
Abstract
Objective
To compare the effects of early and delayed cord clamping on the haemoglobin levels of neonates delivered at term.
Methods
This randomized controlled trial enrolled pregnant women during the second stage of labour. They were randomized into either the early cord clamping (ECC) group or the delayed cord clamping (DCC) group in the ratio of 1:1. Following delivery of the baby, the umbilical cords of participants in the ECC group were clamped within 30 s of delivery of the neonate while those of participants in the DCC group were clamped after 2 min from the delivery of the neonate. The primary outcome measure was the effect of ECC and DCC on the haemoglobin levels of neonates delivered at term.
Results
A total of 270 pregnant women were enrolled in the study. Their baseline sociodemographic and clinical characteristics were similar in both groups. There was no significant difference in the mean haemoglobin level between ECC and DCC groups at birth. The mean haemoglobin level of the neonates at 48 h postpartum was significantly higher in the DCC group than the ECC group.
Conclusion
DCC at birth was associated with a significant increase in neonatal haemoglobin levels at 48 h postpartum when compared with ECC.
Introduction
Determining the appropriate timing for umbilical cord clamping after delivery of the newborn baby has been a controversial issue.1–5 There is a wide variation in the definitions of early and delayed cord clamping in terms of the timing of the clamping. 5 Early cord clamping is often defined as the clamping of the umbilical cord between delivery and 30–60 seconds after delivery, whereas delayed cord clamping is the clamping of the cord beyond 1 minute of delivery.4–6 Although there have been some randomized controlled trials comparing the benefits of delayed versus early cord clamping, an ideal time has not been mapped out. 7 Previously, early cord clamping was incorporated as an important component of the active management of the third stage of labour, when it was thought to prevent primary postpartum haemorrhage. 1 However, recent studies have revealed that it is of no significant benefit in the prevention of postpartum haemorrhage.6,8,9
Some researchers are of the opinion that early cord clamping is beneficial in the sense that it makes the collection of cord blood samples possible for the analysis of blood gases and acid-base balance, permits prompt resuscitation of the newborn when asphyxiated and enhances the harvesting of stem cells for public blood banking.10–12 Nevertheless, others are of the opinion that clamping of the umbilical cord should be delayed for more than 1 minute after delivery. The timing of umbilical cord clamping determines the amount of blood transfused into the neonatal cardiovascular system from the placenta through the umbilical cord. 13 Available evidence has shown that the benefits of delayed clamping include increased haemoglobin and haematocrit levels in the neonate and a subsequent reduction in the rate of iron deficiency anaemia, which may extend into infancy.10–12,14,15
Reduced haemoglobin concentrations associated with iron deficiency anaemia are common problems encountered by children in developing countries because nutritional deficiencies, hookworm infestations, malaria infections and repeat pregnancies remain common in these regions. 16 Neonates also run the risk of anaemia at birth since some of the mothers have anaemia during pregnancy. 17 Anaemia in infancy is a public health issue in developing countries and can lead to poor neurological development.3,17,18 Worldwide, one-fourth of all preschool children are estimated to be affected by reduced haemoglobin concentration and iron deficiency anaemia, with the attendant complications of altered affective response, impaired motor development, and cognitive and behavioural deficits.10,19,20
Delayed cord clamping allows time for the transfusion of foetal blood from the placenta to the neonate at the time of birth. 18 The newborn receives up to a 30% increase in blood volume and approximately a 60% increase in red blood cells through placental transfusion at birth. 12 This placental transfusion is a physiological process and accounts for between 19 and 40 ml/kg of birth weight on average, equivalent to as much as 2% of the newborn's final birth weight.12,21 It also protects very low-birth-weight infants from intraventricular haemorrhage, the late onset of sepsis and motor disability.12,18,21 On the other hand, delayed cord clamping could lead to neonatal polycythaemia, an increased rate of hyperbilirubinaemia and the need for phototherapy. 4
There appears not to be any definite conclusion on whether to practice early or delayed cord clamping in both developed and developing countries. In Europe and other developed countries, there is also a great variation in what is practised.12,14,15 Nevertheless, early cord clamping is apparently the dominant practice in many nations around the world. Despite the established benefits of delayed cord clamping in improving iron status and preventing anaemia in neonates and infants, there is still a palpable disconnect between this knowledge and the practice thereof, even in developing countries where iron-deficiency anaemia is very prevalent.
In our facility at Enugu State University of Science and Technology (ESUT) Teaching Hospital, Parklane, in southeast Nigeria, we tend to use early cord clamping, just like many other hospitals in our environment. However, there is a great need for us to educate our clients on the need for them to be involved in the decision-making concerning the timing of the cord clamping to be adopted for them in the 3rd stage of labour. This formed the basis for this current study, which in addition sought to contribute to establishing an evidence-based recommendation for policy change on the appropriate timing of cord clamping, especially in developing countries like ours.
This study aimed to determine the effect of early versus delayed cord clamping on haemoglobin levels of neonates delivered in this environment and verify the benefits and risks associated with the two cord clamping methods.
Patients and methods
Study design, setting and population
This hospital-based, randomized controlled trial was conducted at the labour ward/delivery unit of ESUT Teaching Hospital, Parklane, Enugu, Nigeria between 22 June 2022 and 22 December 2022. The study population comprised of all the term (37–42 weeks) newborn babies delivered in the hospital within the study period. The inclusion criteria were as follows: (i) healthy consenting pregnant women with normal singleton term pregnancies; (ii) healthy neonates without any complications delivered via spontaneous vaginal delivery. The exclusion criteria were as follows: (i) women with multiple gestations; (ii) preterm pregnancies; (iii) post-term pregnancies; (iv) pregnancies that were complicated by medical conditions such as diabetes mellitus, hypertension, cardiac diseases, sickle cell disease, chorioamnionitis, antepartum and postpartum haemorrhage, maternal haemoglobin level <10.0 g/dl at 36 weeks gestational age for booked mothers and unbooked pregnant women with haemoglobin level <10.0 g/dl on admission to the labour ward; (v) neonates with congenital diseases; (vi) non-vigorous neonates requiring any form of resuscitation; (vii) neonates who became sick within the first 48 h.
