
Abstract
Objective
Value-focused thinking (VFT) is a decision-making method that places the qualitative elicitation of decisionmakers’ objectives at the beginning of the decision-making process. A potential healthcare application of VFT is to elicit patients’ objectives to better understand what matters to them. Only then can treatments be tailored accordingly. This is particularly important for patients with life-threatening diseases such as cancer. Thus, this interview study used VFT to elicit the life and treatment objectives of non-terminal oncologic inpatients.
Methods
Fifteen cancer inpatients (median age 66 years) were sampled in a German university hospital in September 2019. The participants completed questionnaires, the data of which were used to semi-structure the subsequent interviews. Data were analysed using inductive category formation to identify objectives in the transcribed interviews.
Results
Sixteen objectives in five life domains (optimising physical wellbeing, optimising mental wellbeing, optimising personal life, optimising family life and optimising financial life) were identified.
Conclusion
Comparison of the findings with previous research indicated that VFT is a reliable approach to elicit patients’ objectives. The identified objectives could increase understanding of the outcomes that cancer inpatients care about.
Keywords
Introduction
Value-focused thinking (VFT) is a decision-making method developed by operations researcher and engineer R. L. Keeney. 1 The method provides decisionmakers with a step-by-step guide for the decision-making process. The first step in the VFT method is the qualitative identification of relevant objectives for the decision in question. Objectives are the sum of what matters to decisionmakers. They make explicit a decisionmaker’s values, defined as “the things we care about” in VFT, in a decision context. 1 VFT differentiates fundamental objectives from means objectives. Fundamental objectives are the ends that decisionmakers want to achieve and that need to be identified in the elicitation process. In contrast, the purpose of means objectives is to accomplish fundamental objectives. 2 VFT uses the “Why Is That Important?” fundamentality test to differentiate essentially important objectives (e.g., those that are fundamental) from auxiliary objectives (e.g., means). 3 An overview of key VFT terms is provided in Appendix A.
Compared with the elicitation of objectives via available decision alternatives, VFT has two advantages: the method identifies objectives that are otherwise missed, while also creating a superior objectives structure. 4 These characteristics may explain why the method has been used in diverse research areas. 5 In healthcare, VFT has been used to facilitate the design of rehabilitation facilities, 6 to assess how blockchain technology could be used in the Indian healthcare system 7 and to identify objectives for the use of big data analysis. 8
Another potential healthcare application of VFT is the elicitation of patients’ objectives in specific decision contexts. This could contribute to published qualitative research exploring what matters to patients. Such research includes studies by Lim et al., 9 who used photo elicitation in semi-structured interviews and grounded theory to examine the perspectives of a sample of patients with multiple chronic conditions. Saigal et al. 10 used interviews and agglomerative hierarchical clustering to identify relevant treatment aspects for patients with prostate cancer. The nominal group technique was used by Col et al. 11 to elicit the treatment goals of multiple sclerosis patients. The underlying aim of qualitative studies is to obtain an unfiltered insight into the realities of patients, thus capturing relevant aspects of experience. Or as Col et al. 11 state, “No amount of finesse or mathematical sophistication in comparing items can compensate for choosing the wrong set of outcomes.”
Choosing irrelevant outcomes is particularly problematic for patients with life-threatening, chronic diseases such as cancer. Thus, research has explored what matters to patients with cancer. A detailed review of the values and needs of cancer patients was conducted by Mitchell et al. 12 Qualitative research has also explored oncologic survivorship goals 13 and the goals of non-curable cancer patients. 14 However, no studies have explored the life and treatment objectives of non-terminal oncologic inpatients using VFT.
The aim of this study was to use VFT in semi-structured interviews to elicit the life and treatment objectives of oncologic inpatients. It was hoped that this would test the method’s applicability to elicit patients’ objectives, and increase the understanding of the outcomes cancer inpatients care about.
Methods
The reporting of this semi-structured interview study follows the Standards for Reporting Qualitative Research guidelines. 15
During the study design phase and prior to field work, a questionnaire assessing five life domains (optimising physical wellbeing, optimising mental wellbeing, optimising personal life, optimising family life and optimising financial life) was developed (see Appendix B). The domains were chosen based on a literature search of studies on cancer patients’ values in treatment decision making. Broad and general domains were selected to ensure that patients would be able to contribute rich data regardless of their background or formal education. Patients’ responses were not restricted to the chosen life domains; patients were actively encouraged to voice any wishes and thoughts that lay outside these predefined areas, both in a dedicated questionnaire section and during interviews.
