
Abstract
Objective
To identify the correlation between serum inflammatory cytokines and immune markers in children with severe hand, foot and mouth disease (HFMD).
Methods
Paediatric patients with severe or mild HFMD from Linping Campus, the Second Affiliated Hospital of Zhejiang University, were included in this retrospective study. Data comprising demographic characteristics, clinical symptoms and signs, laboratory findings and other factors were collected. Serum interleukin (IL)-1, IL-6, IL-10, tumour necrosis factor (TNF)-α, and interferon (IFN)-γ levels were measured by enzyme-linked immunosorbent assay at 1, 3, and 5 days after admission. Risk factors were screened using multivariate logistic regression analysis.
Results
A total of 200 patients with HFMD (120 severe and 80 mild cases) were included. Younger age and longer fever duration were associated with severe HFMD, as were increased white blood cell, neutrophil and platelet counts, blood glucose, immunoglobulin (Ig)M and IgG. IL-6 and IL-10 levels were higher in patients with severe versus mild HFMD on days 1, 3 and 5. TNF-α was higher in the severe group on day 3. Increased white blood cell and neutrophil counts, IL-6, IL-10, and IgG levels, age, fever duration, and blood glucose level were found to be risk factors associated with the occurrence of severe HFMD.
Conclusions
Inflammatory cytokines and immune indexes may be related to the occurrence of severe HFMD.
Introduction
Hand, foot and mouth disease (HFMD), caused by highly contagious intestinal viruses, is a common infectious disease among infants and children, particularly preschool children. 1 Most patients with HFMD have mild symptoms and can be cured within 7–10 days. However, a small number of patients will worsen and experience nervous system damage and cardio pulmonary failure, which may lead to death.2,3 Early prediction of severe HFMD with worsening conditions, and timely appropriate treatment and nursing, may significantly improve treatment and prognosis in children, thus improving the quality of survival.4,5
Markers of inflammation and immune indexes may be useful for understanding the prognosis of patients with HFMD, as children with severe HFMD show perturbations in cellular and humoral immunity.6,7 Immune and metabolic changes have been demonstrated in patients with HFMD, however, the association of these changes with HFMD severity has not been demonstrated. The aim of the present study was to investigate the dynamic changes of inflammatory cytokines and immune index levels in patients with severe HFMD after hospital admission, and to explore the correlation between severe HFMD and serum inflammatory cytokines and immune index levels, and indicators for predicting severe HFMD, to provide a basis for disclosing the pathogenesis of these severe cases.
Patients and methods
Study population
Paediatric patients with HFMD who were admitted to the Linping Campus, the Second Affiliated Hospital of Zhejiang University, between January 2018 and January 2024, were sequentially enrolled into this observational study. HFMD cases were diagnosed following the Chinese Ministry of Public Health ‘hand, foot and mouth disease treatment guidelines’ (revised in 2010). The inclusion criterion was enterovirus 71 infection detected as the disease-causing pathogen. Cases with acute flaccid paralysis, myocarditis, encephalitis, and pulmonary oedema were classified as severe, and cases without the above symptoms were classified as mild. Exclusion criteria were: patients with congenital heart disease, pneumonia, and/or autoimmune disease. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013, and the reporting of this study followed the STROBE guidelines for observational studies. 8 All patient details have been de-identified, and all parents (legal proxies) of the included children provided written informed consent to study participation. The Linping Campus, the Second Affiliated Hospital of Zhejiang University Ethics Committee approved the study (Approval number: linping2023044).
Data collection
Demographic and clinical characteristics, including clinical symptoms, were retrospectively extracted from medical records. Immune index and laboratory indicators were obtained from the results of general blood tests for clinical diagnosis after hospital admission. For each patient, serum inflammatory cytokine levels were determined using enzyme-linked immunosorbent assay kits (ZK-H064, ZK-H238, ZK-H157, ZKH042; Shenzhen Zike Biotechnology Company, Shenzhen, Guangdong, China) on day 1, 3, and 5 of admission. Assays were performed according to the manufacturer’s instructions.
Statistical analyses
Data are presented as n (%) prevalence, mean ± SD, or median (interquartile range) and were statistically analysed using IBM SPSS for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). Differences between groups or subgroups were assessed by Student’s t-test or Kruskal–Wallis one-way ANOVA, according to the distribution of continuous data. Χ2-test or Fisher’s exact test were used to analyse between-group differences in the proportions of categorical variables. Multivariate logistic regression analysis was performed on variables that were selected according to the results of the likelihood-ratio test. Risk factors with a significance level ≤ 0.05 were included and significance level > 0.05 were excluded. A P value < 0.05 was considered statistically significant.
Results
General information
A total of 200 paediatric patients with HFMD were enrolled into the study, including 120 severe and 80 mild cases (Table 1). A representative image depicting the clinical manifestation for phenotypic identification of HFMD is displayed in Figure 1. Comparisons of baseline demographic and basic symptom characteristics revealed statistically significant differences in age, length of hospital stay and fever duration between patients with severe and mild HFMD (P < 0.05, Table 1).
Baseline characteristics of 200 paediatric patients hospitalised due to hand, foot and mouth disease (HFMD).

