
Abstract
Objective
This study aimed to use computed tomography perfusion imaging to investigate the correlation between blood pressure at onset and prognosis in patients with acute ischemic stroke and collateral circulation. It also aimed to verify the value of using blood pressure levels along with computed tomography perfusion imaging for predicting the prognosis of patients with acute ischemic stroke.
Methods
This retrospective study included 237 patients with acute ischemic stroke. Patients were divided into good prognosis group and poor prognosis group based on the National Institute of Health Stroke Scale scores after clinical discharge. All patients underwent computed tomography perfusion imaging, and image post-processing was performed. Comparison of clinical characteristics, blood pressure levels, and computed tomography perfusion imaging measurements was performed between the two groups. Univariate and multivariate logistic regression analyses and receiver operating characteristic curve analyses were performed for the collected clinical variables.
Results
Of the 237 recruited patients (aged 67.54 ± 7.75 years; 103 males), 151 had a good prognosis. There were no significant differences in age, systolic blood pressure levels, and alcohol consumption pattern as well as the presence of diabetes, myocardial infarction, coronary atherosclerotic disease, and atrial fibrillation between the good and poor prognosis groups (P > 0.05). There were significant differences in terms of sex distribution and diastolic blood pressure levels between the two groups (P = 0.028 and P < 0.05, respectively). Binary logistic regression analysis revealed that patient prognosis was positively correlated with diastolic blood pressure levels, cerebral blood flow <30%, and mismatch ratio (P < 0.05). Partial correlation analysis revealed a positive correlation between blood pressure levels and cerebral blood flow <30% and mismatch ratio (P < 0.05). Receiver operating characteristic curve analysis revealed that the areas under the blood pressure, cerebral blood flow, mismatch, and combined prognostic value curves were 0.657, 0.683, 0.693, and 0.711, respectively. The sensitivity and specificity were 69.8%, 46.5%, 46.5%, and 57.4% and 60.9%, 90.1%, 95.4%, and 92.1%, respectively.
Conclusion
There is a correlation between blood pressure levels and prognosis in patients with acute ischemic stroke; however, blood pressure does not affect prognosis by influencing the collateral circulation status in the ischemic area. The combined use of blood pressure levels, cerebral blood flow <30%, and mismatch ratio can improve the prognosis of patients with acute ischemic stroke.
Keywords
Introduction
According to global research on the burden of diseases, injuries, and risk factors, stroke is the second leading cause of death and third leading cause of disability in the world. 1 China has the highest prevalence of stroke in the world. 2 Hypertension is one of the main risk factors of stroke.1,3 Research conducted on the development of stroke has focused on elevated blood pressure (BP) levels. A nationwide study conducted in the United States found that 60% of stroke patients experienced an increase in their BP level within 24 h before the onset of acute ischemic stroke (AIS), indicating an acute hypertension response. 4 However, BP characteristics with respect to prognosis in patients with AIS remain unclear. In previous studies, some scholars have suggested that elevated BP levels in patients with AIS are associated with poor prognosis, while other studies have concluded that the hypertension response in patients with AIS has limited prognostic value and that even sustained BP increases may indicate better clinical outcomes.5,6 The mechanism by which BP affects the clinical outcomes of patients with AIS lacks specific validation.
Hong et al. found that an increase in baseline BP in patients with AIS and reperfusion resulted in a better presence of ischemic penumbra and slower infarct growth, leading to better clinical outcomes. 7 The central area of ischemic cerebral infarction is the core infarction area where brain tissue damage is irreversible. Even after the blocked artery is reopened, neurological function cannot be restored. The functional outcome of the ischemic penumbra in the brain tissue surrounding the infarcted core area is a dynamic state. 8 The infarcted core area and ischemic penumbra are correlated with clinical outcomes.
