
Abstract
Lipomas are the most prevalent benign soft-tissue tumours, however, pedunculated fibrolipoma in the buttock is rare. Here, the case of a Chinese male patient in his early 70s with a 50-year history of a growing pedunculated fibrolipoma on his right buttock is presented. The attending physician and the registered nurse collaborated on a treatment plan, leading to a successful resection with rhomboid flap transfer. The operation went smoothly, and with continued home care and follow-ups, the patient recovered well, without complications. At 4 months post-surgery, the incision had healed perfectly, boosting the patient’s psychological state and allowing him to resume his daily activities unhindered.
Introduction
Lipomas, the most prevalent benign mesenchymal tumours, can develop in any location where fat is normally present. They primarily arise in subcutaneous tissues but may also occur in deeper layers. Fibrolipoma, a microscopic variant of lipoma, is characterized by a significant fibrous component interspersed among lobules of fat cells. 1 The World Health Organization classifies fibrolipoma as an uncommon histological variant of conventional lipoma. 2
While lipomas represent the most frequent benign soft-tissue tumours, pedunculated fibrolipoma is a rare case. 3 Pedunculated fibrolipoma, a rare manifestation of nevus lipomatous cutaneous superficialis, typically presents as large, solitary, slow-growing nodules or plaques that are pedunculated to dome-shaped and skin-coloured. These lesions predominantly occur on the buttocks and upper thighs, although other affected areas may include the back, shoulders, knees, neck, and ears, often in regions subjected to pressure. 4 Lipofibromas manifest in two forms: sessile and pedunculated. Generally asymptomatic, they may provoke symptoms that interfere with daily activities as they enlarge. 3 Fibrolipomas, a histologic subset of lipomas, consist of mature adipocytes blended with fibrous connective tissue. Reported cases of fibrolipomas have demonstrated variability in size and anatomical location. 5 Although not life-threatening, pedunculated fibrolipomas can ulcerate or lead to other functional impairments; hence, surgical excision remains the definitive treatment.3,4
Case report
Presentation
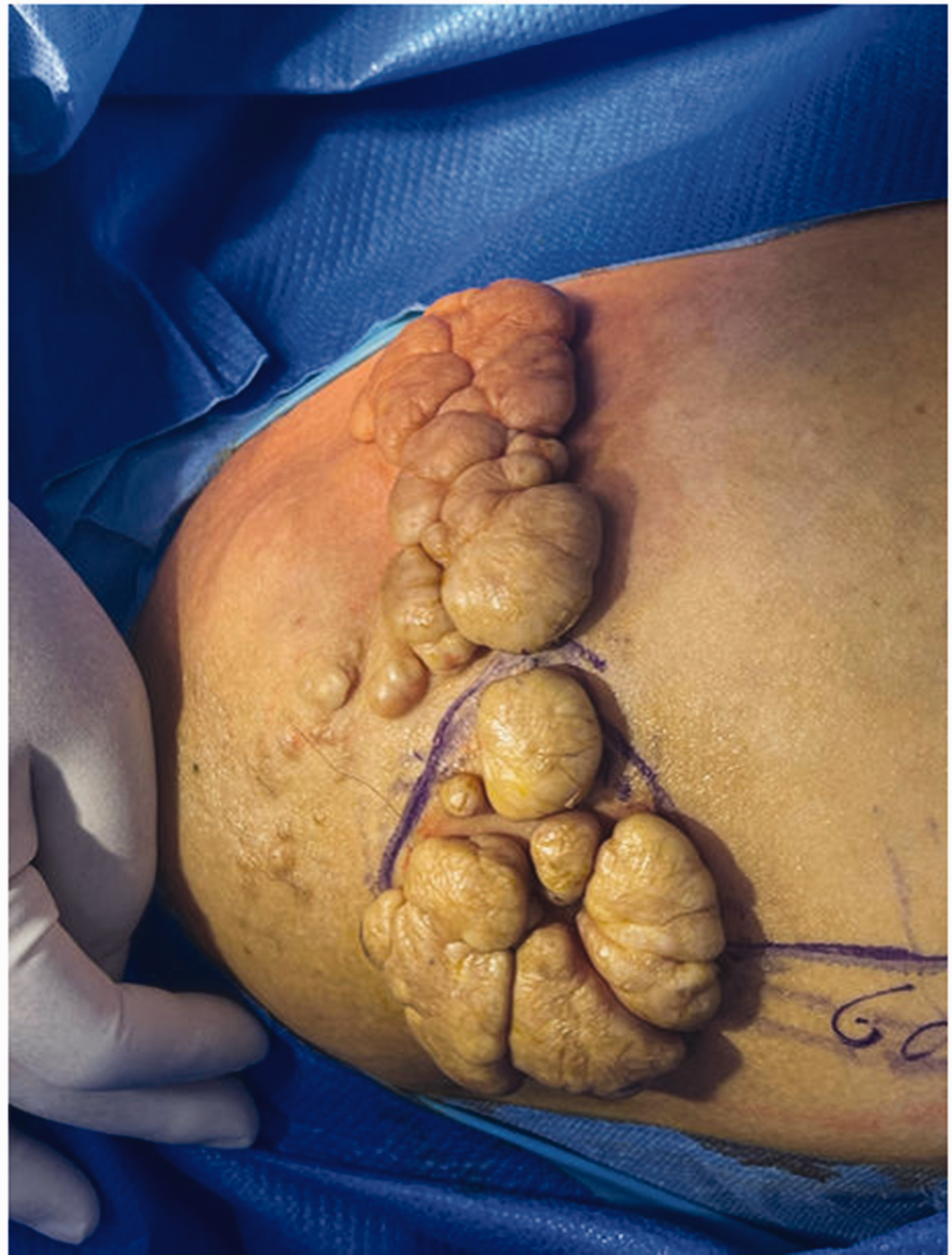
A Chinese male in his early 70s reported noticing a soft, movable, pedunculated mass in his right hip over 50 years previously, approximately the size of a soybean. As the mass was small and asymptomatic, and due to financial constraints and rural living, he did not seek medical attention. Over the subsequent decades, the mass persisted, and additional similar masses appeared around the original lesion, with the largest reaching the size of a ping pong ball. Eventually, at the recommendation of family members, the patient sought hospital evaluation and treatment. Physical examination revealed a 15 cm × 10 cm soft mass in the right buttock, comprising a cluster of dense pedunculated lesions. The mass exhibited no signs of redness, swelling, ulceration, or tenderness, and it had well-defined margins (Figure 1). The patient presented with no medical, family, and psycho-social history. After adequate treatment design, informed consent to treatment was obtained from the patient.