Data presented as mean ± SD, n (%) prevalence, or median (interquartile range).
Student’s t-test, Kruskal–Wallis one-way ANOVA, Χ2-test or Fisher’s exact test.
NS, no statistically significant between-group difference (P > 0.05).

Clinical manifestation for phenotypic identification of hand, foot and mouth disease.
Immune indexes and laboratory findings
To evaluate the association of immune indexes and laboratory findings with the severity of HFMD, data from blood tests performed during clinical diagnosis were analysed. Levels of peripheral white blood cells (WBCs), platelets, neutrophils, lymphocytes, eosinophils, blood glucose and concentrations of immunoglobulin (Ig)M, IgA, IgG, complement (C)3 and C4 from mild and severe cases were included (Table 2). Compared with mild HFMD cases, the numbers of WBCs, platelets, and neutrophils, and the levels of blood glucose, IgG and IgM, were significantly increased in severe cases, while the numbers of lymphocytes and eosinophils, and the levels of C-reactive protein (CRP), IgA, C3, and C4 were not associated with severe HFMD (P > 0.05). These data suggest that immune and laboratory changes may serve as potential predictors of severe HFMD.
Laboratory findings in peripheral blood from 200 paediatric patients hospitalised due to hand, foot and mouth disease (HFMD).

Data presented as mean ± SD or median (interquartile range).
CRP, C-reactive protein; IgM, immunoglobulin M; IgA, immunoglobulin A; IgG, Immunoglobulin G; C3, complement 3; C4, complement 4.
Student’s t-test or Kruskal–Wallis one-way ANOVA.
NS, no statistically significant between-group difference (P > 0.05).
Inflammatory cytokines
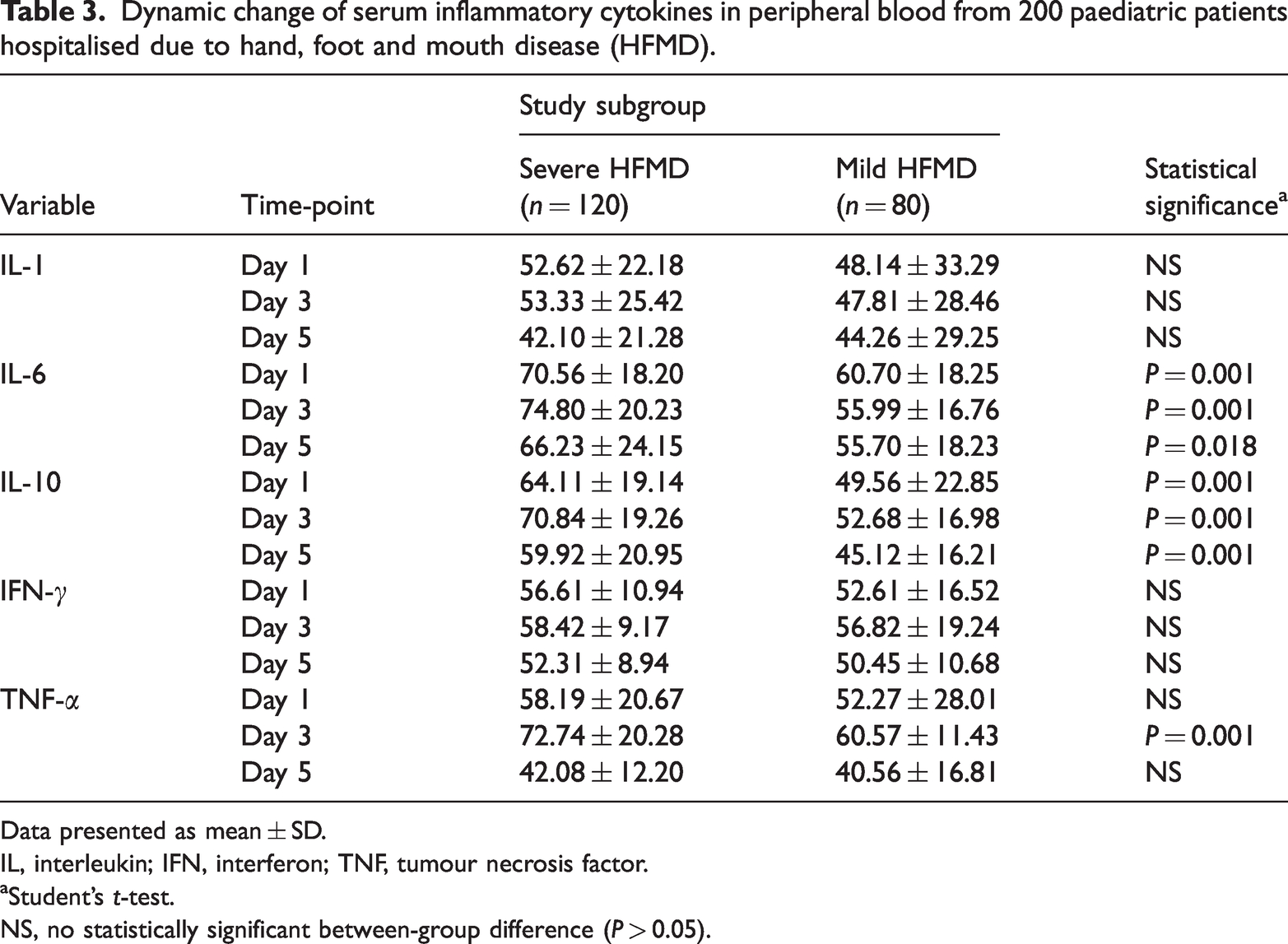
Serum interleukin (IL)-6 and IL-10 levels were significantly higher in the severe group than in the mild group on days 1, 3 and 5 of admission (P < 0.05), and both peaked on day 3 (Table 3). In addition, tumour necrosis factor (TNF)-α was significantly higher in the severe group on day 3 (P = 0.001), when it also peaked. IL-1 and interferon (IFN)-γ were not found to be associated with severe HFMD (P > 0.05).
