
Abstract
The protozoan Trichomonas vaginalis is a parasite associated with numerous sexually transmitted infections worldwide. In males, although Trichomonas vaginalis infection (also known as trichomoniasis) often remains asymptomatic, it can lead to conditions such as prostatitis or urethritis. Herein, we report the case of a man in his early 90s who was admitted to a hospital in northern Iran with mild dysuria, whose precise onset remained unclear. He had a history of chronic prostate discomfort for several years and acknowledged having multiple sexual partners over the past two decades. He complained of dysuria; therefore, urinalysis was performed, which detected trichomoniasis. He received treatment with metronidazole, resulting in the resolution of urinary symptoms and elimination of the parasite. This case highlights the importance of considering the possibility of trichomoniasis in men, especially older men, as they may face an increased risk of inflammation and prostate cancer.
Introduction
Trichomonas vaginalis is a widely distributed parasite and a key causative agent of sexually transmitted infections (STIs) worldwide. Annually, approximately 156 million new cases of T. vaginalis infection (also known as trichomoniasis) are documented globally, which impact both men and women. 1 As trichomoniasis is not a nationally notifiable disease in most countries, its prevalence is primarily estimated through population-based studies, epidemiological modeling, and research surveys rather than routine public health reporting. The World Health Organization has estimated the global prevalence of trichomoniasis as 5.3% in women and 0.6% in men. These estimates reveal significant geographic variation in the burden of trichomoniasis among men, with prevalence ranging from 0.2% to 1.3% and the highest rates being reported in the African and American regions. 1 Individuals infected with this protozoan parasite frequently report symptoms such as dysuria and urethral discharge. In men, the infection is commonly asymptomatic, although it can occasionally result in mild prostatitis or urethritis. 2 Although trichomoniasis is one of the most common nonviral STIs worldwide, its prevalence and burden in men are often underestimated owing to the high proportion of asymptomatic cases and limitations of conventional diagnostic methods. 2 Studies have indicated that most men infected with T. vaginalis do not exhibit symptoms, which contributes to underdiagnosis and continued transmission. When symptoms occur, they most commonly include urinary discomfort, such as dysuria and increased urinary frequency, and less frequently involve complications such as urethritis and prostatitis.3–6 Furthermore, epidemiological data have revealed that older men and those with certain sociodemographic factors may be at higher risk, and the infection can remain undetected in the absence of sensitive molecular diagnostic techniques.2,6 Trichomoniasis should be considered in the differential diagnosis of sexually active males who have urethral symptoms or inflammation without any evidence of discharge during physical examination. 3 Sexual transmission is the primary route; however, nonsexual transfer is also possible. 4 This extracellular parasite employs epithelial cells for attachment, which enable the parasite to infect the human host, with the urogenital tract serving as the primary tissue for colonization. 5 This report details the case of a man in his early 90s who had a history of benign prostatic hyperplasia (BPH) and was diagnosed with trichomoniasis.
Case presentation
In August 2023, a man in his early 90s presented to the emergency room at Razi Hospital in northern Iran with complaints of asymmetric leg pain and swelling in both legs, particularly in his left foot. The edema had commenced 2 weeks prior and had intensified in the previous 48 h. He also reported persistent mild dysuria over an extended duration, although he was unable to recall the exact onset of this symptom. His medical history included hypertension, ischemic heart disease, BPH, previous hospitalization 3 years ago for coronavirus disease 2019, cataract surgery, and surgical removal of a basal cell carcinoma on his forehead. In addition, he reported having multiple sexual partners over the past two decades.
In response to the patient’s report of dysuria, urinalysis (U/A) was performed, which indicated an increase in white blood cell count (25–30/hpf), red blood cell count (3–5/hpf), epithelial cell count (2–3/hpf), mucus, and bacteria, in addition to a positive result for trichomoniasis with significant flagellate mobility (Figure 1). Notably, there was no evidence of urinary casts. The patient received a single dose of 2 g metronidazole (MTZ) and was scheduled for a follow-up U/A and urine culture. The subsequent urine culture revealed no bacterial growth after 24 h; however, the U/A still detected trichomoniasis. Following treatment with a single oral dose of 2 g MTZ, the patient’s urinary symptoms improved. Additional U/A performed 1 week and 1 month later were negative for trichomoniasis. Informed consent for treatment and publication was obtained from the patient.