Presurgical image showing a 15 cm ×10 cm soft mass in the right buttock of a Chinese male patient in his early 70s.
Preoperative skin cleaning care
In the present case, the pedunculated fibrolipoma differed from ordinary fibrolipomas by exhibiting dense growth of large pedunculated tissues. The entire disease course had persisted for over 50 years, resulting in significant accumulation of skin debris at the base of each pedunculated fibrolipoma. This skin debris adhered stubbornly to the skin surface, making it impossible to completely remove with standard preoperative skin cleansing. To address this, paraffin oil was initially applied to dissolve the accumulated dirt within the interstices of the masses. Subsequently, povidone-iodine was employed for localized cleansing of the surgical area, effectively dislodging and removing the dirt. This enhanced cleaning protocol was pivotal in significantly diminishing the microbial load on both the skin at the surgical site and its vicinity.
Liquid paraffin, a colourless and transparent oil, is odourless and tasteless, and exhibits a neutral acidity, protecting against skin irritation. Its lubricating properties make it a staple in clinical practice, particularly as a lubricant for various invasive procedures. In the present authors’ experience, liquid paraffin is highly effective in softening and removing dirt, offering rapid action and significant efficacy. This results in reduced patient discomfort from repeated stimulation and contributes to more efficient nursing time management.
Povidone-iodine is composed of hydroxyl groups that denature bacterial proteins, along with iodine carriers capable of reacting with oxygen-containing functional groups. This interaction targets nucleotides, sulphur groups and fatty acids, leading to microbial eradication through oxidative action and inhibition of microbial protein synthesis. According to the US Centers for Disease Control and Prevention Surgical Site Infection Prevention Guidelines, both chlorhexidine and povidone-iodine are deemed appropriate for preoperative skin disinfection, effectively reducing the risk of surgical site infections. 6
The synergistic application of paraffin oil and povidone-iodine offers a comprehensive preoperative skin cleansing regimen (Figure 2). This combination not only ensures thorough decontamination but also plays a crucial role in infection prevention, enhancing patient safety in the perioperative period.
Presurgical image of a 15 cm × 10 cm soft mass in the right buttock of a Chinese male patient in his early 70s, showing meticulously cleaned and disinfected skin at the surgical site, adhering to established protocols to minimize the risk of infection and promote optimal surgical outcomes.
Surgery
The patient had a large tumour mass, so a simple excision and closure would result in high skin tension at the suture site, posing a challenge for postoperative wound healing. Therefore, based on thorough surgical planning, a ‘resection of the right buttocks pedunculated fibrolipoma and transfer of rhomboid flap’ was performed under lumbar anaesthesia. The L3/4 intervertebral space was selected for puncture. After local infiltration anaesthesia with 4 ml of 1% lidocaine, a single bolus injection of 0.5% ropivacaine, 2.4 ml, was administered into the subarachnoid space. The entire anaesthesia treatment lasted for 4 h. A rhomboid excision area was designed centred around the flat-shaped mass on the right buttock. First, a fusiform incision was made along the skin mass on the right buttock, reaching the subfascial layer. The skin mass was then completely excised, along with the subcutaneous lipoma, ensuring haemostasis. Next, a rhomboid skin flap was created below the lesion, with each angle measuring 60 degrees. Following the predetermined lines, the skin and subcutaneous tissue was incised, reaching the fascial layer. The full-thickness rhomboid flap and subcutaneous tissue was meticulously dissected, achieving haemostasis by electrocautery (using Peng's Multifunctional Operative Dissector; Zhejiang Shuyou Surgical Instrument Co., Ltd, Zhejiang, China). The flap closure was tension-free, secured with interrupted 2/0 prolene sutures. The surgery lasted a total of 1 h and 5 min without complications, and was well-tolerated by the patient (Figure 3 and 4). Postoperative pathology confirmed fibrolipoma (Figure 5), characterized by the presence of both mature adipose tissue and fibrous connective tissue. Key histological features included mature adipocytes, fibrous connective tissue with a significant amount of fibrous tissue interspersed among the adipocytes giving the tumour a firmer consistency compared with a typical lipoma, and lobular architecture, with fibrous septa dividing the adipose tissue into lobules.

