
Abstract
Objective
To investigate the effect of hospital working hours on outcomes of patients with acute ischemic stroke 3 months after receiving alteplase intravenous thrombolysis.
Methods
A retrospective analysis was performed on 254 individuals with acute ischemic stroke who received alteplase intravenous thrombolysis between January 2018 and December 2020 either during peak hospital working hours (08:00–17:59; Group A) or off-peak hours (18:00–07:59 the following day; Group B). Patients were also categorized according to which of four peak/off-peak-hour periods they received treatment in: Group 1 (08:00–11:59), Group 2 (12:00–17:59), Group 3 (18:00–21:59), Group 4 (22:00–07:59 the following day). Baseline data and 3-month prognosis were compared across groups. Logistic regression analysis was used to investigate the correlation between hospital working hours and 3-month prognosis.
Results
There were no significant differences in door-to-needle time, onset-to-needle time, 24-hour National Institutes of Health Stroke Scale (NIHSS) score, 7-day NIHSS score or Modified Rankin Score between Groups 1 to 4 or between Groups A and B. Whether treatment was administered during peak or off-peak hours did not significantly affect 3-month prognosis.
Conclusion
At this hospital, differences in the time at which stroke patients were treated were not associated with outcomes.
Keywords
Introduction
Ischemic stroke is responsible for 60% to 80% of all strokes and has a high death and disability rate.1–3 Administering alteplase intravenous thrombolytic therapy within 4.5 hours of stroke onset is an effective method that may considerably reduce stroke mortality and disability rates. 4 However, the beneficial effects of intravenous thrombolytic treatment are time-dependent. The standard for alteplase intravenous thrombolysis is that it should be performed within 4.5 hours of stroke onset. Only 1.6% of Chinese patients with acute ischemic stroke meet the criteria for intravenous thrombolytic therapy, and only 22% of these patients are admitted to hospital within 3 hours of stroke onset. 5 Given the strict time limits for administration of intravenous thrombolysis, it is essential to thoroughly investigate and address the factors that contribute to a lengthy time interval between symptom onset and the initiation of infusion to ensure favorable therapy outcomes in acute ischemic stroke patients.
Onset-to-needle time (ONT) is the time from disease onset to the initiation of intravenous thrombolysis. Door-to-needle time (DNT) is the time from hospital admission to initiation of intravenous thrombolytic therapy, which is the first stage of in-hospital treatment for acute ischemic stroke patients. Hospital delays are the main cause of extended DNT times. 6 Several factors can contribute to such delays, including complicated hospital treatment protocols, slow decision-making of patients and their families and insufficient stroke-related expertise of medical personnel. Acute ischemic stroke can occur unexpectedly, and there are no reliable models that predict onset time, making it difficult to determine when patients should seek medical attention.7–11 There are substantial operational differences between Chinese medical facilities, and hospitals in different areas vary in their staff and equipment ratios. Hospitals in China generally have adequate personnel and are very busy; all departments typically operate from 08:00 to 17:59, and equipment may be used extensively. The number of medical staff members in each department during off-peak hours (18:00–07:59 the following day) is very low; at such times, the staff are very busy, there is a shortage of senior experts with skills and there is limited access to tools and equipment.12–13 Furthermore, general hospitals treat a wide range of patients, not only those with stroke. There is considerable variation in the number of patients seeking therapy during different periods, with substantial spikes and decreases in treatment demand. All these factors can affect the level of work effectiveness. One real-world investigation showed that stroke onset in approximately half of patients with acute pro-circulatory large vascular occlusive stroke occurred during off-peak hours. 14 However, there may be differences in the course of treatment for stroke depending on whether treatment was given in peak hospital working hours (08:00–17:59) or off-peak working hours (18:00–07:59 the following day). Medical institutions should implement strategies to minimize in-hospital delays by establishing stroke green lanes and employing dedicated neuro-emergency physicians. However, there is no consistent consensus regarding prognostic disparities between peak and off-peak hours.
A literature search identified a lack of real-world research comparing the effects of alteplase intravenous thrombolytic therapy administered during peak vs. off-peak hospital working hours. In addition, there are no reports on the treatment of patients during peak hours and subsequent outcomes of alteplase intravenous thrombolytic therapy. Hence, the objective of this study was to examine the effect of working hours on the outcome of alteplase intravenous thrombolysis in individuals with acute ischemic stroke.