The establishment of collateral circulation is a key factor in the recovery of penumbra function in patients with AIS. Higher BP may increase collateral perfusion, maintain ischemic penumbra, and minimize the final infarcted area, potentially worsening patient outcomes. In previous reports on collateral circulation and BP, Hong et al. found that higher baseline BP levels were associated with better collateral blood flow. 7 Lima et al. found that patients with AIS have higher systolic blood pressure (SBP); this could translate into less collateral circulation; however, it was not related to clinical outcomes. 9 Wufuer et al. demonstrated a correlation between the initial BP levels at the onset of AIS and collateral circulation, as evaluated using the American Society for Interventional Therapy Neuroradiology/Society for Interventional Radiology (ASITN/SIR) collateral flow classification system. 10
Computed tomography perfusion imaging (CTPI) and post-processing software have been widely used to calculate cerebral blood flow (CBF) and time to maximum (Tmax) for the evaluation of the cerebral ischemia status. These tools have been widely used to measure infarct core volume (ICV) and penumbra volume (PV). 11 Fast processing of ischemic stroke (F-STROKE) is a fully automated processing software that can segment and label large blood vessels, brain parenchyma, and cerebrospinal fluid based on their time–intensity curves and label the ischemic core or semi-dark area on the time–intensity curve of the brain parenchyma. In addition to the ability to automatically generate ICVs and PVs, F-STROKE provides an additional density map and specific density values for the lateral branches. 12 At present, no correlation has been established between collateral circulation and ischemic penumbra in studies on the correlation between BP and prognosis in patients with AIS. It is worth exploring whether BP before treatment in patients with AIS is related to collateral circulation and ischemic penumbra and whether it affects clinical outcomes. Therefore, this study aimed to investigate whether baseline BP and clinical prognosis in AIS patients are related to the establishment of collateral circulation, as predicted by software. Furthermore, we aimed to determine the predictive value of CTPI combined with BP for adverse clinical outcomes in patients with AIS.
Materials and methods
Patients
Patients who underwent CTPI in the computed tomography (CT) room were included in this study.
The specific inclusion criteria were as follows: (a) clear diagnosis of AIS13,14 as per the following diagnostic criteria: 1) acute onset, 2) focal neurological deficits or a few cases of comprehensive neurological deficits, 3) imaging showing a responsible lesion area or one of the symptoms and signs that persist for more than 24 h, 4) exclusion of other nonvascular causes, and 5) head CT or magnetic resonance imaging excluding cerebral hemorrhage; (b) age >18 years; and (c) improved CT results. Patients with brain injury; those with other important organ diseases such as those of the heart, liver, or kidney or malignant tumor diseases; or those with incomplete clinical data were excluded.
Clinical assessment
In total, 237 patients with acute ischemic cerebral infarction were enrolled after screening them as per the inclusion and exclusion criteria. All cases were retrospectively analyzed and numbered to protect patient privacy. Patients were discharged from the hospital with a National Institute of Health Stroke Scale (NIHSS) score, defined as a short-term outcome. An NIHSS score ≤4 was considered to indicate good prognosis, while a score >4 indicated poor prognosis.
This study included complete data regarding the patients’ clinical characteristics and follow-up information, including age, sex, SBP, diastolic blood pressure (DBP), mean arterial pressure (MAP), smoking habit, and alcohol consumption pattern as well as the presence of diabetes, myocardial infarction, coronary atherosclerotic disease, atrial fibrillation, and hypertension.
CT
A Siemens Healthcare GmbH SOMATOM Force 64 row CT scanner was used in this study. Spiral scanning was adopted for the flat scan, with a tube voltage of 70 kV and a tube current of 200 mA. The cradle-bed mode with variable pitch is an adaptive 4D spiral mode with a rotation time of 0.25 s, layer thickness of 0.5 mm, and detector width of 40 mm. An intravenous pressure syringe was used to inject 50 mL of soluble nonionic contrast agent (iodine alcohol injection) and 30 mL of physiological saline through the right elbow median vein at a rate of 4.0–5.0 mL/s.