The questionnaire served three purposes. First, patients’ wishes, thoughts and statements recorded on the questionnaire were used as a semi-structured interview guide. Second, the questionnaire was used to create an individual wish list for each participant for the decision situation at hand (e.g., being treated for cancer). A wish list is a suggested method in the VFT approach to elicit a decisionmaker’s objectives; Keeney has described this method in detail. 1
Third, the questionnaire was intended to initiate reflection among participants about what mattered to them prior to the interviews, thus increasing the accessibility of patients’ values and objectives 16 and reducing clarification requests, which are a main determinant of interview length. 17 Shorter interviews were conducted to reduce the possibility of fatigue, which is often experienced by this population. 18
Data collection
Interviews took place during a 3-week period in September 2019. Approval to conduct the interviews was obtained from the University Hospital Aachen Ethics Committee (Reference: EK 225/19) in July 2019. Participating inpatients were treated on two wards at the University Hospital Aachen. Participation did not alter, delay or interfere with treatment. No financial or therapeutic benefits resulted from participation, nor did refusal to participate cause any disadvantages to patients. Inpatients were sampled using purposive sampling. Sex ratio and age distribution were taken into account to ensure sample representativeness. The inclusion criteria for participation were presence of a non-terminal oncologic illness (including both solid and liquid tumours) and patient circumstances (e.g., if the patient’s health condition and treatment made the interview possible). An age cut-off for participants was not established.
Ward physicians informed eligible patients about the ongoing study. Patients willing to participate were then approached by the first author, who provided further instructions. Both written and oral consent for participation were obtained from each participant. During this first encounter, questionnaires were distributed to patients, who were given a reasonable amount of time to complete the questionnaire. After questionnaire completion, interviews took place on the same day. The interviews were conducted by the second author, who is an experienced user of VFT and its techniques (e.g., the “Why Is That Important?” test) in different research areas. Interviews were conducted on the assumption that the overall fundamental objective 1 of patients is to “get well.” Interviewing thus focused on what facilitated this for patients.
Interviews were recorded using a digital audio-recorder. Two researchers, the first and second authors, were present during the interviews. The interviews were semi-structured and took place in patients’ rooms or lounges to ensure privacy and a quiet and comfortable atmosphere. The interviewer read out the wishes, thoughts and statements that the patient had written down in the questionnaire and encouraged the patient to elaborate on them. The “Why Is That Important?” test was repeatedly used to differentiate patients’ fundamental objectives from their means objectives. The concept of data saturation 19 was used to determine the number of interviews conducted.
Data analysis
Recorded interviews were transcribed verbatim by the first author. At this stage, all patient details were deidentified. The audio files were deleted after the transcription, according to European data protection laws. Data analysis was performed by the first and third authors, who used inductive category formation 20 to identify recurring themes (i.e., objectives) in the transcripts. Any remarks or statements from patients’ relatives that were recorded in the transcripts were not considered. Category formation comprised two steps. Initially, the first and third authors independently coded all the interview transcripts using individual codes. Each code was allocated to one of the five life domains, resulting in two individual codebooks. After this initial round of coding, a research group meeting was held that included non-coding members. During this meeting the two unique codebooks were merged into one final codebook. The categories in the final codebook were formulated as proposed by Keeney in terms of an object and a direction of preference. 1
The same two researchers then used the final codebook in a second independent coding round to match transcript passages to categories. Codes were then compared. Any mismatches were discussed by the two coders, and the reasoning behind the chosen category was stated. The disagreement was resolved by the two researchers unanimously selecting a code. Cohen’s kappa (κ) was calculated using the number of matching and divergent codes in the second coding round to determine interrater reliability using the cut-off values provided by Landis and Koch. 21
Microsoft Excel® and Access® were used for data analysis. German transcript passages intended for inclusion in this research paper were translated using DeepL, Version 1.11.0 (DeepL GmbH, Cologne, Germany).