Data and methods
Study participants and setting
A retrospective analysis was conducted on data for patients who had experienced ischemic stroke and were treated with intravenous thrombolytic therapy at the neurological emergency department of the People’s Hospital of Deyang City, China, a large tertiary hospital, between January 2018 and December 2020. The study included patients who met the inclusion criteria throughout the entire period. The reporting of this study adheres to the STROBE criteria. 15
Inclusion criteria: (1) Diagnosis of acute ischemic stroke. (2) Alteplase intravenous thrombolysis indication. (3) Time from onset to treatment of less than 4.5 hours. (4) Aged 18 years or above.
Exclusion criteria: (1) Patients with alteplase intravenous thrombolysis contraindications. (2) Patients with incomplete clinical data or life expectancy of less than 3 months. (3) Occurrence of stroke in hospital. (4) Patients with tumors, rheumatic immune system disease or severe cardiac, liver or renal insufficiency.
Ethical approval
Informed consent was waived by our institutional review board because of the retrospective nature of the study.
Collection of clinical baseline data
The baseline data obtained comprised the patient’s age, sex, weight, history (including hypertension, diabetes, hyperlipidemia, atrial fibrillation, coronary heart disease, congestive heart failure history), smoking history, baseline systolic blood pressure, baseline diastolic blood pressure, baseline National Institutes of Health Stroke Scale (NIHSS) score, 4 24-hour NIHSS score, 7-day NIHSS score, baseline Modified Rankin Score (mRS), 16 3-month mRS, ONT, time of admission, DNT, baseline blood glucose level, white blood cell count, red blood cell count, neutrophil ratio, hemoglobin level, platelet count, prothrombin time, activated partial thromboplastin time, international normalized ratio, and levels of fibrinogen, D-dimer, sodium, potassium and urea nitrogen. All blood samples were taken before the start of alteplase intravenous thrombolytic therapy but at the time of hospital admission. To fully protect patients’ identity, all patients were de-identified.
Intravenous thrombolysis
For intravenous thrombolysis, recombinant tissue plasminogen activator (Boehringer Ingelheim, Ingelheim, Germany) was used. The maximum dose of 90 mg was delivered at a dose of 0.9 mg/kg, with 10% administered intravenously in less than a minute and the remaining 90% administered via a micropump over 1 hour.
Grouping and observation indicators
Patients were categorized into two groups according to hospital working hours during the treatment period: Group A (08:00–17:59) for patients treated during peak hours, and Group B (18:00–07:59 the following day) for patients treated during off-peak hours. These two peak and off-peak periods characterize working hours in most hospitals in China. The number of patients receiving treatment between 08:00 and 11:59 was greater than the number of patients receiving treatment between 12:00 and 17:59. Therefore, patients were divided into four groups according to whether the hospital was operating at full capacity at the time of treatment: Group 1 (08:00–11:59), Group 2 (12:00–17:59), Group 3 (18:00–21:59) and Group 4 (22:00–07:59 the following day). The mRS at 3 months (mRS = 0, 1, 2, 3, 4, 5, 6; a score of 6 = death) was the primary outcome measure for this investigation. 17 Patients were categorized into two groups based on their mRS at 3 months: patients with a good prognosis (mRS ≤2) and those with a bad prognosis (mRS >2). The 24-hour NIHSS score and the 7-day NIHSS score were the secondary outcome measures.
Statistical methods
IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA) and R 4.3 (www.r-project.org) were used for statistical analysis. Normally distributed data were expressed as mean ± standard deviation. The t-test or one-way analysis of variance was used for between-group comparisons.
Non-parametric tests were used to assess the data distribution in terms of the median and upper and lower quartiles. The number of cases and percentages were used to characterize the binary classification data, and the χ2 test was used to compare groups. Independent variables with P-values of <0.05 in the univariate logistic regression analysis were included in the multivariate logistic regression analysis model. For the odds ratios and 95% confidence intervals, bilateral values of P < 0.05 were deemed statistically significant.