Image post-processing
CTPI data were generated by fully automatic processing using F-STROKE software. Large vessels, brain parenchyma, bone, and cerebrospinal fluid were segmented according to the time–intensity curve, and the ischemic core area or semi-dark area was labeled on the time–intensity curve of the brain parenchyma, which avoided the mislabeling of low-signal areas such as arachnoid cysts. CBF values, Tmax values, mismatch ratio, collateral vessel density, and Alberta Stroke Program Early Computed Tomography Score (ASPECTS) were calculated. CBF <30% was defined as ICV, and Tmax >6 s was defined as ischemic semi-dark band volume.
BP measurement methods
Patients’ BP levels were measured as soon as possible after admission. At rest, the patient was made to sit or asked to be in the supine position, with their bare upper arm straightened and mildly abducted and the arm maintained at the same level as the heart. The BP cuff was placed over the elbow socket, and the body piece of the stethoscope was placed on the surface of the brachial artery for auscultation. When the stethoscope detects the first pulse sound, the mercury column indicates the SBP, and when the sound disappears, the mercury column indicates the DBP. After the measurement was completed, the air in the cuff was drained, and the cuff was removed; the measurement was repeated thrice, and the average value was recorded.
Statistical analyses
We used the Statistical Package for Social Sciences (SPSS27.0) medical statistical software to process data for statistical analysis. Normally distributed continuous variables were expressed as mean ± standard deviation, while non-normally distributed continuous variables were expressed as median and interquartile ranges (1st quartile, 3rd quartile) M (Q25, Q75). Normally distributed continuous variables were compared between the two groups using independent samples t-test. The Mann–Whitney U test was used as a nonparametric test for continuous variables that did not conform to a normal distribution. Count data were expressed as frequency (%), and comparisons between the two groups were made using the chi-square test. The correlation between patients’ prognostic outcomes and the results of BP and CTPI processing was analyzed using binary logistic regression (independent variables with P < 0.05 were screened using univariate analysis and included in the multivariate analysis). Partial correlation analysis was performed for BP and CTPI measurements after correcting for age, sex, smoking habit, and alcohol consumption pattern as well as the presence of diabetes, myocardial infarction, coronary atherosclerosis disease, atrial fibrillation, hypertension, and previous stroke. The effects of DBP, CBF <30%, mismatch ratio, and their combinations on patient prognosis were analyzed using receiver operating characteristic (ROC) curves for the relevant variables according to the multifactorial results (0.6–0.9 indicated good predictive value and >0.9 indicated excellent predictive value). Statistical significance was set at P < 0.05.
Results
Clinical characteristics
Overall, 237 cases of acute ischemic cerebral infarction were obtained after screening as per the inclusion and exclusion criteria. Among them, 151 had a good prognosis and 86 had a poor prognosis. Among them, 173 were males and 64 were females; the patient age range was 38–86 years, with a mean age of 67.54 ± 7.75 years. There were no significant differences in the clinical data between the two groups in terms of age, smoking habit, and alcohol consumption pattern as well as the presence of diabetes, myocardial infarction, coronary atherosclerotic disease, and atrial fibrillation (P > 0.05). In contrast, the SBP (P = 0.012), SBP (P < 0.001), and MAP (P = 0.001) were significantly higher in the poor prognosis group than in the good prognosis group (Table 1). The AIS outcome was associated with whether the patients had hypertension (P = 0.001) or had experienced a stroke (P < 0.001) before admission. There was a difference in the right ASPECTS between the two groups of patients with different outcomes (P < 0.001) (Table 1).
Baseline demographic and clinical characteristics.

SBP: systolic blood pressure: DBP: diastolic blood pressure; MAP: mean arterial pressure; ASPECTS: Alberta Stroke Program Early Computed Tomography Score; M: median; Q1: first quartile; Q3: third quartile.
