
Abstract
Objective
This case–control study tested a crisis awareness-based chain warning management model for patients with difficulties cooperating with magnetic resonance imaging (MRI) examinations.
Methods
All participants experienced difficulties cooperating with MRI examinations and underwent cranial magnetic resonance spectroscopy (MRS) and MRI at the same hospital in China. The control group (n = 1233) underwent examinations from January to June 2023 and received routine nursing care (pre-examination safety notification, instructions on cooperating during the examination, post-examination observation). A crisis awareness chain warning management model was implemented for the intervention group (n = 1352), who underwent examinations from July to December 2023. The groups were compared on average time for examination completion, quality of care and occurrence of complications. Data were collected using a self-devised data collection form.
Results
The average length of time to complete MRS and MRI was shorter for intervention group patients than for control group patients. The intervention group showed better pre-examination preparation, examination success rate, image quality attainment rate, and one-time examination success rate, and lower incidence of examination-related complications.
Conclusion
This management model could increase MRI examination efficiency, improve quality of care, reduce complications and increase nurses’ understanding of nursing continuity and crisis awareness.
Keywords
Introduction
Magnetic resonance imaging (MRI) examinations have become indispensable in clinical practice because the technique permits multi-parameter, multi-angle and high-resolution imaging. MRI dynamic enhancement imaging involves the distribution of a contrast agent to the target organ via the blood. MRI imaging produces high-contrast images, and is essential to determine the presence of malignancies in tissues and organs. 1 However, the examination process is time-consuming and is conducted in closed and narrow spaces with high noise levels. Patients often lack understanding of the examination procedures and principles, resulting in negative emotions like anxiety and nervousness. In addition, factors such as illness can make it challenging for patients to cooperate fully during the examination, leading to interruptions or the need for repeated examinations. A model that increased quality of care could enhance patient satisfaction and improve the examination success rate.
Several precautions are necessary before patients undergo an MRI examination. These include scheduling a lengthy appointment, allowing for the extended metabolism time of the contrast agent post-examination, and an extended period of observations. These tasks require the collaboration of multiple healthcare professionals. 2 The chain nursing management system 3 advocates decomposing complex problems into modules, linking each module through chain management, and assigning tasks based on the abilities of nursing staff and the module they are assigned to. This approach aims to increase the likelihood of ensuring the smooth progress of each module, thereby enhancing the efficiency and quality of the examination process. Yuhong and Linyi 4 have proposed a chain nursing management system that connects prehospital services to shorten the duration of each stage, thereby reducing treatment time for patients with severe limb trauma. This approach aims to reduce rescue time and minimize postoperative complications. Crisis awareness5,6 is based on the risk management process, which involves continuous and cyclical management of risk before, during and after a crisis occurs. It categorizes the crisis event into four stages: reduction, preparation, reaction and recovery. This approach enhances readiness to cope with the crisis event and minimizes the impact and severity of unexpected events. Zhu et al. 7 constructed an early warning intervention model based on the 4 R Crisis Management Theory (which comprises reduction, readiness, response and recovery) to enhance the efficiency of emergency care and the resuscitation of emergency patients with thoracic trauma. They found that the model increased the efficiency of emergency medicine and the resuscitation success rate, reduced the occurrence of complications, and increased patients’ chances of survival and satisfaction with nursing care. In this study, we developed an early warning management model within a crisis awareness framework, integrated multidisciplinary personnel within the management system, implemented standardized training and assessed the effect of the model on MRI and magnetic resonance spectroscopy (MRS) outcomes.
Methods
Participants
Patients who underwent cranial MRI and MRS examinations at Beijing Tsinghua Changgung Hospital, China, from January to June 2023 comprised the control group. Patients who underwent cranial MRI and MRS examinations at Beijing Tsinghua Changgung Hospital from July to December 2023 comprised the intervention group. All data were collected using a self-devised data collection form. Written informed consent was provided by all patients or their families. This was a case–control study. The study was approved by the ethics committee of Beijing Tsinghua Changgung Hospital (approval number: 2022-012). The reporting of this study conforms to the CONSORT statement. 8 In error, the trial was not prospectively registered, but is now retrospectively registered in a research registry (Chinese Clinical Trial Registry; https://www.chictr.org.cn).
