
Abstract
Pneumocystis jirovecii is a ubiquitous opportunistic fungus that can cause life-threatening pneumonia. The clinical manifestations of pneumonia caused by severe acute respiratory syndrome coronavirus 2 and P. jirovecii are similar, posing a significant challenge in the diagnosis of P. jirovecii pneumonia or coronavirus disease 2019. Herein, we report a case of P. jirovecii pneumonia diagnosed through bronchoalveolar lavage and sputum smear analyses. The patient recovered successfully and was discharged following combination therapy with trimethoprim/sulfamethoxazole and corticosteroids. Early diagnosis and prompt treatment are of vital importance in managing P. jirovecii pneumonia, particularly in individuals with related risk factors for P. jirovecii pneumonia development.
Keywords
Introduction
Pneumocystis jirovecii is a ubiquitous opportunistic fungus that can cause life-threatening pneumonia. Although P. jirovecii pneumonia (PJP) is a well-known and frequent opportunistic infection in patients with human immunodeficiency virus (HIV) infection, its occurrence in patients with coronavirus disease 2019 (COVID-19) has recently gained attention. Most reports of coinfection with P. jirovecii have been published during the infection period of COVID-19, with limited reports of PJP infection during the recovery phase. Herein, we report a case of a patient with PJP who developed fever, cough, sputum, and dyspnea after hospital discharge during the resolution of COVID-19 pneumonia. Concurrently, the literature on COVID-19 convalescence complicated by PJP was retrospectively analyzed to explore its clinical characteristics and provide references for clinical diagnosis and treatment.
Case report
An older woman in her 70s was admitted to our department due to fever and cough. She had been previously diagnosed with COVID-19 in a local hospital 1 month ago and was treated with antiviral therapy using nematovir/ritonavir and anti-inflammatory medication using methylprednisolone. However, methylprednisolone was discontinued 5 days before this admission. Upon further investigation using chest computed tomography (CT), signs of improved lung exudation were observed compared with those in previous scans at the local hospital. Despite this improvement, her fever recurred, and her cough worsened 3 days before admission. She had attempted self-treatment with moxifloxacin at home for 3 days without symptom improvement, prompting her visit to our clinic.
Her medical history was unremarkable, and she denied hepatitis, tuberculosis, hypertension, diabetes, and heart disease. She had received the COVID-19 vaccine.
Upon admission, tests for COVID-19 through polymerase chain reaction (PCR) and antigen detection using nasopharyngeal swabs showed negative results. Analysis of blood routine indicated normal white blood cell counts with a predominance of neutrophils. Her C-reactive protein levels were elevated at 242.5 mg/L, and the lactic dehydrogenase level was 350 U/L.
Following admission, the patient received 3 days of anti-infection therapy with meropenem. On the third day, the patient’s condition unexpectedly changed. Specifically, her oxygen saturation suddenly decreased. With the assistance of a 10 L/min oxygen storage mask, her finger oxygen saturation was maintained at approximately 97%. Furthermore, the arterial partial pressure of oxygen/fraction of inspired oxygen (PaO2/FiO2) ratio decreased to 130. Chest CT showed diffuse exudative changes in both lungs with thickening of the interlobular septum (Figure 1). This led to a suspicion of either viral pneumonia or PJP. Based on clinical experience, PJP was considered more likely. Therefore, the patient was treated with trimethoprim/sulfamethoxazole (TMP/SMX) (three tablets orally every 6 h) and methylprednisolone (40 mg every 12 h).