Results
Clinical characteristics of study participants
Of the 254 patients, 154 (60.39%) were men and 100 (39.22%) were women. The median age was 69 years, with a range of 60 to 78 years. The median DNT was 62.00 minutes, with a range of 48.00 to 84.00 minutes. The median ONT was 147.50 minutes, with a range of 120.00 to 192.00 minutes. The number of patients in Groups 1, 2, 3 and 4 were 34 (13.33%), 71 (27.84%), 88 (34.51%) and 61 (23.92%), respectively. There were 34 patients (13.33%) in Group B and 220 (86.27%) in Group A. Of the total patients, 112 (43.92%) had a poor prognosis and 142 (55.69%) had a good prognosis (Table 1).
Clinical characteristics of study participants.
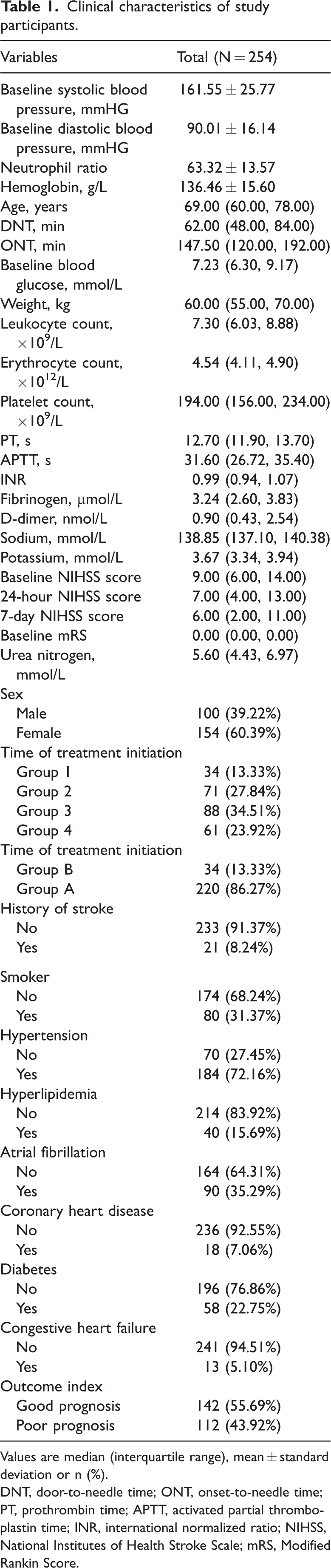
Values are median (interquartile range), mean ± standard deviation or n (%).
DNT, door-to-needle time; ONT, onset-to-needle time; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; NIHSS, National Institutes of Health Stroke Scale; mRS, Modified Rankin Score.
Comparison of clinical characteristics of patients in different treatment periods
There were significant differences in age, fibrinogen level, potassium level, and presence of diabetes between patients treated in different time periods (P < 0.05). However, values for the outcome index (mRS), DNT, ONT, 24-hour NIHSS, and 7-day NIHSS did not differ significantly (Table 2).
Comparison of clinical characteristics of patients in different time periods.

Values are median (interquartile range), mean ± standard deviation or n (%).
DNT, door-to-needle time; ONT, onset-to-needle time; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; NIHSS, National Institutes of Health Stroke Scale; mRS, Modified Rankin Score.
Comparison of clinical features of patients treated in peak vs. off-peak hours
There were significant differences in the neutrophil ratio and baseline NIHSS scores between patients treated in peak hours and patients treated in off-peak hours (P < 0.05). However, mRS, DNT, ONT, 24-hour NIHSS and 7-day NIHSS scores were not significantly different between the two groups (Table 3).
Comparison of clinical features between patients treated in peak vs. off-peak hours.

Values are median (interquartile range), mean ± standard deviation or n (%).
DNT, door-to-needle time; ONT, onset-to-needle time; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; NIHSS, National Institutes of Health Stroke Scale; mRS, Modified Rankin Score.