Inclusion and exclusion criteria
The inclusion criteria were as follows: patients who had undergone their first cranial MRI and MRS examinations in the last 2 years, aged 14 to 70 years, normal hearing, normal speech function and ability to engage in normal verbal communication.
The exclusion criteria were as follows: patients with serious heart, lung, kidney or other important organ dysfunction; critical illness; previous mental disorders or psychiatric disease; or incomplete clinical data.
Procedure
The control group received routine nursing, including safety notification before the examination, instructions on how to cooperate during the examination, and post-examination observation.
For the intervention group, the crisis awareness-based chain management early warning model was implemented. Details of this model are as follows.
Crisis reduction stage
A literature review was conducted to identify relevant literature. The medical records of patients with failed MRI examinations or poor examination results in 2022 were analyzed to determine possible reasons for examination failure or poor examination quality. The results showed that patients failed to cooperate with the examination because they did not understand the examination purpose and procedure, were afraid of being in a confined space during the examination, and experienced symptoms such as cognitive impairment and limb jitter.
Risk preparation stage
Establishment of a crisis awareness chain management team. The core of the team was the radiography department, with head nurses and clinicians from other departments as assistants. The different departments and staff with different roles undertook supervision and cooperated with each other.
Personnel training: The team members were required to regularly devise training and related assessment plans, and simultaneously carry out training and engage in group communication. The person in charge of each training session passed on one or two documents containing relevant information (e.g., on chain management, the risk management model, and analysis of reasons for unsuccessful examinations) to the working group once a week, each time. After reading the information, team members had to click a corresponding button (“Understand” or “Don’t Understand”), and the person in charge of each training session explained the information points that were not understood. Every week, outpatient and ward nurses received various types of training, such as training in the wards, scene drills and video information. Each training session lasted a maximum of half an hour. After completing the training, the nursing staff were assessed regularly, and were only permitted to take up their posts after passing the training.
Establishment of a standardized and homogeneous chain management system using screening and evaluation to prevent patients from failing MRI examinations. The standardized education process included the following.
Pre-examination preparation stage: Ward nurses and outpatient nurses must inform patients in advance to remove metallic foreign bodies and jewelry, clean their skin, remove traces of medicated plaster, and avoid cupping and other behaviors that may cause local skin congestion 1 week before the examination.
Preparation for examination: Imaging nurses familiarize patients with the MR room environment by showing them a short film before the examination. In addition, patients and their family members are permitted to visit the scanning room in advance if needed. Patients are informed that the MRI and MRS examinations are noisy and the space is confined. Some patients may experience irritability, involuntary movements and palpitations, especially in serious cases. Nurses must instruct patients to take deep breaths and redirect their attention to maintain a relaxed mood. For patients who require contrast enhancement, a thick, straight vein should be selected for puncture. Nurses should also confirm in advance whether any indwelling needles inserted in the ward are unobstructed.
Preparation during the examination: A comfortable environment is ensured by maintaining appropriate room temperature and humidity levels, appropriate lighting, cleanliness and quietness. Patients are allowed to close their eyes or wear an eye mask to reduce anxiety. Patients’ emotional and psychological changes are carefully observed so that they can be provided with support. If the situation permits, relatives are allowed to accompany patients to reduce psychological stress and increase patient cooperation. Nurses should ensure that patients’ privacy is protected, and should address any issues patients encounter in a comprehensive and confidential manner. Patients are advised to try to assume a relatively comfortable position to ensure that the quality of the examination is not compromised. For patients with lumbar disc herniation, it is necessary to elevate their lower limbs, place soft pillows under their knees and keep them in a supine position with knees bent. If necessary, patients are allowed to take a short break between exams to relax their muscles. During contrast enhancement procedures, it is important to slowly inject the contrast agent and instruct patients to take a deep breath to help stabilize their condition. In the event of any serious adverse reactions, the injection and examination should be terminated immediately. The doctor should be promptly notified, and the patient should receive timely treatment.
Post-examination guidance: The patient should be promptly removed from the examination area while maintaining venous access. Patients can rest in the lounge for more than 30 minutes accompanied by family members. Any needles will be subsequently removed and patients allowed to leave the observation area when they feel ready. If their condition allows, patients are advised to consume hot water to facilitate the excretion of contrast media.