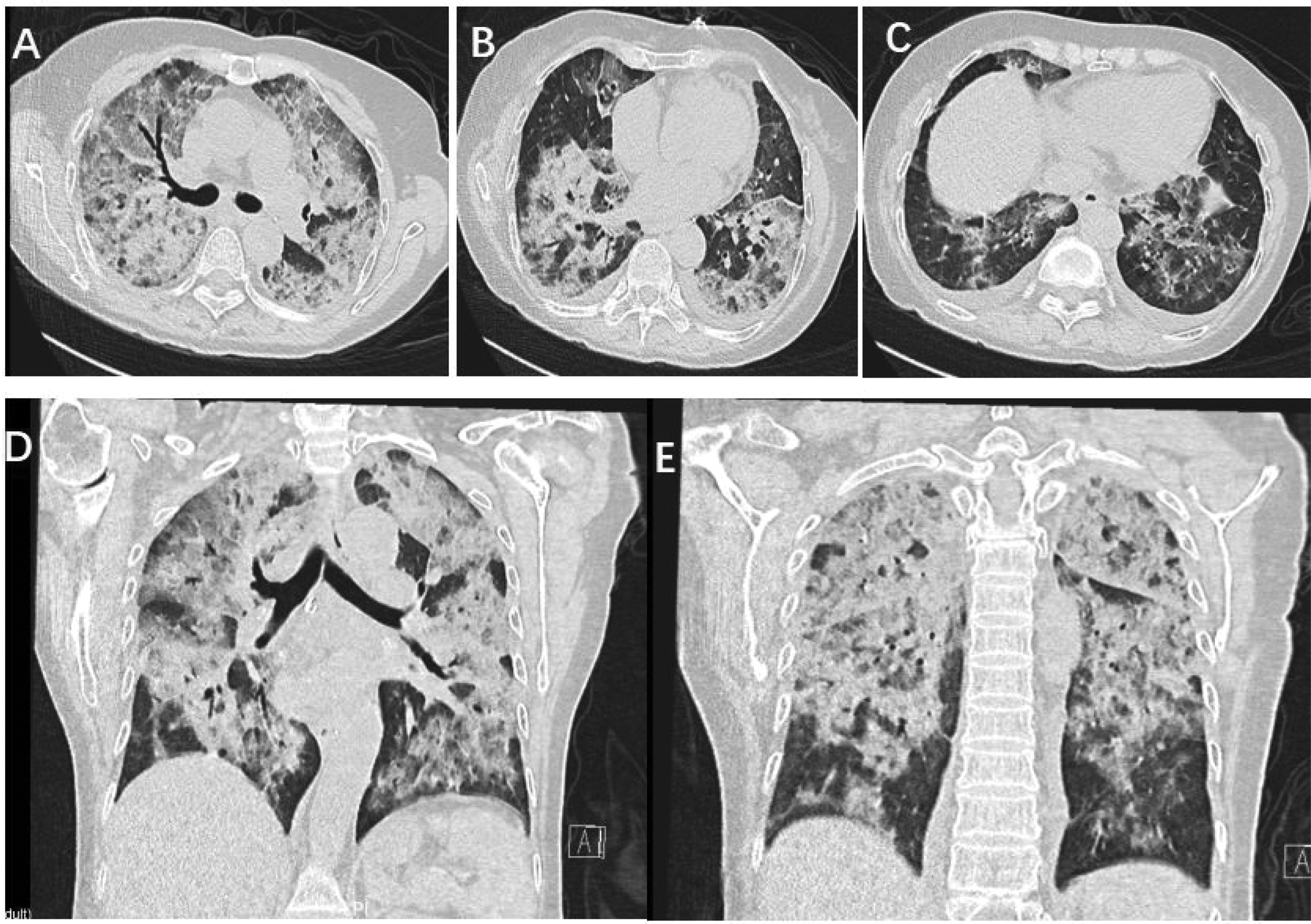
Chest computed tomography immediately showed diffuse exudative changes in both lungs and thickening of the interlobular septum (day 3).
Later, in that afternoon, the patient’s respiratory condition worsened, with a further decrease in pulse oxygen saturation. Despite the use of a 15-L/min oxygen storage mask, the pulse oxygen saturation was maintained at approximately 88%. The critical decline resulted a low PaO2/FiO2 ratio of 87, prompting the need for emergency tracheal intubation. The patient was urgently transferred to the intensive care unit (ICU) for treatment.
