
Abstract
The aim of this short narrative review was to evaluate the existing literature regarding the clinical use of ketamine among individuals with dementia, especially those with behavioral disturbances. PubMed, Cochrane, and Ovid (Embase, APA PsycINFO, and MEDLINE) databases were searched for abstracts using the search terms “ketamine” AND “dementia.” Only articles describing the use of ketamine in individuals with dementia were included. Articles that did not include individuals with dementia, did not use ketamine, were published in a non-English language, primarily described animal studies, or were reviews were excluded. Three case reports met the inclusion criteria. One described the use of subcutaneous ketamine for depression, one described the use of intramuscular ketamine for acute agitation, and one described the use of S-ketamine as anesthesia during electroconvulsive therapy for depression and catatonia. No significant adverse effects were reported in any of the cases. Although the use of ketamine in the treatment of depression and agitation associated with dementia has potential, the current evidence remains limited. High-quality prospective studies are needed to confirm the observations of these case reports before ketamine can be used to treat behavioral disturbances in individuals with dementia.
Introduction
Alzheimer’s disease (AD) and related dementias affect around 1.6% of the population of the United States, with an expected increase to 3.3% by 2060. 1 During disease progression, behavioral disturbances—including depression, psychotic behaviors, and agitation—are commonly observed. The pharmacologic interventions currently approved by the Food and Drug Administration (FDA) for the management of AD and related dementias are categorized by the Alzheimer’s Association into those that delay symptom progression and those that treat behavioral disturbances. 2 Another recent class of interventions includes the intravenous-infused monoclonal antibodies aducanumab and lecanemab, which alter disease progression by targeting beta-amyloid protein in the early stages of AD.3,4 Acetylcholinesterase inhibitors and glutamate regulators are reported to delay disease progression. 3 Furthermore, an orexin receptor inhibitor, suvorexant, is indicated for insomnia, whereas an atypical antipsychotic, brexpiprazole, is approved for agitation related to dementia.5–7 However, despite efforts by the FDA to expand treatment options for dementia, the most commonly used medications have limited efficacy and can cause substantial adverse effects. Additionally, the ongoing use of off-label medications for the management of behavioral disturbances in this vulnerable population reflects the urgent need for alternative treatment options.
Over the past two decades, an anesthetic, ketamine (an N-methyl-D-aspartate [NMDA] receptor antagonist), has been studied for its use in treating depression. 8 In 2019, the FDA approved the use of esketamine (a ketamine derivative) outside of anesthesia as a treatment for depression.8–10 Its mechanism of action is postulated to involve NMDA receptor antagonism coupled with the increased expression of neurotrophic factors (specifically, brain-derived neurotrophic factor [BDNF]). Recent studies support the use of ketamine for the management of several other psychiatric and nonpsychiatric disorders, including treatment-resistant depression, neurocognitive disorder, delirium, and pain.11,12
The history of ketamine begins in 1956, with the discovery of the compound phencyclidine. Although a potent anesthetic and analgesic, phencyclidine led to increased postoperative delirium, thus limiting its use in clinical practice. 12 A decade later, in 1966, Parke Davis Company introduced ketamine, a shorter-acting analog of phencyclidine, as an anesthetic. Eduardo Domino and Guenter Corssen discovered that the shorter half-life of ketamine (compared with its native compound phencyclidine) led to a unique dissociative state without undesirable post-delirium side effects. 13 This led to the FDA approving the use of ketamine for the induction and maintenance of anesthesia in 1970. The ease of use, safety, tolerability, and antinociceptive effects of ketamine have placed it among the most successful human and veterinary anesthetic agents.10,14