Results
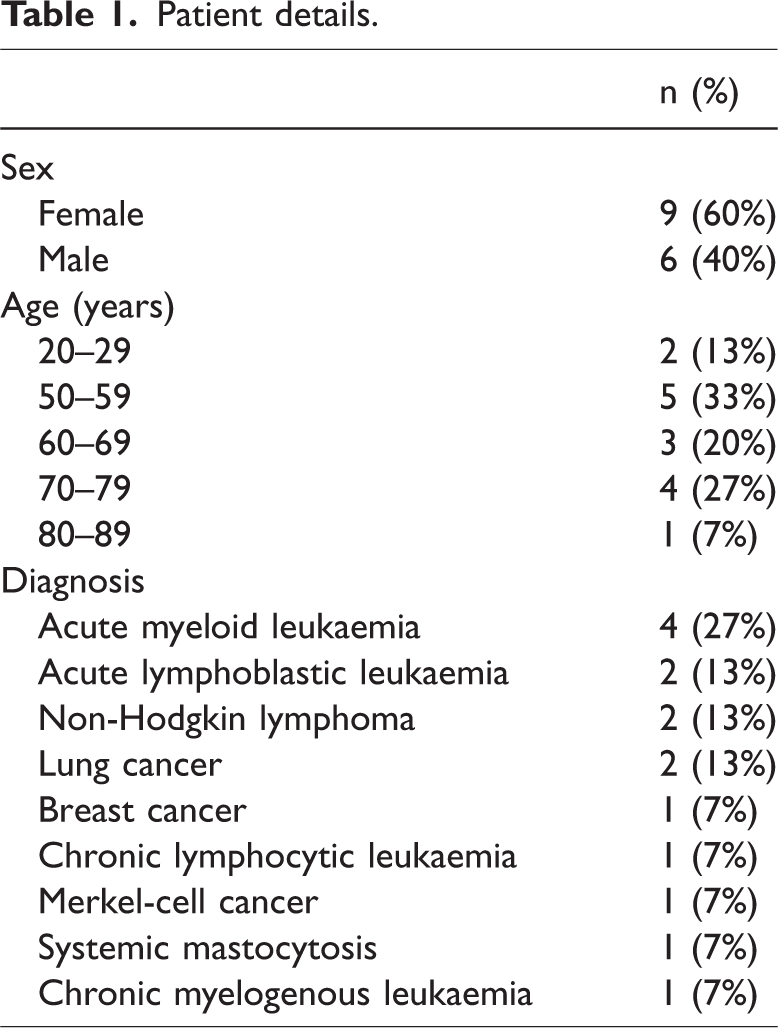
Sixteen inpatients were sampled for interviewing. One sampled patient was diagnosed with a non-oncologic illness after interviewing took place and was thus excluded from data analysis for not meeting the inclusion criteria. The remaining 15 inpatients were aged between 20 and 80 years (median: 66 years) and comprised nine women (60%) and six men (40%). Patient details are shown in Table 1. Interviews lasted between 10 and 33 minutes (median: 19.5 minutes).
Patient details.
Patients reported no issues or misunderstandings about the questionnaire they were asked to complete before the interviews. All objectives mentioned by participants in the relevant questionnaire section and in the interviews were covered by the life domains chosen by the research team.
Data analysis using inductive category formation identified 16 recurring fundamental life and treatment objectives voiced by oncologic inpatients. The Cohen’s kappa (κ) coefficient for intercoder agreement during the second round of coding using the final codebook was 0.71, which indicates substantial interrater agreement. 21
The identified objectives in each of the five life domains are discussed in detail below. A summary of the findings is presented in Table 2.
Framework of cancer inpatients’ treatment and life objectives and corresponding life domains

“Fundamental objectives” are the ends that decisionmakers want to achieve. The purpose of “means objectives” is to accomplish fundamental objectives.
AML, acute myeloid leukaemia; ALL, acute lymphoblastic leukaemia; NHL, non-Hodgkin lymphoma; CLL, chronic lymphocytic leukaemia; CML, chronic myelogenous leukaemia.
Optimising physical wellbeing
Patients reported negative effects on their mobility and quality of life owing to their health condition or treatment: “(…) I sometimes felt like a 100-year-old grandpa, I’d say. The power is gone.” Patient F, 53, male, acute myeloid leukaemia (AML)
Consequently, an objective that was frequently expressed by patients was to regain their physical strength over time.