After transfer to the ICU, alveolar lavage and metagenomics next-generation sequencing (mNGS) analysis of lavage fluid were performed. Notably, P. jirovecii was detected in alternate-day lavage fluid via mNGS. Additionally, positive results were obtained from both lavage fluid fungal 1-3-β-D glucan (BDG) test at 600 pg/mL and blood G test at 229 pg/mL. P. jirovecii was also identified via the immunofluorescence assay of sputum smear. Based on these findings, the patient was immediately started on a combination therapy with TMP/SMX and caspofungin for treating PJP.
After 4 days of combined therapy, the tracheal intubation was successfully removed, and ventilator support was discontinued. The patient was then transferred back to the general ward while continuing caspofungin treatment. After 3 weeks of TMP/SMX therapy, chest CT showed significant improvement (Figure 2). After 4 weeks of treatment, the lesions were almost completely resolved, with only residual fibrous cords remaining in both lungs (Figure 3).
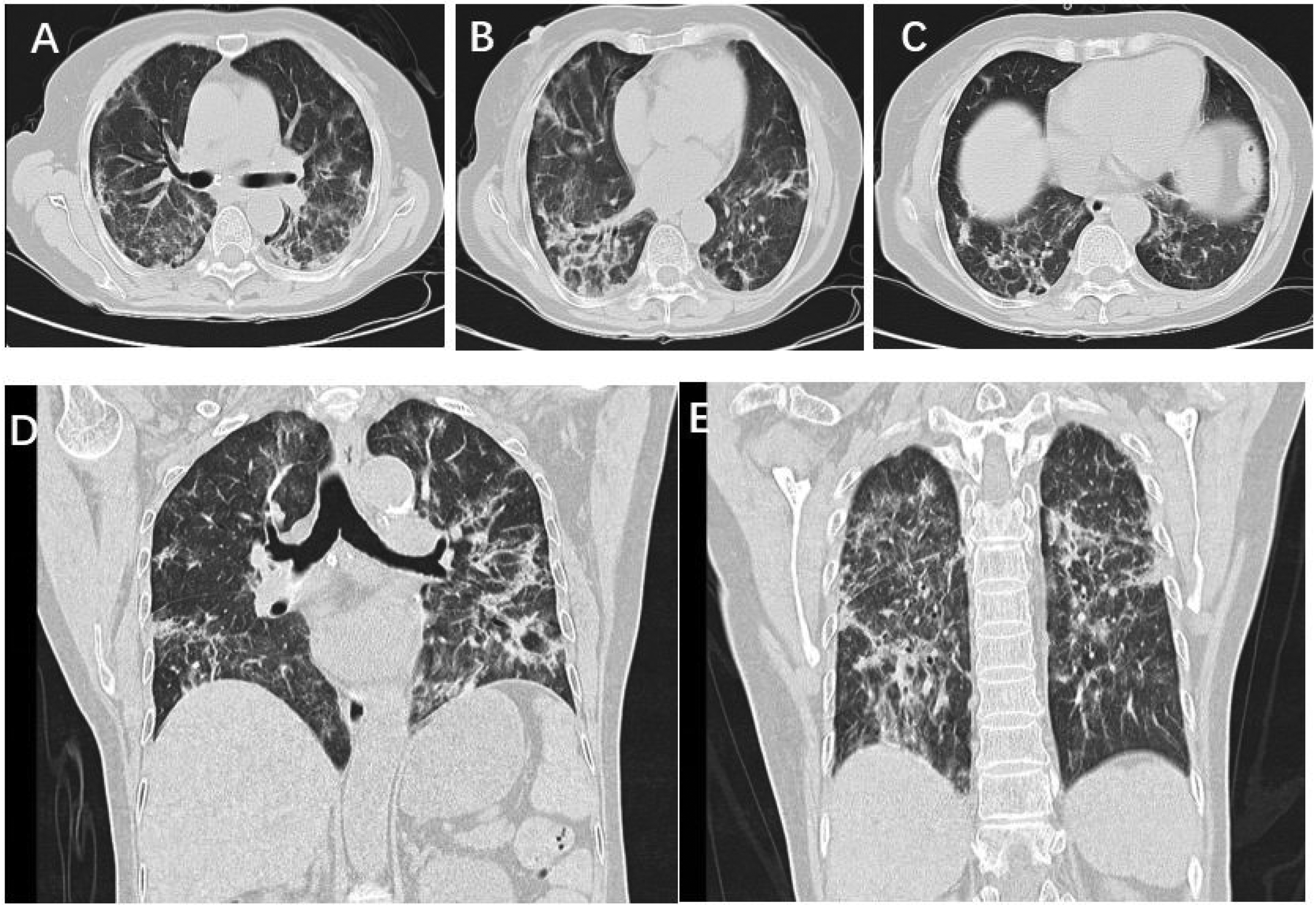
Chest computed tomography changes in pulmonary lesions of the patient (after 3 weeks of TMP/SMX treatment).