Establishment of an risk early warning mechanism: We developed the Adult MRI Cooperation Examination Difficulty Assessment Scale by consulting relevant literature and experts. The scale is used by ward nurses to assess patients’ risk before each examination. If the risk of cooperation difficulties is higher than moderate, an early warning mechanism is initiated.
Risk response stage
An early warning system was developed and emergency plans distributed to all departments to ensure that medical and nursing staff were familiar with the contents of the plan and could promptly and effectively intervene if an early warning was issued. The early warning mechanism includes the following components.
Claustrophobia-susceptible patients Pre-examination preparation stage: Ward nurses and outpatient nurses inform patients and their families about the examination process and possible psychological reactions in advance using imaging data. They also assist them in preparing psychologically beforehand. Preparation for examination: Patients are allowed to visit the examination room environment in advance. The principle and safety of MRI and MRS examinations are explained to patients. Patients are allowed to close their eyes before the examination to reduce anxiety.
9
Preparation during the examination: Advance preparation of noise-canceling headphones can help to reduce the psychological effect of noise on patients. Patients’ family members are permitted to touch the patient’s limbs when necessary to make them feel more secure. Post-examination guidance: The patient’s condition is observed. The patient is allowed to rest in the designated area for at least 30 minutes until their vital signs stabilize before departing. Acute and critical patients Pre-examination preparation stage: Critical patients should be accompanied by clinicians and nurses, and should be accompanied by relevant medical supplies for the examination. Clinicians should inform patients and their families in advance of the potential consequences of the examination. Rescue vehicles and supplies should be prepared in advance, and medical staff who perform the imaging should receive regular training in rescue-related procedures. Preparation for examination: Nurses in the imaging department should promptly assess whether patients are accompanied by clinicians and nurses and whether patients are accompanied by rescue equipment that causes electromagnetic interference. When necessary, clinicians should provide manual monitoring and rescue support in the examination room as an alternative to the use of emergency monitoring facilities.
10
Patients who are unable to cooperate with the examination owing to factors such as restlessness, involuntary muscle tremors caused by Parkinson’s disease, or other reasons should receive appropriate sedation following evaluation by clinicians. Trauma patients, especially those with head and cervical injuries, should be guided and assisted by their families to ensure safe transportation and prevent secondary injuries. Preparation during the examination: The patient’s condition should be closely monitored through the observation window to minimize unnecessary examination procedures and shorten the examination time. If the condition changes, the examination should be promptly terminated, the imaging staff should collaborate with the clinician in resuscitation procedures and the relevant departments should be notified immediately. Post-examination guidance: Clinical medical staff should be assisted in communicating with patients’ families, documenting rescue efforts and transferring patients to clinical departments. Pre-examination preparation stage: The ward nurse/outpatient nurse evaluates the patient’s allergy history, renal function and other characteristics. Patients undergoing MRI and MRS examinations are given information about the process of injecting iodine contrast agents and potential adverse reactions, such as extravasation and allergies. In addition, information is provided about the emergency procedures that medical staff will follow in case of adverse reactions. Preparation for examination: The imaging nurse once again informs the patient of the risks associated with contrast agent injection and the emergency treatment options. A thick and straight vein is selected and punctured by experienced nurses to minimize the risk of contrast agent extravasation. Appropriate rescue materials are prepared in advance. Preparation during the examination: The patient’s condition is closely observed through the observation window. Prompt rescue is performed if an allergic reaction occurs. Post-examination guidance: After completion of the examination, the patient is observed while with their family for 30 minutes. Once the patient’s vital signs are stable and they are free of discomfort they are discharged. Patients are encouraged to drink plenty of water to facilitate the excretion of contrast media. A shift change meeting is conducted with clinical nurses to update them on the essential aspects of follow-up observation.
Risk recovery phase
The incidence of patients experiencing challenges cooperating with MRI and MRS examinations within a 3-day period are analyzed retrospectively. The plan-do-check-act method is used to examine the underlying causes of these challenges and the potential factors affecting their occurrence.
Observation indexes
The time taken for each patient to complete a cranial MRS and cranial MRI was recorded. Then, the average time taken to complete the MRS and MRI in the two patient groups was compared. The quality of care of patients in the two groups, including pre-examination preparation, examination success rate, image quality attainment rate and one-time examination success rate, were compared. Pre-examination preparation: Nursing preparation before the examination should fully meet the requirements of the examination. Preparation is considered satisfactory if the patient has received all the relevant information, the rescue facilities are comprehensive and ready for use, and the patient has been completely prepared in advance. Successful examination: The patient completes the MRI and MRS examinations. Image quality attainment rate: The image quality is of the required level if the key anatomical parts and details of the image obtained during the examination are clear and meet the standard for uploading. One-time examination success rate: The patient has successfully completed the examination at one time, without the need for a second examination. The occurrence of complications was recorded; these included claustrophobic episodes, contrast extravasation and fall/carrying injuries.