Structurally, ketamine is an aryl cyclohexylamine derivative that is composed of a racemic mixture of two isomers: S-ketamine and R-ketamine. S-ketamine binds with a stronger affinity to NMDA receptors, thus leading to more potent anesthetic effects than those of its isomer counterpart.12,14 However, despite its lower NMDA affinity, recent studies focusing on depression have demonstrated that R-ketamine has longer-lasting effects on depression, with fewer side effects such as psychotomimetic and dissociative states.11,12,14 Ketamine is most frequently administered intravenously, to obtain 100% bioavailability at doses ranging from 0.5 to 2 mg/kg.10,14 Its bioavailability decreases to 93% when administered intramuscularly (at doses of 1–13 mg/kg) and to between 8% and 45% when administered nasally (at doses of 0.5–1 mg/kg). Oral administration is generally avoided because of extensive first-pass metabolism in the liver. Ketamine is lipid-soluble, has relatively low protein-binding properties, and is rapidly distributed upon crossing the blood–brain barrier. After its metabolism by cytochrome P450 (CYP450) enzymes, the inactive metabolites are renally excreted with an elimination half-life of 1 to 3 hours. CYP450 inhibitors may increase ketamine serum concentrations. For example, its concomitant use with central nervous system depressants such as tramadol and haloperidol, which are CYP450 inhibitors, can significantly worsen sedation. 14
For the past two decades, ketamine has been of clinical interest outside the field of anesthesia, particularly in psychiatry. 8 The earliest human clinical trial, by Berman et al., revealed that a single ketamine dose can improve symptoms of depression. 15 Several studies have since confirmed these results, and its use is now well established.8,11 However, the mechanism of action of ketamine is still not fully understood. Ketamine has a “slow off rate,” referring to its longer binding period to the NMDA receptor compared with memantine (another NMDA receptor antagonist that was approved by the FDA in 2003 for the treatment of moderate-to-severe Alzheimer’s dementia). 12 The antidepressant effects of ketamine may result from its stimulation of α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptors as well as the higher expression of plasma BDNF and mammalian target of rapamycin, through the activation of second messenger systems.12,14 Ketamine also acts on hyperpolarization-activated cyclic nucleotide channels and smooth muscle L-type voltage-dependent calcium channels, which are thought to contribute to its hypnotic and psychomimetic effects. 14
Collectively, studies have reported the potentially positive effects of ketamine in several acute and chronic psychiatric conditions, including treatment-resistant depression, bipolar disorder, post-traumatic stress disorder, obsessive compulsive disorder, substance use disorder, eating disorders, delirium, and pain.8,11 Its use has also been proposed for individuals with dementia based on its effects on neuroinflammation and the stimulation of neurotrophic factors.8,11,12,16,17 This, combined with its antidepressant effects, suggests that ketamine may have several potential roles in individuals with dementia. The present review aimed to assess the evidence regarding the use of ketamine among individuals with dementia, especially those with behavioral disturbances, and to outline the full scope of its potential applications. In this way, we aim to layer evidence onto the theoretical narrative outlined in the existing literature.
Methodology
Although the present article was not intended as a systematic review, we followed an organized methodology for a review of the literature regarding the use of ketamine among individuals with dementia. The authors CC, KD, TPE, and NY searched the PubMed, Cochrane, and Ovid (Embase, APA PsycINFO, and MEDLINE) databases on 24 March 2023 using the search terms “ketamine” AND “dementia.” Studies were included if they evaluated the use of ketamine among older individuals (≥60 years) with dementia and were published in English-language journals. Studies were excluded if they did not include individuals with dementia, did not use ketamine as the therapeutic agent, were published in non-English languages, were animal studies, or were review papers. Information that was extracted from the studies included the type of study, indication for ketamine use, drug comparators, outcomes, and adverse events. Any disagreements regarding the inclusion or exclusion of articles were resolved by discussion between the first (AK) and corresponding (RT) authors.