Univariate and multivariate logistic regression analyses of patient prognosis, BP, and CTPI management results
Data on sex, SBP, DBP, MAP, hypertension, stroke, and CTPI processing were subjected to a univariate logistic regression analysis. The results showed that there was a significant correlation between sex, DBP, MAP, hypertension, stroke, CBF <30%, Tmax >6 s, Tmax >4 s, mismatch ratio, mismatch volume, and patient outcomes (P < 0.05). In multifactorial logistic regression analysis, DBP (odds ratio (OR) = 0.076, 95% confidence interval (CI) = 1.105–1.058, P = 0.035), hypertension (OR = −0.917, 95% CI = 0.196–0.817, P = 0.012), stroke (OR = 0.985, 95% CI = 1.270–5.642, P = 0.010), CBF <30% (OR = 0.117, 95% CI = 1.007–1.255, P = 0.037), and mismatch ratio (OR = 0.069, 95% CI = 1.007–1.041, P = 0.030) were independent risk factors for the prediction of patient outcomes (Table 2).
Univariate and multivariate logistic regression analyses of patient prognosis, blood pressure, and CTPI management results.
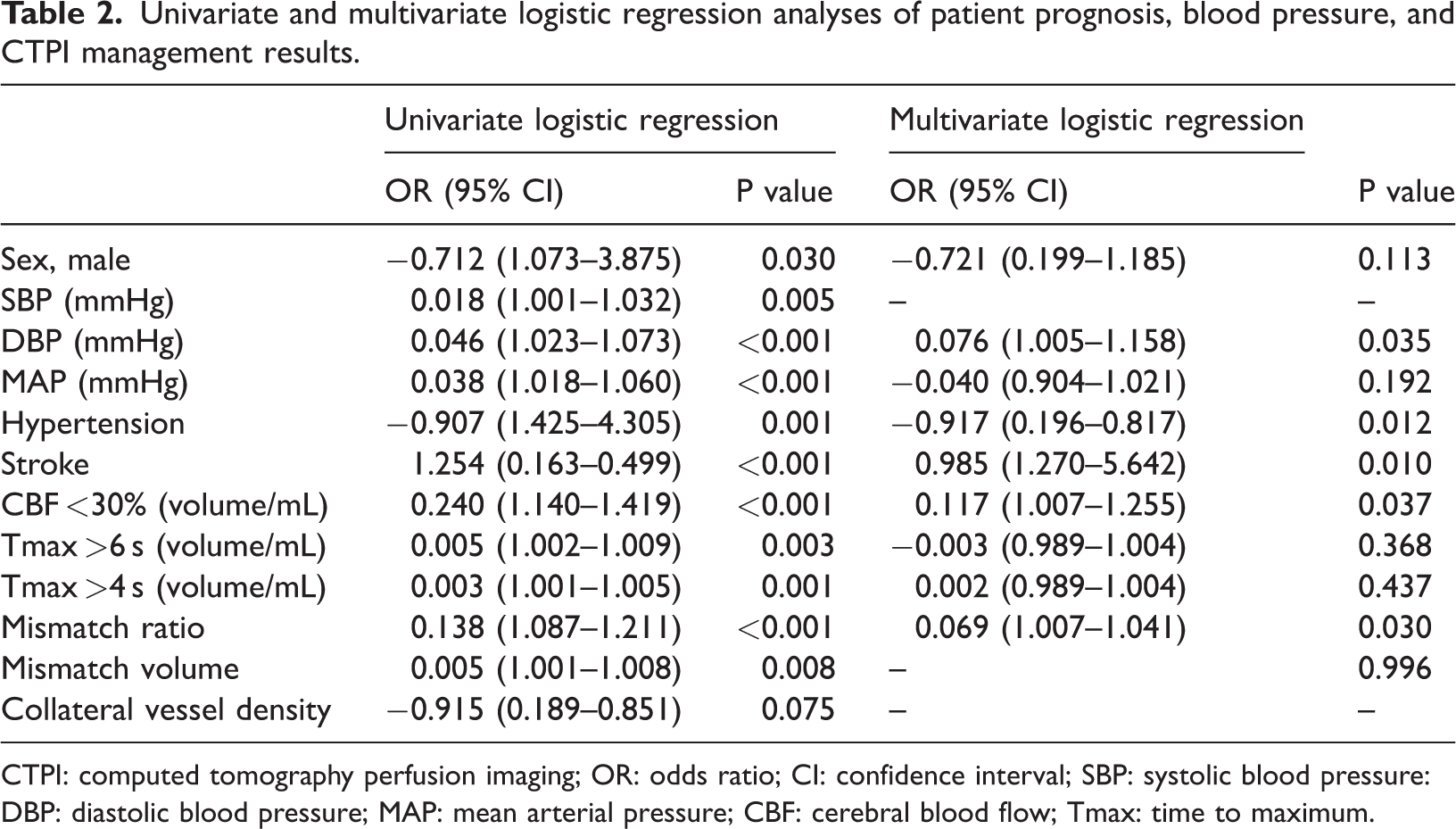
CTPI: computed tomography perfusion imaging; OR: odds ratio; CI: confidence interval; SBP: systolic blood pressure: DBP: diastolic blood pressure; MAP: mean arterial pressure; CBF: cerebral blood flow; Tmax: time to maximum.
