsychotic drugs and the incidence of side effects. 3 In addition, serotonin–norepinephrine reuptake inhibitors can induce UR by stimulating α1-adrenoreceptors. 10 The use of haloperidol combined with fluoxetine, sertraline, venlafaxine, and other antidepressants is also related to UR, 11 particularly in patients prescribed benzodiazepines and antiparkinsonian agents (e.g. biperiden and trihexyphenidyl), because of extrapyramidal side effects, which also increase the probability of UR.
Case report
This study conformed to the Case Report (CARE) guidelines. 12 The participant provided informed consent for publication of this case report, and his anonymity was preserved.
A 70-year-old man was initially brought to the clinic by his daughter (on 2 March 2020) with a 2-month history of depressed mood, loss of interest, fatigue, poor appetite, suicidal ideation, and poor drug compliance. The first mood episode occurred when the patient was 65 years old and manifested as depression owing to decreased income. The patient was followed up at a psychiatric clinic three times. The precipitating factor for this major depressive episode was his wife’s diagnosis of metastatic cancer in 2019.
At the first visit, the patient was prescribed mirtazapine for treating melancholic depression (Figure 1). However, the following day, he presented to the emergency room (with his daughter) with AUR. After undergoing catheterization in the emergency department, he was admitted to the psychiatric ward and received an immediate consultation with the urology department for a urethral injury with hematuria; he was prescribed tamsulosin (0.4 mg/day) and bethanechol (50 mg/day). During hospitalization, the patient was switched to escitalopram (10 mg/day) for depression, short-acting benzodiazepines for anxiety, and non-anticholinergic zopiclone for difficulty falling asleep. Several days later, his mood improved and he was discharged from the hospital with an indwelling urinary catheter.
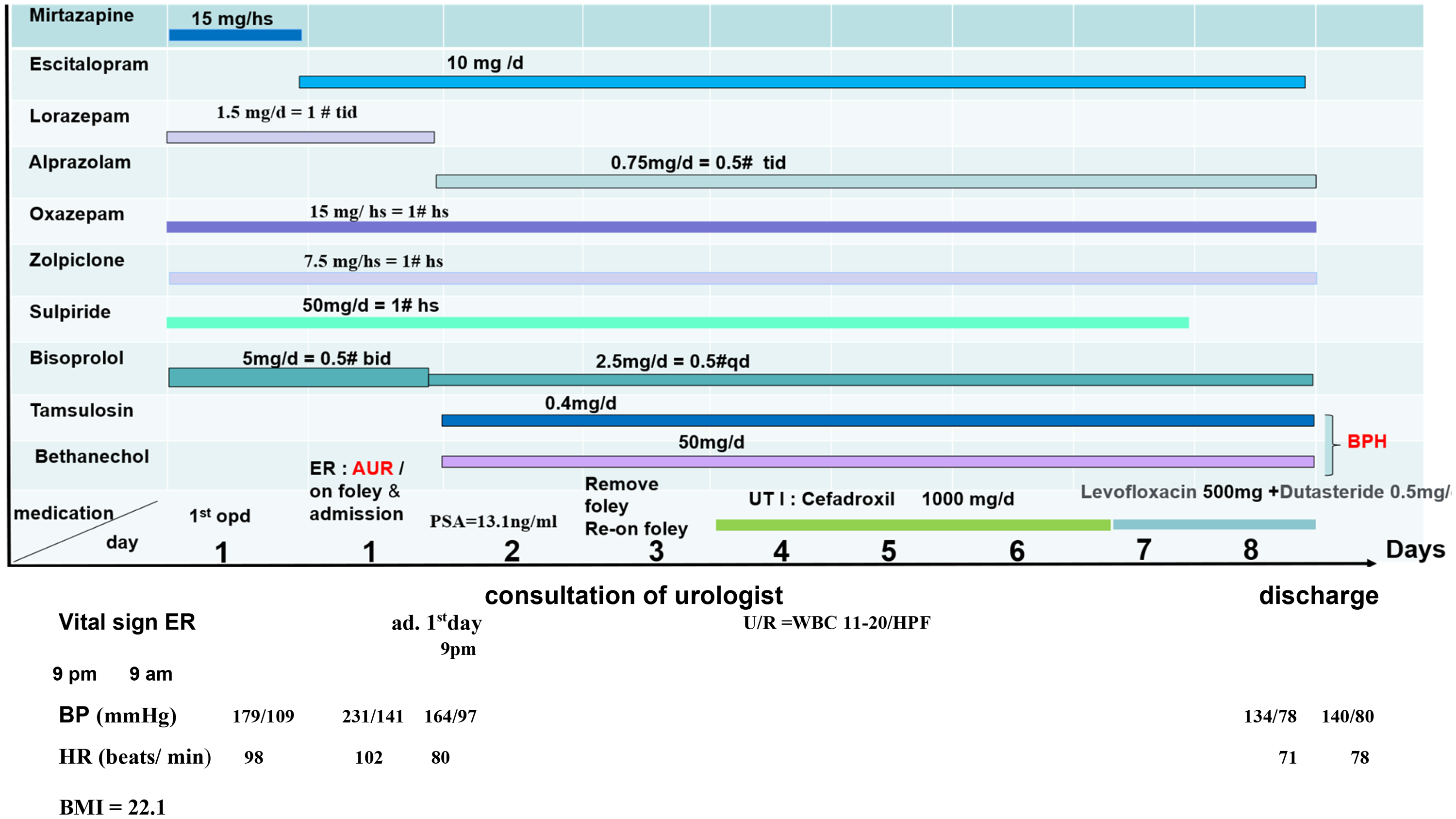
Patient’s clinical situation and management in Taichung Hospital, Taiwan. Note: The patient visited the emergency department the day after the outpatient visit. Because of difficulty urinating, he was hospitalized after on foley with suspicion of BPH. AUR: acute urinary retention; ad: admission; bid: twice a day; BMI: body mass index; BP: blood pressure; BPH: benign prostate hyperplasia; HR: heart rate; hs: at bed-time; OPD: outpatient department; PSA: prostate-specific antigen; tid: three times a day; UTI: unitary tract infection; U/R: urine routine; qd: once a day; hs: at bed-time (before sleep).