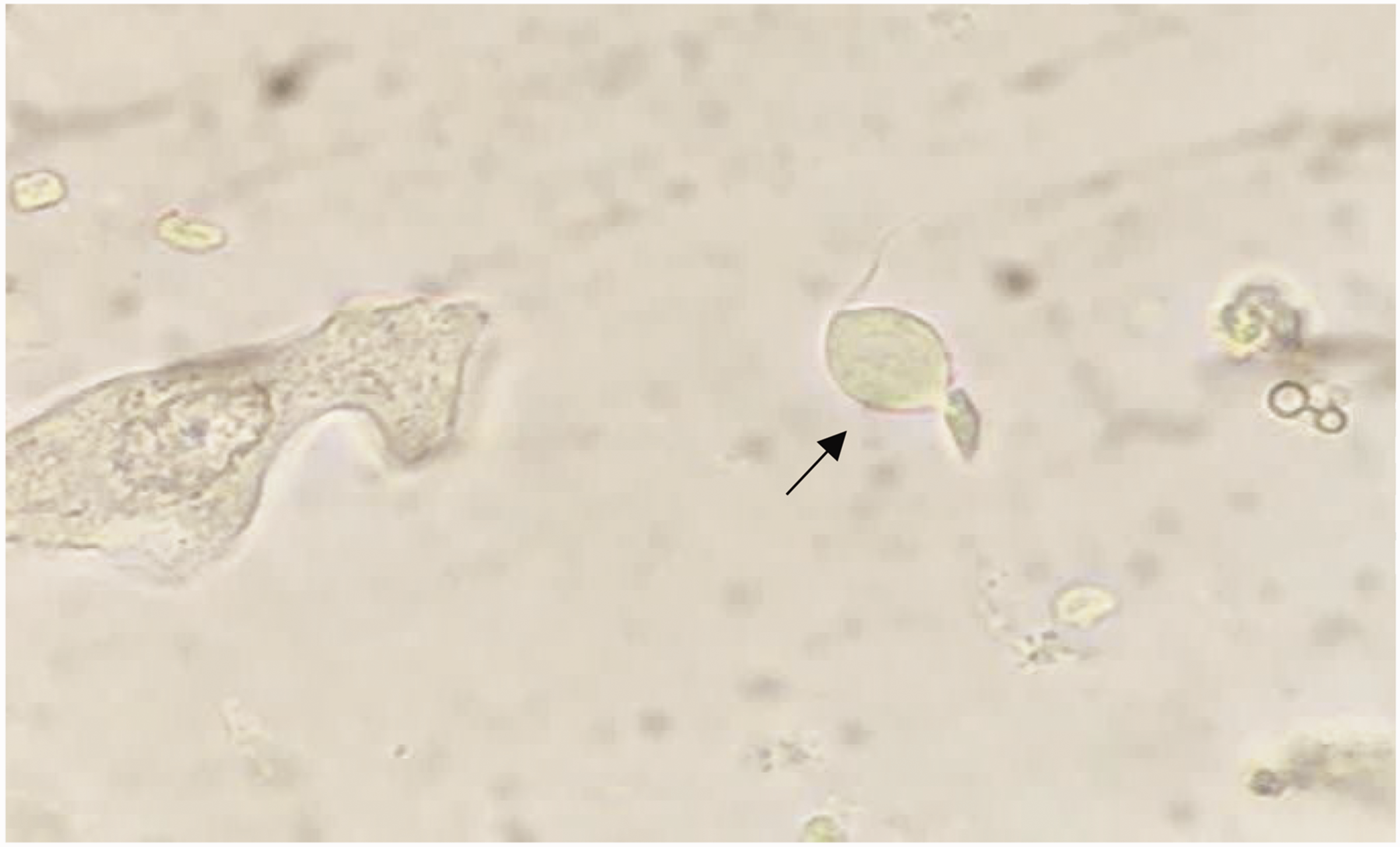
Trichomonas vaginalis (arrow) in the urine sediments of a 95-year-old man with chronic prostatitis (magnification, 400×).