Bias correlation analysis of DBP and CTPI processing results
A skewed correlation analysis showed that the patients’ BP was positively correlated with CBF <30% (correlation coefficient (Rs) = 0.163, P = 0.014), was positively correlated with mismatch ratio (Rs = 0.208, P = 0.002), and was not correlated with Tmax >6 s, Tmax >4 s, or collateral vessel density (P > 0.05) (Table 3).
Correlation analysis of DBP and CTPI processing results.

DBP: diastolic blood pressure; CTPI: computed tomography perfusion imaging; CBF: cerebral blood flow: Tmax: time to maximum.
Predictive values of DBP, CBF <30%, Tmax >4 s, mismatch ratio, and their combination
ROC curve analysis of the predictive value of the combination of DBP, CBF <30%, and mismatch ratio for the clinical outcomes of patients with AIS is shown in Figure 1. The areas under the curve for DBP, CBF <30%, mismatch ratio, and their combinations were 0.657, 0.683, 0.693, and 0.711, respectively (Table 4).

Predictive value of the combinations of DBP, CBF <30%, and mismatch rate for clinical outcomes in patients with acute ischemic stroke using receiver operating characteristic curve analysis. DBP: diastolic blood pressure; CBF: cerebral blood flow.
Predictive values of DBP, CBF <30%, mismatch ratio, and their combination.

DBP: diastolic blood pressure; CBF: cerebral blood flow.
Discussion
According to the results of this study, the higher the DBP in patients with AIS, the worse their prognosis. However, patients with a history of hypertension may have a better outcome after AIS than those without hypertension. If a patient had experienced a stroke in the past, the correlation was reversed. Patient clinical outcomes were correlated with ICV obtained using F-STROKE software processing but not with collateral circulation. BP was also correlated with ICV but not with collateral circulation. Moreover, DBP combined with ischemic ICV and mismatch ratio had a higher prognostic value for patients.
The NIHSS score is a comprehensive assessment system of multiple aspects of function, such as sensation, speech, movement, and consciousness. A higher NIHSS score indicates that the patient’s intracerebral infarct foci or the impact of cerebral edema is greater; the more severe the neurological deficits, the worse the probability of poor prognosis. The NIHSS score in patients with AIS is a valid predictor of stroke outcome. 15 In our study, we defined patients with an NIHSS score > 4 as having poorer clinical outcomes, and there was a positive correlation between DBP and patient clinical outcomes, indicating that higher DBP may indicate poorer prognosis. This is similar to previous studies showing that higher BP may result in poor outcomes in patients who have experienced an ischemic stroke. 6 In contrast, some studies have suggested that a higher BP may portend a favorable prognosis for patients and that a low BP may increase the risk of death. 16 Transient decreases in BP may lead to a reduction in cerebral perfusion via both direct and indirect mechanisms. However, an increase in BP may result in higher perfusion to the lesion area, thereby improving patient prognosis. This protective mechanism is transient, and BP decreases spontaneously over time. Differences in BP measurements would then cause some degree of difference in the experiment. There has been some controversy regarding the management of SBP in patients with AIS to improve prognosis and prevent recurrence. In clinical practice, antihypertensive medications are generally discontinued preoperatively in patients who are amenable to thrombolysis; in patients for whom the opportunity for thrombolysis exists, the BP is generally controlled at 180/105 mmHg. The American Heart Association guidelines for AIS have also recommended that BP should not be lowered unless it is greater than 220/120 mmHg. 17 This is because a higher BP may have a positive effect on perfusion in the ischemic semi-domain, leading to favorable outcomes. In our study, we found that a DBP >85 mmHg plays an early warning role in clinical prognosis.