Another need that was identified in relation to physical wellbeing was to feel clean. This was particularly expressed by participants who were temporarily unable to independently tend to their personal hygiene owing to sickness and/or treatment.
Patients also expressed a wish to limit disturbances while in hospital. One such disturbance that was frequently mentioned was noise during the night caused by factors such as alarms from treatment devices in the rooms and staff working in the corridors. Patient: “(…) I need to sleep. But when it’s loud here, I can't sleep. If it’s very loud in the corridor here.” Patient O, 68, male, lung cancer
Patients also considered the lack of personal privacy on the ward to be disruptive and repeatedly mentioned this during interviews with the research team. The issue was especially problematic in patients’ rooms, which they felt provided little opportunity for quiet retreat. Although patients acknowledged the difficulties of providing full privacy in a medical treatment facility, this was something that affected their hospital stays: “(…) You have a life somewhere. Sometimes you have to arrange things, or someone calls. Then I'm on the phone with my son, for example. But you know that your roommate is listening. Then you’re a bit guarded, I’d say. (…)” Patient D, 55, male, AML
Many participants expressed a wish to reduce treatment and illness-related symptoms and other associated factors that negatively affected their physical wellbeing.
Issues frequently brought up by interviewees in this context were gastrointestinal symptoms, such as vomiting and nausea, and pain. Other patients were worried about the consequences of diagnosis and treatments on their mental abilities. One interviewed patient reported his experiences in connection with nausea: “(…) When I brush my teeth or just rinse my mouth, for example, I have to retch. And you can’t eat feeling like that. (…)” Patient L, 79, male, lung cancer
Optimising mental wellbeing
Many patients regarded self-determination as essential to their mental wellbeing. This was understood differently by patients. For some, being self-determined meant freedom to choose how they spent their time in hospital and to plan the day according to their needs. For others, self-determination was associated with decision making and having a voice during their hospital stay: “Well, I have to say, they really do cater to the patient here. When you say, ‘I want it like this and that,’ then … yes, it will be done. Well, I can’t complain about that right now. (…)” Patient C, 53, female, AML
Another important aspect was a comfortable hospital atmosphere. For some patients, that meant clean and tidy surroundings. For others, personal interactions were considered essential to a pleasant ambience. One patient elaborated on this, explaining that for her, a good atmosphere meant being treated normally by friends and relatives during their visits: “(…) But just like before is best. Talking about their own problems or something. Because a lot of people think that they can’t tell me about their experiences or their problems anymore just because I’m here now. (…) I tell everyone again and again: ‘Treat me the same way as before! Because I haven’t changed that much.’” Patient A, 25, female, acute lymphoblastic leukaemia (ALL)
The way in which information was shared, specifically examination and blood test results, and the type of communication experienced during stays was also of concern. Completeness and speed were repeatedly mentioned as important to information sharing. As well as prompt communication of results, patients wanted medical professionals to explain what their results meant and possible consequences. “It’s the same with these haemoglobin levels. ‘Your haemoglobin was 7.1 today.’ Is that good? ls it not?” Patient D, 55, male, AML
Communication was not limited to exchanges between patients and healthcare experts. Some participants wanted medical professionals to communicate well with each other and even with relatives. Another aspect of communication mentioned by patients was a desire for transparent communication from healthcare workers during treatment. One patient described an examination situation in which the healthcare professionals who performed the examination provided little explanation. Another stated a wish to be present when important decisions were made: “(…) when they talk about you or whatever, that I witness it. Otherwise, I feel like ‘What's going on?’” Patient N, 77, female, breast cancer
Patients also wanted to be sure that they were receiving the “right” medical care. It was important to some that their treatment was managed by well-trained medical professionals using the most up-to-date equipment and pharmaceuticals. For others, confidence in treatment meant being taken care of and that their medical histories were known: “(…) I’m glad I came here because they have all my records and really care.” Patient L, 79, male, lung cancer
Patients frequently associated the “right” medical care with treatment outcomes, especially success rates and life expectancy. Also of importance was that complications during treatment would be detected quickly and that the correct measures would be taken accordingly.