Statistical methods
All data were statistically analyzed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Data that conformed to a normal distribution are expressed as the mean (±standard deviation), whereas data that did not conform to a normal distribution are expressed as the median and interquartile range. Between-group comparisons were conducted using t-tests or Kruskal–Wallis tests. Count data are expressed as percentages (%) and were compared using the chi-square test. A statistical difference was considered significant when P < 0.05.
According to previous research results, the MRI failure rate is approximately 40% (incidence rate = 0.4). 13 The following formula was used to calculate the required sample size: N = Z1-α/22[p × (1 − p)]/e2, and Z = 1.960. The allowable error δ is 5%, so N = 369. Considering a rejection rate of 20%, a total sample size of 443 was needed.
Results
General data
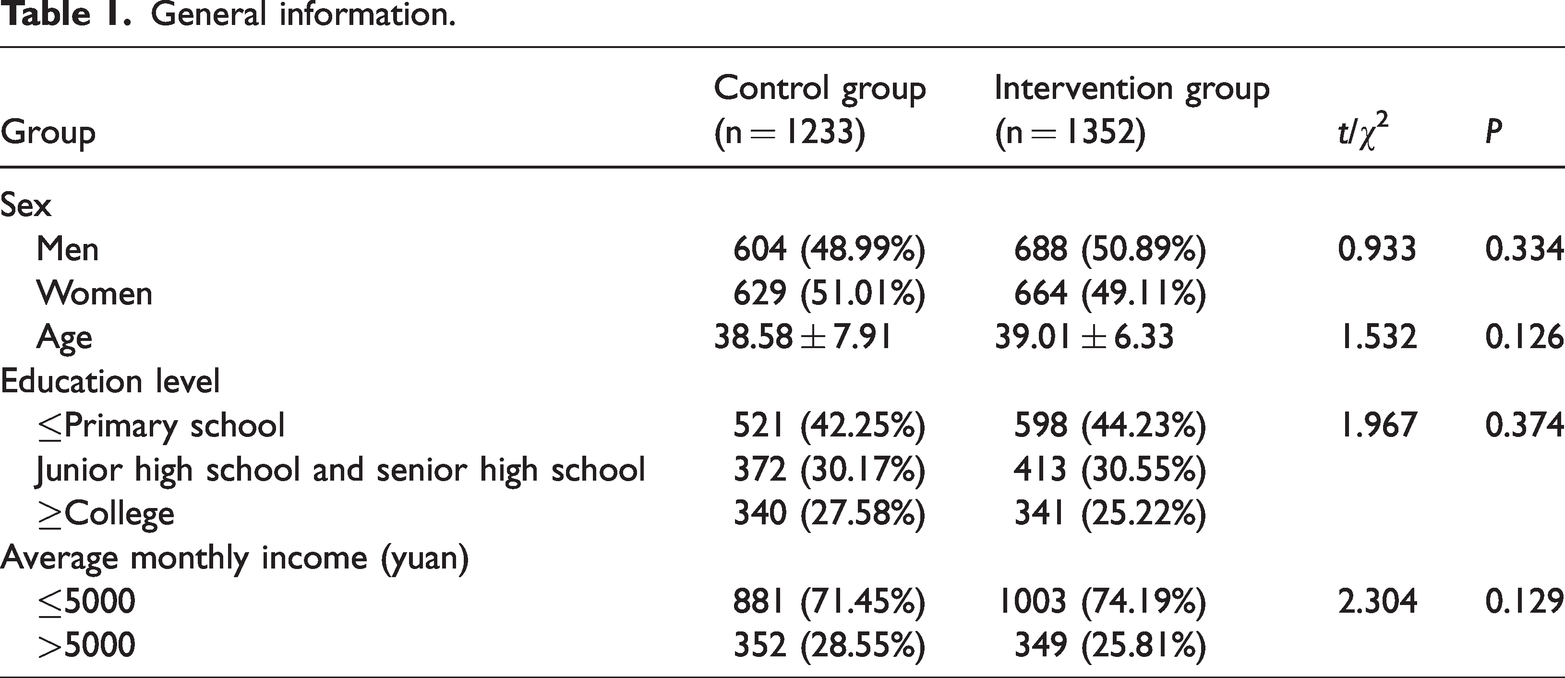
After excluding 148 patients with incomplete data, there were 1233 patients in the control group. After excluding 167 patients with incomplete data, there were 1352 patients in the intervention group. There was no statistical difference in general clinical data between the two groups. Detailed data are shown in Table 1.