We found a close relationship between patient prognosis and ICV (CBF < 30%). Similarly, there was a correlation between DBP and ICV. Mismatch is usually used as an inclusion criterion for endovascular treatment in clinical practice to assist in clinical decision-making regarding whether to proceed with endovascular treatment. In our study, both patient outcomes and DBP were associated with mismatch. The efficacy of BP combined with CBF <30% and mismatch in predicting clinical outcomes in patients with AIS increased to 0.711. Tmax >6 s is defined as the ischemic penumbra, which is the low-perfusion area around the infarcted core area. The ischemic penumbra is currently a sensitive indicator for evaluating ischemic areas after cerebral infarction, and Tmax >6 s can be used to indirectly evaluate collateral circulation. The brain tissue structure in this area was intact but was in a stage of functional damage. If blood flow in the corresponding area is improved, brain tissue function can be restored, further affecting the final ICV. Collateral circulation exerts a considerable impact on the prognosis of ischemic areas. The presence of collateral circulation can help improve the success rate of vascular recanalization treatment, improve ischemia reperfusion, reduce the risk of bleeding transformation, and effectively improve the clinical prognosis. However, in our correlation study, we have not yet confirmed the correlation between Tmax >6 s and the quantized values of collateral circulation obtained from F-STROKE treatment and prognosis. No association was found between patient BP and ischemic penumbra and collateral circulation. This may be related to the fact that this was a single-center study with a relatively lower sample size. Furthermore, the mechanism of the correlation of different types of BP with the core volume of intracranial infarcts, semi-dark band, and establishment of collateral circulation have not yet been clarified. Some studies have suggested that sustained hypotension may trigger compensatory establishment of collateral circulation in ischemic regions in patients who have experienced an ischemic stroke. 10 However, because the BP of patients with AIS is constantly changing, the regulation of BP on the supply of intracranial ischemic core volume is imperfect. Low BP may not only increase the establishment of collateral circulation but also further increase the infarct area. 18 In similar studies, the relationship between BP status and changes in collateral branches as well as clinical outcomes may also be influenced by different factors, such as whether blood vessels are reopened after treatment in patients with infarction. 7 Further research and discussion are needed on the relationship between BP, collateral branching, and uncertain outcomes.
In summary, this study confirms that BP has an impact on the prognosis of patients with AIS but is not related to the collateral circulation density obtained from F-STROKE treatment. It has not yet been confirmed whether lowering or increasing BP can improve collateral blood flow and thus affect patient prognosis. However, parameters such as BP combined with CBF <30% and mismatch ratio can improve the predictive value of prognosis in patients who have experienced an ischemic stroke.
Footnotes
Acknowledgements
We thank all the study participants. We appreciate the feedback from the reviewers and the editorial team.
Author contributions
Yunxia Qi and Bolin Liu proposed the research idea; designed the research plan; collected, organized, and analyzed the clinical data; and drew the statistical charts. Yiying Wu assisted in statistical analysis, and Yifeng Peng was responsible for proofreading of the manuscript and overall research paper.
Data availability statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethical compliance
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
Plan of Scientific Project in Science and Technology Commission of Shanghai Municipality (Project Number:19411951404).