Optimising personal life
Patients frequently expressed a desire to spend as much time as possible outside of medical facilities. Many patients had already spent a considerable amount of time in various institutions, both for treatment and rehabilitation. For some participants, hospitals were associated with disease and being sick, so they wished to return to familiar surroundings. When asked why being at home was so important, one patient replied as follows: “(…) Well, I just think that where you feel comfortable you are automatically happier and more positive. You find it easier to be positive. Or you need less energy for it. Instead of being suddenly here, and everything is new, and you feel somehow … well it’s not as if it’s so terrible here, but you just feel different and not as comfortable as at home. And then it just takes more energy to motivate yourself every day.” Patient A, 25, female, ALL
Patients also sought to regain control of their private lives. In contrast to self-determination in relation to mental wellbeing, this objective was more about life outside the medical treatment facility, a life that still existed, but had been somewhat interrupted by treatment: “(…) You had a life. Or have. And that is now suddenly over. Well, not over, but still very restricted, I’d say. And it is important that you can look after it, right? (…)” Patient D, 55, male, AML
For some participants, this also involved being able to plan into the future. Frequently mentioned in this context were trips and holidays that patients wanted to take when they no longer had to attend medical appointments. Participants also longed for some kind of normality. They wanted to return to the life they had before they became ill. As one participant expressed it, this meant having a private life that included a variety of activities and fewer constraints: “(…) That everything will be like before, that you can … just do more with friends again … sport … study. Just move forward again, not stupidly sit through the time without anything happening.” Patient J, 20, female, ALL
Participants told the research team that maintaining relationships with relatives and friends during treatment was sometimes difficult. One spoke of the mental burden of being unable to meet up with her young relatives owing to the potential risks she would be exposed to: “(…) Yes, I can see them [the grandchildren], but, like I said before, it’s a risk because of these childhood illnesses. And you know what kids are like: they come, they kiss, they kiss all the time … and if I don’t do that and just keep my distance, that’s not so good.” Patient E, 67, female, AML
Many leisure activities that brought patients joy and enriched their lives had to be avoided either because of illness or hospital treatment. This created a desire in patients to take up their previous activities again. Sport was one such leisure activity that some patients found it difficult to engage in: “(…) Let’s just say I enjoyed doing sports in the past. Loved to ride my bike. Swimming and going for walks and stuff. (…) and these are things that are very, very difficult for me now.” Patient H, 59, female, systemic mastocytosis
Optimising family life
Participants mentioned the effects of diagnosis and treatment on their families. They wished to be able to fulfil their family roles but being ill meant that they could not complete tasks that they usually performed. Therefore, responsibilities sometimes had to be temporarily transferred to relatives, leading some patients to question their role in the family: Interviewer: “But you feel your role as a wife, so to speak, that does all this …” Patient: “Useless.” Patient B, 66, female, chronic myelogenous leukaemia (CML) “(…) This is not only a difficult time for the patient personally, it is also a difficult time for everyone around him or her. And it makes you wonder, ‘Can they do it?’ Like, ‘Are they mentally strong enough to get through this?’” Patient A, 25, female, ALL
Optimising financial life
Under the healthcare system in Germany, hospital treatment was covered by patients’ healthcare insurance. However, they incurred other expenses. Some participants therefore expressed a wish that any additional costs would be low. Expenses mentioned by patients included parking fees, special ambulant treatment and medication expenses. “(…) Everything is always quite expensive in the pharmacy. The pharmaceuticals. I’ll see if I can somehow get a remission [of fees].” Patient B, 66, female, CML
Some patients had to take sick leave to receive hospital treatment. Although all participants received sick pay, some still experienced financial worries because of their situation. In particular, participants who were financially dependent on their jobs expressed a wish that treatment would not restrict their ability to work in the future: “(…) I’m too young to retire. And at my age, any disability pension I might get would be very … low, I think. That would also cause financial problems.” Patient F, 53, male, AML
Discussion
The purpose of this study was to elicit life and treatment objectives across five life domains of oncologic inpatients using the VFT decision-making approach.
VFT and the “Why Is That Important?” fundamentality test 1 was used to elicit oncologic inpatients’ objectives, thus adding to the growing number of VFT applications in healthcare.6–8 The objectives and goals of patients are receiving increasing attention, as shown by the development of a goal-based shared decision-making model. 22 Identifying patient objectives is essential in patient care in general. 23
The identified treatment and life objectives of oncologic inpatients captured what matters to these specific patients in their own language. Therefore, the findings contribute to qualitative research that uses alternative elicitation methods to explore what matters to specific patient groups.9–11,14,24
The findings suggest that non-medical objectives play an important role in cancer inpatients’ decision making. Approximately half of the identified objectives addressed non-medical issues. This is in accord with findings by Schellinger et al., 25 who showed that patients with serious illnesses had approximately as many non-medical as medical goals.