Chest computed tomography changes in pulmonary lesions of the patient (after 4 weeks of TMP/SMX treatment).
Methods of research strategy
A literature search was conducted in PubMed, Web of Science, Embase, Scopus, and the Cochrane Library using the following search terms, limited to titles and abstracts: ((Coronavirus Disease 2019) OR (COVID-19) OR (Novel Coronavirus) OR (2019 Novel Coronavirus) OR (Severe Acute Respiratory Syndrome Coronavirus 2)) AND ((Pneumocystis jirovecii pneumonia) OR (P. jirovecii pneumonia) OR (PJP)).
Only case reports published in English between 1 December 2020 and 31 October 2024 were included. These reports described patients with a proven or probable diagnosis of PJP according to the European Organisation for Research and Treatment of Cancer and Mycoses Study Group (EORTC/MSG) 2020 criteria1,2 and severe pneumonia according to the American Thoracic Society and Infectious Diseases Society of America 2019 criteria. 3 A total of 891 articles were identified. Two authors (JLL and ZYX) independently reviewed these articles, selecting those that met the inclusion criteria based on the title and abstract, in accordance with the EORTC/MSG 2020 guidelines. Ultimately, 5 articles, encompassing 11 patients, were included. Figure 4 shows a flow diagram presenting the search and study selection strategy. A total of 11 patients were reported in the literature (Table 1).

A flow diagram presenting the search and study selection strategy.
Clinical features of 11 patients with PJP during the convalescence of COVID-19.

BALF: bronchoalveolar lavage fluid; BDG: (1,3)-β-D-glucan; CT: computed tomography; PCR: polymerase chain reaction; PJP: Pneumocystis jirovecii pneumonia; SMX: sulfamethoxazole; TMP; trimethoprim; COVID-19: coronavirus disease 2019.
Discussion
Among the 11 patients selected,4–8 the average age was 61 years, with a male proportion of 81.8%. The median period between the occurrence of COVID-19 and the development of PJP in all patients was 29 days. The most common comorbidity was diabetes mellitus (n = 5; 45.5%), followed by chronic kidney disease, hematological malignancy, autoimmune diseases, and renal transplant. The common clinical manifestations comprised fever, cough, and dyspnea, which align with those reported in a previous study. 9
PJP is an opportunistic pathogenic fungal infection caused by P. jirovecii, 10 especially in patients with HIV infection. However, the incidence of severe PJP cases in HIV-negative patients has been on the rise.11,12 The use of corticosteroids and adjunctive immunomodulatory agents is the most important risk factor for PJP in non-HIV patients.13,14
COVID-19 is characterized by clinical manifestations ranging from paucisymptomatic illness to interstitial pneumonia, leading to respiratory failure and ICU admission. 15 In severe cases, patients often need to be treated with steroids, which suppress the immune system. 16 All 11 patients were administered systemic steroids during COVID-19 treatment. One patient who underwent kidney transplantation required long-term oral prednisolone, mycophenolate mofetil, and tacrolimus for immunosuppressive therapy. 4 Another patient took prednisolone orally daily for interstitial pneumonia and rheumatoid arthritis. 6
The clinical manifestations of pneumonia caused by severe acute respiratory syndrome coronavirus 2 and P. jirovecii are similar, often presenting symptoms such as fever, cough, and dyspnea. Radiographic similarities include the appearance of ground-glass opacities or infiltration or consolidation changes on lung CT.17–19 The diagnosis of PJP versus COVID-19 can be challenging. 20 Six patients showed ground-glass opacities, with five cases showing infiltration and four demonstrating consolidation changes on CT. There was no significant difference between the imaging findings of PJP and COVID-19.