Dynamic change of serum inflammatory cytokines in peripheral blood from 200 paediatric patients hospitalised due to hand, foot and mouth disease (HFMD).
Data presented as mean ± SD.
IL, interleukin; IFN, interferon; TNF, tumour necrosis factor.
Student’s t-test.
NS, no statistically significant between-group difference (P > 0.05).
Multivariate logistic regression analysis
Multivariate logistic regression analysis was performed to further determine the factors influencing clinical outcomes in patients with severe HFMD. The regression model included variables that showed statistically significant between-group differences in the initial analyses (Tables 1–3). Age, duration of fever, blood glucose, WBC and neutrophil counts, IgG, IL-6, IL-10 and TNF-α were all found to be significant risk factors associated with severe HFMD (P < 0.05; Table 4). The Hosmer–Lemeshow goodness of fit test was applied and revealed a good degree of fit to the model (χ2 = 5.643, P = 0.540). Although length of hospital stay, platelet count, and IgM were found to be statistically significant in the between-group analyses, they were not found to be statistically significantly associated with severe HFMD in the logistic regression (P > 0.05).
Multivariate logistic regression analysis of risk factors associated with severe hand, foot and mouth disease in 200 hospitalised paediatric patients.

OR, odds ratio; CI, confidence interval; IgG, immunoglobulin G; IL, interleukin; TNF, tumour necrosis factor.
Discussion
Although the majority of HFMD cases are generally self-limiting and mild, a small number of children may rapidly develop severe complications that could be life-threatening.9,10 Therefore, it is necessary to understand the risk factors that may predict the occurrence of severe cases. Accordingly, the aim of the present study was to explore risk factors that might indicate a child’s risk of progression to severe HFMD, and to provide further information to help identify patients who may progress at an early stage.
Consistent with previous studies,11,12 the present data showed that age may be a risk factor for severe HFMD, which might be due to the underdeveloped immune system of young children. In addition, fever duration may also be a risk factor for severe HFMD, with a previous study indicating that long fever duration was associated with the severity of disease. 13 However, the present research suggested that there was no significant association between clinical outcomes and sex, maximum body temperature or residence in a rural area, suggesting that these factors have little effect on disease progression.
Neutrophils, macrophages, and WBCs have been reported to be associated with HFMD.14,15 The present research also found that WBCs and neutrophils may play an important role in severe HFMD, possibly due to the fact that they are part of the first line of defence against disease and are immediately recruited to the site of inflammation. 16 IgG, produced by plasma B cells, plays important roles in host defence against pathogens, protecting the body from infection by binding to the invading pathogens. 17 The present data suggest that increased levels of IgG may predict severe HFMD, in accordance with a previous study. 18 Blood glucose level has been reported as a risk factor for HFMD in numerous previously published studies,19,20 and was also found to be associated with severe HFMD in the present study.
Inflammatory cytokine levels are significantly increased in patients with severe HFMD, and are closely correlated with prognosis.21,22 TNF-α, IL-10 and IL-6 are inflammatory mediators, playing a role in modulating the inflammatory response, 23 and IL-6 and IL-8 are pro-inflammatory cytokines. As an inducer of tissue damage, abnormal increases in IL-6 have been associated with immune damage in HFMD, 21 and high levels of IL-6 may exacerbate tissue damage and even cause death, which is closely related to the severity of disease. 24 In the present study, the inflammatory cytokines TNF-α, IL-10 and IL-6 were found to be associated with the occurrence of severe HFMD, which conforms to the results of previous studies. 25
Conclusion
In summary, the release of inflammatory cytokines plays a major role in the occurrence and development of HFMD, and levels of inflammatory cytokines and immune indexes in children with HFMD is of great significance for the diagnosis and prognosis of severe HFMD. The results of the present study may be limited by several factors, such as the single-centre study setting and relatively small sample size, and different treatment regimens may have affected the results. Accordingly, further retrospective studies should be conducted to understand the underlying risk factors for severe HFMD.
Footnotes
Author contributions
Xiao Li wrote the main manuscript text. Qian Zhou prepared the tables and was responsible for supervision. Both authors reviewed the manuscript final version.
Availability of data and materials
All data relating to this research are included within the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.