Results
After title and abstract screening, we identified 23 articles. After removing 11 duplicates, 12 articles remained for the full-text review. The full-text review revealed six reviews, one translational study, one book chapter, and one study in a non-English language; the remaining three case reports (Table 1) met the inclusion criteria.
Case reports describing ketamine use in patients with dementia.
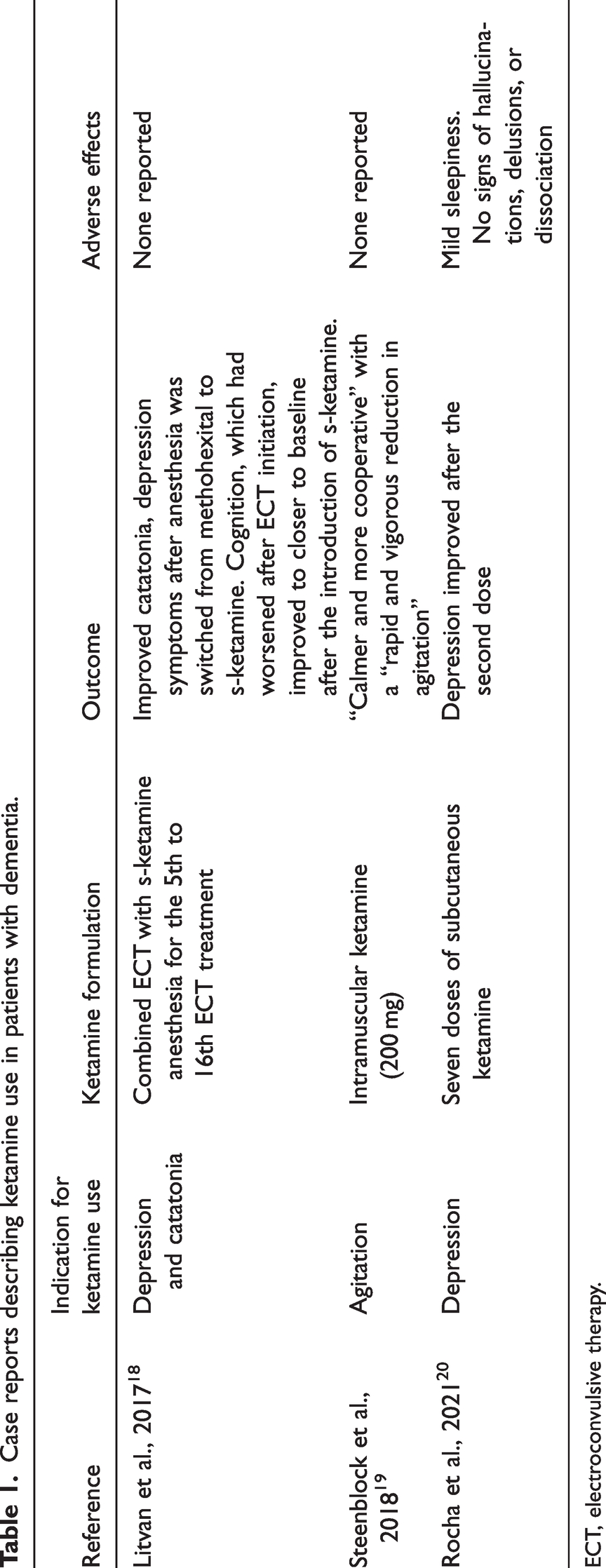
ECT, electroconvulsive therapy.
The first case report, by Litvan et al. in 2017, described the use of S-ketamine as an anesthetic during electroconvulsive therapy (ECT) in a 74-year-old woman with AD with mixed-type dementia who resided in an assisted-living facility. 18 Her Mini Mental State Examination (MMSE) score was 24/30 at the time of diagnosis. She experienced a severe depressive episode with psychotic features; the onset was approximately 10 months prior to her presentation to a psychiatric intensive care unit, where she was eventually treated with S-ketamine and ECT. Upon admission to the psychiatric intensive care unit, she exhibited symptoms of catatonia, with a Bush–Francis Catatonia Rating Scale score of 23. She was described as immobile, unresponsive, incontinent, and requiring a nasogastric tube and intravenous nutrition. The patient was treated with a regimen of lorazepam, mirtazapine, haloperidol, and donepezil for 3 weeks without recovery; she then underwent six unilateral and 10 bilateral ECT treatments. After the fourth ECT treatment, methohexital was switched to S-ketamine because of its low seizure threshold; the S-ketamine dose was not reported by the authors. Although the measured quality of seizure activity did not improve, the patient’s symptoms showed marked improvements; the authors reported that “she was able to establish contact with her environment for the first time since her admission and partially responded to questions adequately.” Following an additional 11 sessions of ECT, her symptoms of catatonia resolved, with a reduction in the Bush–Francis Catatonia Rating Scale from 23 to 2 points. Her cognition declined during the treatment, with an MMSE of 13/30 after the 14th ECT session. However, after lorazepam discontinuation and following the last ECT treatment, her MMSE improved to 21/30. The authors opined that the antidepressant effect (and possible synergism with ECT), a favorable seizure profile, and the potentially neuroprotective attributes of ketamine led to the complete remission of depression and catatonia in this patient with dementia.
In 2018, Steenblock et al. described the successful use of ketamine to treat acute agitation in a 77-year-old woman with dementia (described as major neurocognitive disorder by the authors). 19 The patient grew increasingly agitated and aggressive in the memory care unit of a long-term care facility in which she had resided for 3 months. Despite de-escalation attempts by the police and pharmacologic interventions (intramuscular haloperidol and lorazepam), she was sent to the emergency room for acute agitation that did not respond to treatment. While traveling to the emergency department, she continued to exhibit substantial agitation and was administered 200 mg intramuscular ketamine (3 mg/kg), given in divided doses (100 mg per buttock). The authors described a “rapid and vigorous reduction” in agitation following the administration of intramuscular ketamine, “with no apparent adverse effects.” The patient was observed overnight for monitoring in the emergency department and was reportedly “calm, alert, and cooperative, although somewhat bland and apathetic” the following morning; her behavior remained stable for the following week.