A comparison of these findings with those from previous studies (see Table 3 for details) indicated that VFT is a reliable and valid method to elicit patients’ objectives. Hoskote et al. 13 interviewed cancer patients on their survivorship goals, and identified four goal domains (Physical wellbeing and symptoms, Psychological wellbeing, Social wellbeing and Spiritual wellbeing). Although the present study did not identify a domain corresponding to “Spiritual wellbeing,” many of the objectives in the optimising mental wellbeing, optimising family life and optimising financial life domains reflect those found in the work of Hoskote and colleagues.
Correspondences between cancer inpatients’ objectives identified in this study and those identified in previous studies

Although the authors acknowledge that some of the identified objectives may match more than one of the items from previous studies, for simplicity a one-to-one matching was carried out (except for “Resuming work/hobbies” from van der Kluit et al., 22 which was matched to both “Reduce limitations on engaging in hobbies” and “Reduce work limitations”). Bold items in the last column are themes without subthemes; non-bold items are subthemes whose theme is not shown for clarity.
There are many similarities between the goals of patients in the present study and those of the advanced, incurable cancer patients interviewed by Rand et al. 14 The findings of both studies indicate that what cancer patients want to achieve is not always dependent on clinical prognosis.
Many of the objectives identified in the present study were included in a list of older, hospitalised patients’ goals by van der Kluit et al. 24 Participants in their study were on average older and had predominantly non-cancer diagnoses, indicating that some of the identified objectives are independent of age and diagnosis.
A comparison of the present findings with those of a review by Mitchell et al. 12 on cancer patients’ values and needs provides several useful insights. As goals guide “the individual step by step toward need fulfilment,” 26 the objectives identified using the VFT method in the present study should have corresponding needs or values in the Mitchell et al. review 12 (and vice versa). For example, the important objective of increasing self-determination can be linked to the general values of “being listened to,” “being involved in decision-making” and “taking action” identified by Mitchell et al. 12 Furthermore, many of the identified objectives match themes or subthemes in the needs and general values described in the review. This again shows that eliciting patients’ objectives using VFT methods produces reliable results. However, there are differences between the findings of the two studies. Some of the needs and subthemes identified by Mitchell et al. 12 do not match the fundamental objectives found in the present study (e.g., “faith/spirituality”). This may indicate a sampling bias. The Mitchell et al. 12 review does not include any subthemes for the value of autonomy or the need for social support (from family/friends). In contrast, the cancer patients in the present study expressed objectives associated with those two themes. Moreover, fundamental objectives such as reducing limitations on engaging in hobbies, maximising time at home and reducing work limitations expressed in this study do not have corresponding themes or subthemes in the Mitchell et al. study. 12 This suggests that identification of these objectives provides new insights into what matters to oncologic inpatients.
Overall, comparison of the identified objectives with those found in previous studies shows that although there was at least one issue that was not mentioned (i.e., spirituality), many of the life and treatment issues raised by patients were considered important by oncologic and non-oncologic patients in other studies. The present findings may also provide insights into findings from previous similar studies. It is therefore argued that VFT is a suitable approach to elicit and structure patients’ healthcare objectives.
Strengths and limitations
The study may be one of the first to use VFT as an alternative method to elicit patient objectives in decision-making contexts. The qualitative design permitted an unfiltered, first-hand exploration of the realities and experiences of a group of oncologic inpatients of different ages and sexes. The use of patient-derived objectives ensured that the included domains matter to this specific patient population.
There were several study limitations. Patients were invited to participate by their treating ward physicians. This may have caused selection and sampling biases. As only inpatients participated, the objectives of outpatients, which may be different, were not measured. The comparatively small sample included many patients with haemato-oncologic cancers, and underrepresented patients with more common cancers, such as those of the prostate, lung and breast. The transferability of the study may be limited, as only two participants (approximately 13%) were younger than 30 years and only 40% of interviewees were men. Research in dermatology suggests that sex and age affect treatment goals, 27 so the objectives of younger and male patients may have been underrepresented. Similarly, possible differences in objectives according to ethnicity were not examined because participants were not asked to state their ethnicity.