Mirtazapine is a unique antidepressant and is known for its role as a presynaptic α2 antagonist, its enhanced effects on the noradrenergic and serotonergic systems, and its potent antagonist effects on postsynaptic 5-HT2 and 5-HT3 receptors. These effects increase noradrenergic activity, specifically serotonergic activity, particularly at the 5-HT1A receptors. 13 Norepinephrine (NE) stimulates presynaptic α2 autoreceptors (gatekeepers) to inhibit its own release. Mirtazapine blocks not only the α2 receptor but also 5HT2A, 5HT2C, 5HT3, and H1 histamine receptors. 9 By increasing NE and serotonin activity, mirtazapine can cause UR, especially in older men with BPH.8,14 Mirtazapine binds to the H1 receptor as an antagonist, exerting antihistamine effects and indirectly affecting bladder contraction.15–16 A series of case studies on mirtazapine-induced UR is warranted to strengthen this evidence. However, the single case study presented here cannot rule out the impact of over-the-counter antihistamines or undiagnosed bladder dysfunction.
Conclusions
Escitalopram is recommended as the first-line treatment for older patients with depression; its single effect on the mechanism of serotonin and drug interactions may prevent unexpected sequelae of AUR. To avoid anticholinergic side effects and negative effects on memory, short-acting and low-dose tranquilizers have been used to relieve anxiety, along with Z-drugs (zopiclone and zolpidem) for treating the symptoms of difficulty in falling asleep and early awakening.
Footnotes
Acknowledgements
None.
Author contributions
Lee-Hou Tsai treated the patient. Lee-Hou Tsai and Jeng-Wen Lin wrote the manuscript. Maw-Sheng Lee and Yennun Huang revised the manuscript. All the authors contributed to and approved the final version of the manuscript.
Consent for publication
The participant provided informed consent for publication of this case report.
Data availability statement
All data are available in the article.
Declaration of conflicting interest
The authors declare no conflict of interest regarding the publication of this study.
Funding
This work was supported by Academia Sinica, Taiwan, under Grant (No. SV-114-1-14).