Discussion
Trichomoniasis in men is often benign and self-limiting. 6 A study showed that the prevalence of trichomoniasis in men aged ≥30 years who presented with urethral discharge at sexually transmitted diseases clinics was similar to that of Neisseria gonorrhoeae infection (12%). 7 In men, trichomoniasis can cause urethritis, prostatitis, epididymitis, urinary tract infections, and diminished fertility. 6 Although the majority of patients exhibit only mild symptoms, trichomoniasis can cause significant complications. Persistent infection has been associated with impaired sperm function, infertility, and increased human immunodeficiency virus (HIV) shedding in seminal fluid. Emerging evidence suggests a potential link between chronic trichomoniasis and prostate cancer risk, although this finding remains inconclusive due to multifactorial contributors. 6 It is crucial to recognize that T. vaginalis can ascend the urethra and impact the prostate, which may result in prostatitis if not addressed. In older men with BPH (aged >55 years), trichomoniasis causing urethritis or prostatitis may aggravate urinary symptoms, such as dysuria, urination frequency, and inflammation. Chronic infection may disrupt the urogenital microbiome, potentially contributing to dysbiosis that perpetuates inflammation or facilitates coinfections. 6 However, specific data on T. vaginalis-induced dysbiosis in men remain limited compared with data on vaginal infections in women.3,5 In the present case, sustained trichomoniasis, stemming from multiple infected sexual partners over the past two decades may have played a role. In our case, as reported in several previous studies,1,3,6 a correlation appears to exist between persistent trichomoniasis and the development of BPH and, to a lesser extent, prostate cancer. However, this association remains inconclusive owing to the presence of confounding factors such as age-related hormonal changes, chronic inflammation, and microbiome alterations.
Most men typically recover quickly from this infection, indicating a possible association with variations in urogenital microenvironments. Although some studies have reported spontaneous resolution of trichomoniasis in a subset of untreated men, in most patients, the infection does not subside rapidly without treatment, and asymptomatic carriage can persist for weeks to months. The hypothesis that differences in the urogenital microenvironment, such as a more oxidative environment in men compared with a more reductive environment in women may influence parasite survival, is supported by experimental and clinical observations, although direct evidence in humans remains limited. Additionally, higher concentrations of zinc in prostatic fluid may exert trichomonacidal effects, potentially contributing to shorter infection duration or reduced organism viability in men. Nevertheless, comprehensive knowledge regarding the clinical complications of this infection in men remains limited.8,9
The Centers for Disease Control and Prevention (CDC) recommends that men diagnosed with trichomoniasis or those who have had sexual exposure to the infection should receive treatment to mitigate the risk of transmission to their female sexual partners. The conventional treatment approach for trichomoniasis typically involves the administration of 2 g MTZ or oral tinidazole. Another option is a multidose regimen of oral MTZ, which consists of 500 mg MTZ taken twice daily over a period of 7 days. 6 A randomized controlled trial conducted among HIV-uninfected women showed that compared with a single dose of 2 g MTZ, a multidose MTZ regimen significantly reduced the percentage of women diagnosed with trichomoniasis at the 1-month follow-up. In addition, men received the greatest benefit from the single-dose treatment of 2 g MTZ. 9
Studies conducted in the United States have revealed that individuals infected with trichomoniasis tend to be older than those infected with other STIs. Furthermore, the average age of men infected with T. vaginalis was approximately 10 years higher than that of their female counterparts. Fluctuations in reproductive hormone levels among men may contribute to a heightened susceptibility to trichomoniasis. 10 Lindrose et al. demonstrated that the prevalence of trichomoniasis is significantly higher in older populations than in younger adults. 11 Herein, we reported trichomoniasis in a man in his early 90s, an unexpected finding in this age group. It is crucial to recognize the possibility of this infection in older patients because they are at an increased risk of conditions such as inflammation and prostate cancer. 11 Future investigations should aim to pinpoint specific subgroups within the older population who may be more susceptible to trichomoniasis or its associated complications. 11 This study’s reporting adheres to the Case Report (CARE) guidelines. 12
Conclusion
This case of a man in his 90s with persistent trichomoniasis and BPH underscores the importance of considering trichomoniasis in older men with urinary symptoms, even among those without classic STI risk factors. Trichomoniasis can aggravate lower urinary tract issues and potentially contribute to prostatic inflammation in this demographic population. Our findings combined with existing research suggest a link between chronic trichomoniasis and BPH; however, further research is needed to clarify the nature of this association. Clinicians should remain vigilant regarding this infection in older individuals, particularly given the potential for underdiagnosis and the need for targeted management strategies.
Footnotes
Acknowledgement
We would like to appreciate the assistance offered by the colleagues at Razi Hospital, Northern Iran.
Author contributions
MF and SSA played pivotal roles in the conceptualization and design of the research study. The initial draft of the manuscript was written by MF and SSA. SK, SSB, A. Nooreddini, and A. Nozari wrote sections of the manuscript. MF obtained information from the patient’s records. HN and ES were responsible for collecting data and submitting the manuscript. All authors have made significant contributions to the critical revision of the manuscript and thoroughly reviewed and endorsed the final submitted version.
Data availability statement
The data are available from the corresponding author on request.
Declaration of conflicting interests
None declared.
Ethics approval
This research was approved by the research ethics committee of the Mazandaran University of Medical Sciences (IR.MAZUMS.REC.1397.2969).
Funding
No funding was received for this study.