Postsurgical image of the right buttock of a Chinese male patient in his early 70s, showing the incision after completion of surgery to remove a 15 cm × 10 cm soft mass.

Postsurgical image of the right buttock of a Chinese male patient in his early 70s, showing the incision after completion of surgery to remove a 15 cm × 10 cm soft mass.

Pathology photomicrograph showing haematoxylin and eosin-stained section of excised tissue from a 15 cm × 10 cm soft mass in the right buttock of a Chinese male patient in his early 70s, confirming fibrolipoma (original magnification, × 100).
Nutritional diet and home care services after discharge
During the postoperative recovery period, a reasonable nutritional plan was devised for the patient, which included starting a regular diet on the day after surgery. The patient followed a three-meal-a-day routine, focusing on foods rich in protein and vitamins, and low in fat, according to the following recommendations: wholemeal bread, hard-boiled eggs, milk and fruit for breakfast; chicken breast, vegetables, rice or noodles for lunch; and fish, vegetables, rice and fruit for dinner.
The patient was discharged after 7 days of hospitalization. Because the patient lived 11 kilometres away from the hospital, to reduce the cost of returning the patient to hospital for dressing change and review, the attending doctor and the nurse kept in close contact with the patient and provided continuous home care. After discharge, the incision dressing was changed every 2 days until the incision was basically dry and clean, and this process lasted for 2 weeks after the operation. On-site dressing changes were then performed, with follow-up every 4–5 days until the incision was completely crusted and healed, and this process continued until 5 weeks after surgery. The patient was then visited every week for follow-up review. From surgery, wound healing took 7 weeks to complete. At the last follow-up visit at 5 months after surgery, the patient’s incision was examined and no signs of infection or recurrence were found. The patient and their family expressed high satisfaction with the treatment (Figures 6, 7 and 8).

Image showing healing of postsurgical wound during home care at 2 weeks following surgery to remove a 15 cm × 10 cm soft mass in the right buttock of a Chinese male patient in his early 70s.

Image showing healing of postsurgical wound during home care at 5 weeks following surgery to remove a 15 cm × 10 cm soft mass in the right buttock of a Chinese male patient in his early 70s.