The suspicion of PJP is typically based on clinical factors and imaging results. To confirm the presence of PJP, specific laboratory testing, including serum markers and clinical specimens, is necessary. 21 Serum BDG is the most advantageous serum biomarker for PJP assessment. BDG, a polysaccharide, is found in the antigenic cell wall component of many fungi. 22 Serum BDG level increases only in reaction to fungal infections. 23 Many studies have reported that BDG has high sensitivity ranging from 85% to 100% and low specificity from 54% to 75%.24–26 In this case, the serum BDG tests showed positive results in eight patients.
Currently, due to the growth limitations of P. jirovecii, culture is not a routine means of definitive diagnosis. PJP diagnosis is based on the direct microscopic examination or a positive PCR result of respiratory samples such as bronchoalveolar lavage fluid (BALF) or sputum.27,28 Direct microscopic examination is appealing as the main specific test for PJP. However, many hospitals do not recommend using noninduced sputum for Pneumocystis species testing.29,30 Bronchoscopy is an invasive procedure used to obtain BALF samples; however, this technique is associated with attendant risks and is expensive in certain patients. 31 Nevertheless, compared with other samples, it is more advantageous to obtain BALF specimens from intubated patients in ICU. Etiological evidence was obtained via BALF PCR in five patients and sputum smear analysis in two patients. The other four patients’ etiologies were not clearly identified.
Regarding the current therapy, the preferred treatment regimen remains the utilization of trimethoprim/sulfamethoxazole (TMP/SMX).32,33 However, the use of corticosteroids remains controversial. Fishman and Gans 34 recommended that prednisone should be given within 72 h to critically ill patients, with gradual dose reduction. In a 10-year retrospective study involving 323 HIV-negative patients with PJP, Wieruszewski et al. 35 observed that the use of steroids within the initial 72 h had no significant benefits. The patient described in this report received a combination of TMP/SMX and steroids. Of the 11 patients, 1 exhibited an allergic reaction to TMP/SMX, which was subsequently replaced with atovaquone. Despite aggressive treatment, half of the patients included in the literature review succumbed to the disease, consistent with previous reports. 36
Conclusions
Among patients diagnosed with COVID-19 pneumonia, even in the recovery state, the possibility of PJP infection should be considered if worsening of respiratory failure and typical CT suggesting a secondary infection are noted, especially when the patient has COVID-19-related risk factors for PJP development.
A misdiagnosis or delayed diagnosis of opportunistic infections can lead to perilous consequences. Thus, physicians should consider not only COVID-19 in febrile patients with respiratory symptoms but also opportunistic infections such as PJP.
Footnotes
Acknowledgments
The authors sincerely thank the editors and reviewers for their feedback and comments.
Authors’ contributions
JLl, ZYX and WJY collected the data. ZYX drafted the manuscript. WOY and FX revised the manuscript. All authors read and approved the final manuscript.
Consent for publication
The reporting of this study conforms to the Case Report (CARE) guidelines. 37
Data availability statement
Data will be made available on request.
Declaration of conflicting interests
The authors have no competing interests to declare that are relevant to the content of this article.
Ethics approval and informed consent
This study was authorized by the Ethics Commission for Clinical Research of the Second Affiliated Hospital of Zhejiang University School of Medicine (ethics approval no. (2023) No. (1275)). We have de-identified all patient details. The need for informed consent was waived due to the nature of the retrospective study.
Funding
This research is funded by Key research and development program of Zhejiang Province (No. 2025C02093).