Propensity score matching between peak vs. off-peak hours treatment groups
Table 3 clearly shows that there was a significant difference in baseline NIHSS scores between patients treated during peak hours compared with those treated in off-peak hours (P < 0.05). To mitigate the effect of baseline NIHSS score on the prognosis of patients following intravenous thrombolysis, a nearest matching method was used to pair 66 patients at a 1:1 matching ratio. After adjusting for confounding variables, the neutrophil ratio and baseline NIHSS scores of the two groups became equal. The statistical analysis indicated that there was no significant difference in the prognosis of the two groups after 3 months (χ2 = 1.538; Table 4).
Results of univariate logistic regression analysis of clinical features of the two patient groups after matching.

Values are median (interquartile range), mean ± standard deviation or n (%).
DNT, door-to-needle time; ONT, onset-to-needle time; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; NIHSS, National Institutes of Health Stroke Scale.
Relationships between peak vs. off-peak hours, specific peak/off-peak period and prognosis
The logistic regression analysis identified no significant correlation between treatment administration during peak vs. off-peak hours and treatment administration during four specific periods of peak/off-peak hours. Additionally, there was no association between these factors and the 3-month prognosis of acute ischemic stroke patients who received alteplase intravenous thrombolysis. However, after 3 months of treatment for acute ischemic stroke with alteplase intravenous thrombolysis, longer DNT (P < 0.05), higher 24-hour NIHSS score (P < 0.05), higher 7-day NIHSS score (P < 0.001), higher baseline systolic blood pressure (P < 0.05) and history of stroke (P < 0.05) were risk factors for a poor prognosis (Table 5).
Univariate and multivariate logistic regression analysis of peak vs. off-peak hours, four peak/off-peak periods and prognosis at 3 months.

SE, standard error; OR, odds ratio; CI, confidence interval; DNT, door-to-needle time; ONT, onset-to-needle time; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; NIHSS, National Institutes of Health Stroke Scale; mRS, Modified Rankin Score.
Discussion
Thrombolytic therapy is essential for improving the prognosis of individuals with acute ischemic stroke. However, data obtained from the Chinese National Stroke Registry Database shows that the thrombolytic rate of recombinant tissue-type plasminogen activator in Chinese patients with acute ischemic stroke is only 1.23%. This rate is substantially lower than that observed in industrialized countries in Europe and the USA.18,19 Similar studies have demonstrated that the main reason for inadequate and ineffective thrombolytic therapy in stroke patients is delayed medical treatment. 20 This delay is affected by three factors: patient delay, transport delay and in-hospital delay. However, it is difficult to achieve major improvements in patient and transport delays in a short timeframe.21–27 Therefore, it is important to increase the efficacy of intravenous thrombolysis treatment by examining the factors that contribute to hospital delays. Currently, both local and international guidelines and consensus strongly advocate for a DNT of less than 60 minutes. In China, the average DNT is 115 minutes, with less than 10% of cases meeting the optimum DNT criteria of less than 60 minutes.4,19
One study showed that individuals with acute ischemic stroke experienced an average duration of 3.7 hours between hospital presentation and receiving treatment, considerably more than 60 minutes. 28 If implementation of DNT is too slow, some patients who are eligible for thrombolysis within the designated time frame may not receive it. For example, if a patient arrives at the hospital close to the thrombolysis maximum time window (4.5 hours after onset) and has to wait for treatment, they may exceed the time limit and ultimately not be eligible for treatment. 29 However, it remains uncertain whether there is a correlation between the timing of patient admission and the prognosis of intravenous thrombolysis. Several studies indicate that ischemic stroke patients who receive treatment during the weekend are more prone to a negative prognosis; this is sometimes referred to as the “weekend effect.”30,31 However, an effect of weekend visits on the outcome of ischemic stroke patients has not been observed in other studies. The inconsistent results among studies could be attributed to differences in cultural and healthcare environments.32,33
Differences in country-specific and geographical factors contribute to variations in staffing levels across different medical institutions during different working hours. 34 There are fewer medical personnel on duty during off-peak hours, including weekends. This limited staffing may adversely affect work efficiency owing to increased workload. Research has indicated that patients who are admitted to hospitals on weekends may have a higher probability of experiencing negative outcomes. 35 This could be attributed to substandard care in weekend emergency departments, insufficient availability of imaging staff, longer transportation time for patients to reach the inpatient ward, lower ability to evaluate complications and reduced capacity of the hospital’s emergency response. A comprehensive study conducted in the UK found that patients with ischemic stroke who undergo intravenous thrombolysis on weekends and at night experience extended DNT. 36 In contrast, the prognosis, DNT and ONT of patients in the present study did not differ significantly according to whether treatment was administered during peak vs. off-peak hours. A possible factor contributing to this disparity is that the present data were from a prominent tertiary hospital, which has a team of trained neuro-emergency physicians and a stroke green channel. The hospital has skilled medical staff available 24/7 to provide a seamless thrombolytic process. The stroke green channel process ensures that after experiencing a stroke, a patient receives prompt and efficient care. Another possible explanation for this difference in study findings is that despite the reduced staff numbers, there are generally fewer patients to attend to during off-peak hours in hospitals in China, resulting in expedited emergency imaging procedures compared with peak hours.