It is likely that these sampling biases explain the lack of reference to the issue of spirituality in the data. To obtain a broader view of patients’ objectives, future studies should use a more detailed purposive sampling approach.
In addition, the present findings should be considered in the cultural context of the German welfare system. For example, the results may not be transferrable to other countries where healthcare costs or the inability to work have a bigger effect on certain life domains and hence on the objectives of this patient population.
Outlook and future research
This study showed that VFT produces reliable results when exploring patients’ objectives. Researchers and healthcare providers should therefore be encouraged to use the method to investigate the objectives of stakeholders in clinical decision making or healthcare in general. This method can help to create “more complete, more operational, equally concise, and more understandable” hierarchies of objectives compared with methods that derive objectives from decision alternatives. 4 Clinical professionals could use VFT to elicit their patients’ objectives and adapt treatments accordingly. This may reduce the delivery of low-value care. 28 Focussing on what matters to patients may also increase satisfaction and reduce costs. 29 Moreover, the use of patients’ objectives to guide care might simplify coordination between practitioners and reduce the possibility of conflicting recommendations, as all involved parties focus on the same outcomes. 30
The objectives described in this paper could be used by oncologists to initiate a conversation about what matters to cancer inpatients. This may reduce the risk of omitting important objectives, which can be an issue in decision making.31,32 It could also clarify what information needs to be conveyed to patients, 33 reduce communication boundaries 34 and satisfy many cancer patients’ expectations of regular treatment goal discussions. 13 Research also suggests that discussing patients’ health priorities may improve the physician–patient relationship. 35
Like existing values clarification methods, 36 the use of the VFT method to identify objectives could aid the creation of tools that help cancer inpatients identify and communicate what matters to them.
Other researchers are encouraged to extend the objectives identified in this study to further increase understanding of what matters to cancer inpatients. Future research could investigate which objectives are considered more or less important (and in which situations) by patients by exploring patients’ trade-offs between objectives, for example.1,37 As research findings indicate that cancer patients’ goals change over time, 38 it would also be interesting to conduct longitudinal research to identify potential changes in objectives. Research could investigate the transferability of the present findings using the same method with patients with different types of diseases (e.g. cardiological, urological and endocrinological diseases), as well as those of different ages and cultural backgrounds.
Conclusion
This study demonstrated that VFT is a useful qualitative method to elicit patients’ objectives. A comparison of the study findings with previous research showed that the method is reliable and valid when used to elicit what matters to cancer inpatients. Other researchers and practitioners are encouraged to use VFT to explore the objectives of patients and other healthcare stakeholders. The findings of this qualitative interview study suggest that cancer inpatients have a diverse set of life and treatment objectives. This indicates that oncologists need to be thorough when eliciting what matters to their inpatients to be able to tailor treatments accordingly. VFT could be a useful method to aid this elicitation process.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241266224 - Supplemental material for Using value-focused thinking to elicit oncologic inpatients’ life and treatment objectives: a qualitative interview study
Supplemental material, sj-pdf-1-imr-10.1177_03000605241266224 for Using value-focused thinking to elicit oncologic inpatients’ life and treatment objectives: a qualitative interview study by Lukas Fenkart, Rüdiger von Nitzsch, Esther Höggemann and Cord Spreckelsen in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank all the patients who agreed to participate in the interviews, thus enabling this study to be conducted. We would also like to express our appreciation for the efforts of oncologists Jens Panse, Anna Dorottya Doleschall and Benjamin Rolles of RWTH Aachen University Hospital, who approached eligible patients for this study and allowed us to conduct the interviews on the wards. We also thank Martina Thume for her valuable support.
Author contributions
Lukas Fenkart: validation, formal analysis, investigation, resources, data curation, writing – original draft and visualisation. Rüdiger von Nitzsch: conceptualisation, methodology, validation, formal analysis, investigation, writing – review and editing, supervision and project administration. Esther Höggemann: formal analysis and validation. Cord Spreckelsen: conceptualisation, methodology, resources, writing – review and editing, supervision and project administration.
Declaration of conflicting interests
The authors declare that they have no conflicting interests.
Funding
This research received open access funding provided by the Open Access Publishing Fund of RWTH Aachen University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.