In 2021, Rocha et al. described the use of subcutaneous ketamine for treatment-resistant depression in a 76-year-old woman with AD. She had a Clinical Dementia Rating Score of 3, with severe cognitive impairment, and was hospitalized for acute medical comorbidities. 20 She experienced remission of her depression following the second of two doses of subcutaneous ketamine. The first dose (0.5 mg/kg) was administered 2 days prior to the second dose (0.75 mg/kg). Recovery was defined by a Clinical Global Impression-Improvement score reduction from 7 to 1 21 (suggesting a marked improvement in global illness severity), overall improvement from the start of treatment, and therapeutic response. Six additional treatments of subcutaneous ketamine were administered at a dose of 0.75 mg/kg, with desvenlafaxine supplemented at the fourth dose. One month after the last ketamine dose, the patient displayed no symptoms of depression on desvenlafaxine alone. The patient did not have any severe side effects during the treatment, such as hallucinations, dissociation, or autonomic dysregulation. She slept for approximately 1 hour during the treatment but was easily arousable. The authors of the report described “sleepiness” as the only adverse effect of treatment.
Discussion
Our review of the literature identified three publications—all case reports—on the use of ketamine in individuals with dementia. Each of these reports described the use of ketamine in a distinct clinical scenario: depression with catatonia, agitation, and treatment-resistant depression. All three case reports noted a rapid improvement in target symptoms upon ketamine initiation. Litvan et al. documented the good tolerability of ketamine in the context of its use as an anesthetic agent for ECT. 18 However, Steenblock et al. noted that cognitive side effects may vary based on dose, frequency of use, diagnosis, and other unknown variables. 19 Although Rocha et al. acknowledged the risks of high blood pressure, dizziness, dissociation, nausea, and headache with ketamine, they only observed sleepiness as an adverse effect in their patient. 20
The adverse effects of esketamine were highlighted in a recent analysis using the FDA Adverse Event Reporting System; 117 distinct adverse reactions were identified among 5061 reports that were reviewed. Unsurprisingly, potential risks including experiences of flashback, tachyphylaxis, and autoscopy were reported as “newly identified.” Other noteworthy findings included frequent reports of euphoric mood and relaxation, and relatively high rates of suicidal ideation and attempts, further underscoring the importance of close monitoring and healthcare vigilance. However, FDA Adverse Event Reporting System data are self-reported and thus may not be entirely accurate or complete; the study therefore cannot definitively prove causal links between esketamine and specific adverse events. More studies are required to confirm these findings, understand the mechanisms underlying these potential risks, and develop optimal management strategies. 22
There is a growing consensus toward deconstructing the broad entity of behavioral and psychological symptoms of dementia into their component symptoms. 23 Such an approach is also consistent with the deconstruction of the Diagnostic and Statistical Manual of Mental Disorders-defined diagnostic entities into individual symptoms. 24 The case studies reported in the present review, which provide an early indication of the successful application of ketamine in individuals with dementia, align well with this approach. The current diagnostic system is relatively limited in terms of capturing the specific symptoms that may warrant the use of ketamine.
On the basis of its currently understood mechanism of action, ketamine has the potential to affect several aspects of dementia care by targeting multiple hypothesized neurobiological mechanisms that lead to behavioral disturbances. Although the current evidence supports its use for the treatment of just three distinct behavioral symptoms—depression, catatonia, and agitation—it may affect a range of other behavioral symptoms in dementia. Such an approach would be consistent with the principles of precision psychiatry. There is a precedent for using existing medications to target highly specific behavioral phenomena in dementia. For example, both ECT and dronabinol have been used for the treatment of agitation and aggression in dementia.25,26 Notably, the broader mechanism of action of ketamine may point to an even broader set of potential applications, especially among individuals with dementia.
Conclusions
Ketamine is a unique compound with multimodal effects, and there is evidence to support its possible novel indications for treating targeted behaviors in dementia. To date, evidence to support and guide its use is limited to case reports. However, these reports point to a heterogeneous range of applications including depression, catatonia, and agitation. These case reports also suggest that its safety profile may be relatively favorable in individuals with dementia, although larger controlled studies are required to determine additional risks that have not yet been identified. Until more substantial evidence for the use of ketamine among older adults with dementia is available, case-based evidence constitutes a preliminary—but relevant—segment of the literature supporting its use among these individuals. Nonetheless, given the limitations of the available data, the routine use of ketamine in individuals with dementia cannot be advocated at this time. In addition, there is not yet enough evidence for the use of ketamine as a monotherapy in the management of behavioral disturbances in dementia. However, ketamine may have a role in the future management of individuals with dementia, as indicated by the emerging evidence described in our narrative review. Hence, it would be prudent to consider ketamine as an adjunct treatment for the behavioral and psychological symptoms of dementia, in combination with other pharmacotherapeutic agents that have a greater evidence base for their efficacy and safety.
Footnotes
Acknowledgements
The authors thank the SAGE editors for their critical comments and suggested improvements of the draft manuscript.
Author contributions
AK and RT conceived the idea. AK, TPE, CC, NY, and KD wrote the initial draft. AK and RT reviewed the draft and suggested changes. AK and RT reviewed and approved the final manuscript. All authors meet the International Committee of Medical Journal Editors criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.