Image showing healing of wound during home care at 4 months following surgery to remove a 15 cm × 10 cm soft mass in the right buttock of a Chinese male patient in his early 70s.
Written informed consent was obtained from the patient for the publication of this case report. The study was approved by the institutional Review Board of Ningbo Beilun Third People’s Hospital. All methods were performed in accordance with relevant guidelines and regulations, and the reporting of this study conforms to CARE guidelines. 7
Discussion
Lipomas, the most common benign neoplasms of mesenchymal origin, may arise in any region of the body where fat is present.5,6 These well-differentiated neoplasms are composed of adult adipocytes encased within a fibrous capsule. The clinical manifestations of lipomas vary depending on their location, size, growth rate, and the degree of compression exerted on adjacent structures. Typically, a lipoma presents as a painless, well-circumscribed mass that gradually enlarges over time. 8
As a solitary variant of Nevus lipomatosus cutaneous superficialis, pedunculated lipofibromas are benign proliferations of connective tissue that often arise from ectopic adipose tissue. Typically, lipofibromas appear as large, solitary, slow-growing, skin-coloured, compressible, pedunculated, or dome-shaped nodules or plaques. Most commonly, these lesions appear on the buttocks, upper thighs, and non-pelvic areas, such as the axillae, arms, knees, ears, and scalp. 4 In 1975, Mehergan et al. introduced the term ‘pedunculated lipofibroma’ due to its unique clinicopathological characteristics. 9 The aetiology of pedunculated lipofibroma remains uncertain, with theories suggesting that adipose tissue deposition in the dermis may result from degeneration of dermal collagen and elastic tissue, subcutaneous adipose tissue then migrates into the dermis, and dermal vessels differentiate. 9
Fibrolipomas are typically non-pedunculated. However, there have been a few reported cases of pedunculated fibrolipomas in the literature, varying in size and location. The smallest documented pedunculated fibrolipoma originated from the buccal mucosa, measuring 0.4 cm. 1 In contrast, the largest reported pedunculated fibrolipoma was situated in the facial and neck region, involving the cervical sheath, submandibular gland, and buccal fat pad; it measured a staggering 45 × 40 × 46 cm and weighed 6 kg. 10 Additionally, two other reported cases of pedunculated fibrolipomas were situated in the vulva and on the plantar surface of the oesophagus.11,12 However, no relevant literature was found regarding age and gender differences in the pathogenesis of the disease.
Clinically, pedunculated lipofibroma is categorized into two types: classical and solitary. The classical type is typically found in the gluteal region, pelvic or upper thigh areas, and lower back, and may be present at birth or develop before the age of 20. It is characterized by a zonal pattern of multiple, non-tender, soft, pedunculated, skin-coloured, or yellow nodules, papules, or plaques. The solitary type, on the other hand, appears as a single papule and can be located anywhere on the skin. 13
Clinically, pedunculated lipofibromas may be mistaken for other benign papillomas, such as acrochordons, seborrheic keratoses, nevocellular nevi, verrucae, neurofibromas, fibroepithelioma of Pinkus, or eccrine poroma. However, they are histologically distinct, characterized by isolated clusters of ectopic mature adipocytes within the reticular dermis. 4 Although pedunculated fibrolipomas are not life-threatening, they can ulcerate or lead to functional inconveniences. Consequently, surgical excision remains the definitive treatment. 5
In the present case, the patient’s hip mass, with a convoluted surface appearance, remained asymptomatic without pain or itching, leading to the patient’s disregard for its removal over a period of 50 years. This underscores the importance of psychological care in managing such patients. The attending physician and nurse formulated an optimal treatment plan and employed the ‘sandwich’ communication method to effectively engage and educate the patient. This strategy not only fortified the patient’s confidence and enhanced their positive perception of the condition, but also contributed to reduced anxiety, increased self-assurance, and improved wound healing outcomes.
Preoperatively, the application of paraffin oil and iodophor-soaked cotton balls minimized skin irritation, ensuring comprehensive skin cleansing and disinfection, thereby diminishing the risk of intraoperative infection. During the surgery, considering the large area of the patient’s skin tumour, simple excision would result in high skin tension, making postoperative healing difficult. Therefore, a ‘rhombic flap transfer’ was designed to reduce postoperative skin tension and promote incision healing. Additionally, the soft tissue was thoroughly excised above the fascial layer to prevent recurrence. After tumour excision, an electric knife was used to perform thorough electrocoagulation haemostasis on the wound surface to prevent postoperative haematoma and seroma, which may affect incision healing. Postoperatively, the home care service played a pivotal role in monitoring wound healing and managing dressing changes, aligning with the patient’s needs and adding convenience to their recovery process.
Conclusions
For pedunculated fibrolipomas with extensive growth over a prolonged period, systematic communication and treatment are paramount. In the present case, following a comprehensive approach, the patient’s wound healed entirely without complications. The patient expressed high satisfaction with the treatment outcome, lending credibility to the management strategies employed for such conditions in the future.
Footnotes
Acknowledgements
I would like to express my gratitude to all those who helped me during the writing of this article.
Author contributions
Yi Jin: conceptualization, data collection and analysis, and writing of first draft; Jianmin Li and Jiansong Tang: material preparation, data collection and analysis; Zhuoyin Wang: manuscript review and editing, and study supervision. All authors read and approved the final manuscript.
Data availability statement
All data generated or analysed during this study are included within this published article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.