General information.
Mean time taken to complete MRS and MRI
The average length of time taken to complete cranial MRS and MRI of patients in the intervention group was shorter than that of the control group (P < 0.05): MRS examination 13.76 ± 6.01 vs. 16.89 ± 5.34 (t = 13.944, P < 0.001); MRI examination 19.83 ± 5.47 vs. 23.14 ± 6.22 (t = 14.394, P < 0.001).
Quality of patient care
The pre-examination preparation, examination success rate, image quality attainment rate and one-time examination success rate of patients in the intervention group were better than those of patients in the control group (P < 0.05). Detailed data are shown in Table 2.
The quality of care of patients in the two groups.

*P < 0.05.
Occurrence of complications
The incidence of examination-related complications was lower for patients in the intervention group than for those in the control group (χ2 = 74.119, P < 0.05). Detailed data are shown in Table 3.
The occurrence of complications in the two groups.

*P < 0.05.
Discussion
Although MRI is a common non-invasive extracorporeal examination, it is noisy, and the examination environment is enclosed and cold. These factors, together with the effect of the patient’s disease and unfamiliarity with the examination process can easily lead to nervousness and anxiety. These feelings can trigger claustrophobia, involuntary trembling of the limbs, shortness of breath and other responses. Such reactions may affect the image quality, prolong the examination duration and even necessitate an interruption of the examination. 14 In the conventional care model, nursing staff can only advise patients on simple precautions before the examination and provide passive remedial care in case of emergencies. Some patients may require a follow-up examination, which can result in dissatisfaction among patients and their families. Therefore, the aim of this study was to develop a new nursing model that provides continuous nursing management before, during and after examinations to prevent potential adverse events. This approach aims to reduce the burden of caregiving and enhance the quality of care.
The results showed that the average time taken to complete the MRS and MRI was shorter for patients treated using the crisis awareness-based MRI chain warning management model than for patients in the control group. In addition, the examination readiness, examination success rate, examination image quality attainment rate and one-time examination success rate were better for intervention group patients than for control group patients. Moreover, the examination-related complication rate was lower in the intervention group than in the control group (P < 0.05). Possible reasons for these outcomes are as follows.
In the risk reduction stage of this study, data from patients who had experienced difficulties cooperating with MRI examinations in recent years were retrospectively analyzed to determine the possible risk factors that affected patients. Simultaneously, in accordance with crisis management theory and early warning model theory, our evaluation of changes in the team members indicated that the healthcare personnel gradually increased their awareness of the identification of risk factors and strengthened their risk assessment ability. In this study, a risk assessment team was formed during the risk preparation stage. The Adult MRI Cooperation Examination Difficulty Assessment Scale was developed to quickly and accurately predict the risk of potential examination cooperation difficulties among patients. This aim of this scale is to alert nursing staff to implement effective risk control measures based on the assessment results. The goal is to minimize harm to patients and increase nursing satisfaction. The chain nursing management system has been improved, standardized teaching and preparation processes have been established, nursing safety equipment has been upgraded, and standardized training and testing of relevant healthcare personnel have been strengthened. During the risk response stage, healthcare personnel improve their emergency response capabilities through emergency drills and other methods, with the aim of enabling them to promptly assess the patient’s condition following a risk event and promptly implement resuscitation measures. The goal is to minimize unnecessary harm to both the patient and the hospital. During the risk recovery stage, it is essential to promptly conduct a brainstorming session, summarize the experience, thoroughly analyze risk factors and management shortcomings, maintain the nursing system, optimize the management system and prevent similar events from recurring. These actions help to reduce the risk of adverse events and improve the emergency response capabilities of healthcare personnel. Jensen et al. 15 used simulation of crisis resource management to reconstruct the definition of various healthcare roles and communication styles, and to strengthen the team’s ability to work together. Such strategies can enhance the quality of care during the admission of critically ill patients.