Most hospitals have a surge in patient visits during both peak hours (08:00–17:59) and off-peak hours (18:00–07:59 the following day). For instance, the number of patient visits are highest during peak hours, specifically from 08:00 to 12:00 and 14:00 to 18:00, and lower during evening working hours (18:00–22:00). Theoretically, the increase in the average number of patients attended to by each medical staff member during these periods relative to other periods may result in delays in treatment. Several studies support this conclusion.37–39 The present findings showed that there were no significant differences in the prognosis, DNT and ONT of patients receiving intravenous thrombolysis at different times (08:00–11:59 vs. 12:00–17:59 vs. 18:00–21:59 vs. 22:00–07:59 the following day). This suggests that an increase in the number of stroke patients within a certain range would not affect the course of treatment or patient outcomes. The use of a green channel set up specifically for stroke treatment in the study hospital may explain this finding.
The green channel operates as follows: A neurologist is assigned to the emergency outpatient department 24/7. The emergency pre-examination triage nurse sends patients to the emergency rescue room, calls the emergency neurologist and identifies suspected cases of acute cerebral infarction. The nurse also ascertains the time of stroke onset or the time of the last observation of intact neurological function. The neurology department’s emergency physician immediately attends the patient’s bedside, completes an evaluation in 10 minutes, and administers emergency laboratory tests, head computed tomography (CT) scan, electrocardiogram and other examinations. The emergency department nurses communicate with the CT room, assist patients with the head CT examinations and help with peripheral blood glucose monitoring and the administration of a bedside electrocardiogram. The family members of patients who do not have bleeding (as determined by CT scan) are briefly informed about the intravenous thrombolytic treatment plan by the Department of Neurology emergency physicians, and sign a consent letter permitting the administration of intravenous thrombolytic therapy in the CT room.
Thus, patients admitted to medical facilities that have green channels and neurological emergency departments receive prompt, standardized care.
Conclusion
Overall, the study findings indicated that the time period during which treatment was administered did not have a significant effect on the prognosis of patients with acute ischemic stroke receiving intravenous thrombolysis. This lack of effect may be attributed to the existence of a stroke green channel and the availability of 24-hour open neurological emergency services. However, this was a retrospective study conducted at a single medical center; not all medical institutions have specialized neurological emergency and stroke green channels. Differences in the availability of such services may reduce the generalizability of the study findings. To improve the reliability of the results, additional studies are needed in other types of facilities to compare the effects of treatment time across different levels of care.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241271828 - Supplemental material for Effect of working hours on prognosis of acute ischemic stroke patients following alteplase intravenous thrombolysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605241271828 for Effect of working hours on prognosis of acute ischemic stroke patients following alteplase intravenous thrombolysis by JingDa Wang, XingYang Yi and Qian Mi in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241271828 - Supplemental material for Effect of working hours on prognosis of acute ischemic stroke patients following alteplase intravenous thrombolysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605241271828 for Effect of working hours on prognosis of acute ischemic stroke patients following alteplase intravenous thrombolysis by JingDa Wang, XingYang Yi and Qian Mi in Journal of International Medical Research
Footnotes
Acknowledgements
We express our gratitude to the patients for agreeing to the use of their medical data for scientific research.
Author contributions
All authors made substantial contributions to the conception and design of the study, data acquisition, data analysis and interpretation, and drafting of the article or critically revising it for important intellectual content. All authors approved the final version of the manuscript to be submitted.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.