The chain management approach 16 was initially used in business science in relation to the process and regularity of the development of materials. This management style is based on improving the market resilience of enterprises and satisfying customers’ needs in a timely manner. According to chain management theory, all participants should be constantly adjusted according to external conditions to form positive interactions and a virtuous circle among the elements. 17 The present study applied this theory to the field of medicine, focusing on problem-solving from multiple perspectives, including those of healthcare workers, patients, families and management processes. It integrated and established standardized and sequential workflows, and increased healthcare workers’ understanding of management processes using flowcharts and other methods. Using the chain nursing theory, this study elucidated the responsibilities of each department, and improved departmental collaboration by establishing effective multiparty communication pathways and conducting regular emergency drills. These measures ensure that the examination process is conducted smoothly. Xiang et al. 3 applied the chain management system to the emergency treatment of trauma patients. Their findings showed that clarifying the specifics of each step in the process can ensure its efficiency and continuity. Zhang et al. 18 have also shown that the chain nursing model is conducive to nurses’ standardized assessment and recording of pain in cancer patients.
The aim of early warning risk management is to establish a mechanism for early risk detection to identify patients who may face challenges cooperating with MRI scans. It enables personnel to proactively intervene with patients, make necessary emergency preparations and implement protective measures. This approach ensures a smooth and efficient examination process, minimizes examination time and enables continuous monitoring and control of patients’ vital signs. Ultimately, it aims to reduce the occurrence of adverse events during the examination. The anticipation and preparation for risky events helps to assure patients and their families that healthcare professionals have high levels of expertise and can confidently navigate the unfamiliar MRI examination process. MRI examinations can often be intimidating for patients, so this proactive approach increases patients’ trust in the hospital and their satisfaction with the quality of care provided. A environmental-based hierarchical prediction system developed by Teheux et al. 19 can facilitate the timely identification of risks at the early stage of abnormalities in infant vital signs. It enables faster detection of signs of clinical deterioration, increasing the possibility of early and timely intervention to reduce infant mortality. Sposito 20 demonstrated the importance of low-density lipoprotein receptor-1 (LOX-1) levels in predicting the recurrence of coronary events and cardiovascular mortality. Kraler et al. 21 showed that persistently high levels of sLOX-1 were associated with coronary plaque progression in patients with established atherosclerotic cardiovascular disease, during a 1-year follow-up of 2804 patients with acute coronary syndrome, highlighting the clinical importance of risk assessment.
Conclusion and limitations
This crisis awareness-based MRI chain warning management model can compensate for the limitations of the traditional MRI examination process, integrate and optimize departmental quality of care processes and interdepartmental coordination, improve the efficiency of the MRI examination, improve the quality of care during the examination and reduce the incidence of related complications. This management model shows promising clinical value.
This study was conducted in only one hospital, and the sample size was limited. Future research could extend this nursing model to multiple centers to strengthen the evidence of its effects. In this study, we focused on patient stress and risk factors that may arise during the examination process, and paid insufficient attention to the examination equipment and environment. The next stage of this research is to classify and compare the effect of different examination equipment on patient cooperation. For example, models of examination equipment may have different effects depending on factors such as the manufacturer, the Hertz frequency used by the equipment, and the noise level.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241266581 - Supplemental material for A crisis awareness chain warning management model for patients with difficulties cooperating with magnetic resonance examinations
Supplemental material, sj-pdf-1-imr-10.1177_03000605241266581 for A crisis awareness chain warning management model for patients with difficulties cooperating with magnetic resonance examinations by Dan Wang, Bicong Zhang, Hongliang Zhao, Yu Zhang and Meng Hou in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank our colleagues in the laboratory and all the individuals who helped and supported us during the process of completing this paper. They provided us with a substantial amount of research support.
Author contributions
Research concept and design: Dan Wang, Meng Hou; Data collection: Bicong Zhang; Investigation and Methodology: Hongliang Zhao; Validation: Yu Zhang; Drafting of the manuscript: Dan Wang; Making important revisions to the paper: Hongliang Zhao, Yu Zhang, Meng Hou; Approval of the final paper to be published: Dan Wang, Yu Zhang, Meng Hou.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.