This study was approved by the ethical committee of ESUT Teaching Hospital, Parklane, Enugu, Nigeria on 10 June 2022 (reference no. ESUTHP/C-MAC/RA/034/141). A written informed consent was obtained from all participants before recruitment into the study. The study adhered to the CONSORT guidelines. 22
Sample size estimation
The minimum sample size N for each arm of this study was determined with the following formula:


Randomization technique and group allocation sequence
Randomization and allocation concealment were applied for the study using a computer-based random sequence generator (http://www.randomization.com) created by a statistician (who was not part of the study team) in a 1:1 ratio using randomization blocks of 4. Sealed, non-transparent brown envelopes were marked serially from 1 to 270; each numbered envelope contained a white piece of paper labelled either ECC for the intervention group that received early cord clamping or DCC for the control group that received delayed cord clamping. The envelopes were handed over to a trained nurse midwife who was completely unaware of the group the participant belonged to. The trained midwife gave the envelopes to the women to pick up when they were admitted to the labour ward. The researcher, the midwives and the participants in labour were not blinded. The women were counselled on the procedure during the antenatal visits and again when they entered the first stage of labour, with informed written consent obtained from them. The paediatrician in the labour ward examined the baby and excluded anomalies from it; the researcher who took the blood sample to the laboratory; the laboratory scientist who analysed the blood sample for haemoglobin level; and the trained staff for the second-day follow-up test were all always available and were blinded.
Pilot study
A pilot study was carried out on 10% of the total population of the study, which was a small group of babies who were not part of the main study. This was done to ascertain the feasibility of this research. The feasibility study was done in a very big mission hospital (Annunciation Hospital, Emene, Enugu, Nigeria) and the result showed that DCC was more beneficial to the neonates 48 h after delivery.
Obstetric and blood sampling procedures
Having counselled and obtained informed consent from the participants, during the second stage of labour, the midwife unfolded the paper and revealed the newborn who underwent early cord clamping (which involved double clamping of the umbilical cord within 30 s of delivery of the neonate) or the newborn who underwent delayed cord clamping (which involved double clamping of the umbilical cord after 2 min from the delivery of the neonate.). The researcher took the delivery and kept the neonate at 15 cm below the maternal vulva for 30 s (early) or 2 min (delayed) according to the intervention in the envelope picked by the pregnant woman. The obstetrics care giver clamped the cord and collected a cord blood sample. The umbilical cord was cut in between the two clamps. The neonate was then placed on the maternal abdomen, which was covered with cloth, which provided warmth. The trained midwife did the timing with the stopwatch, which was set according to the intervention picked by the mother, either 30 s or 2 min.
The cord was double clamped and 1.5 ml of blood was collected from the point between the clamps into an ethylenediaminetetra-acetic acid (EDTA; 1.8 mg/ml) tube (sample A) (BD Vacutainer®; BD, Plymouth, UK). The blood sample for haemoglobin was stored at 4°C and analysed within 24 h. A single dose of 10 IU of oxytocin (Syntocinon®; Norvartis, Basel, Switzerland) was administered intravenously immediately after cord clamping. Then, after blood sample collection, the cord was cut with cord scissors. Controlled cord traction was undertaken and after the delivery of the neonate, routine care was provided to the mother and the neonate. The neonate was handed over to the neonatologist and finally to the mother. Then, 48 h after the delivery of the neonate, an intravenous blood sample (1.5 ml, sample B) was collected from the baby’s vein into an EDTA tube (1.8 mg/ml; BD Vacutainer®) after gentle application of a tourniquet and topical anaesthetic cream on the puncture site. Samples were also collected into EDTA tubes (1.8 mg/ml; BD Vacutainer®) from the mother in the active phase of labour from their cubital fossa (sample C) and another sample was collected 48 h after delivery. The blood samples were stored at 4 °C and analysed within 24 h. The blood samples were sent to the haematology laboratory for analysis using a Sysmex XE-2100™ automated haematology system (Sysmex, Kobe, Japan).
Study definitions
The following definitions were used throughout the study: (i) the normal haemoglobin level in neonates was defined as 14–24 g/dl; (ii) anaemia in a neonate at 48 h was defined as HB < 14 g/dl; (iii) ECC was the clamping of the umbilical cord within 30 s of the delivery of the neonate; (iv) DCC was the clamping of the umbilical cord 2 min after the delivery of the newborn baby.
Primary outcome measure
The primary outcome measure was the effect of ECC and DCC on the haemoglobin levels of neonates delivered at term.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA). The sociodemographic variables were used to categorize the data. Data were subjected to comparative statistical evaluation, which yielded frequencies (%) and mean ± SD. Comparisons between groups used χ2-test for categorical variables and Student’s t-test for continuous variables. A P-value <0.05 at one degree of freedom (df = 1) was considered statistically significant.
Results
This randomized controlled trial included 270 neonates and 270 mothers; 135 had ECC and 135 had DCC. Figure 1 shows the flow diagram of the study participants. There were no significant differences in the sociodemographic characteristics and clinical profile of the mothers between the ECC and DCC groups (Table 1).
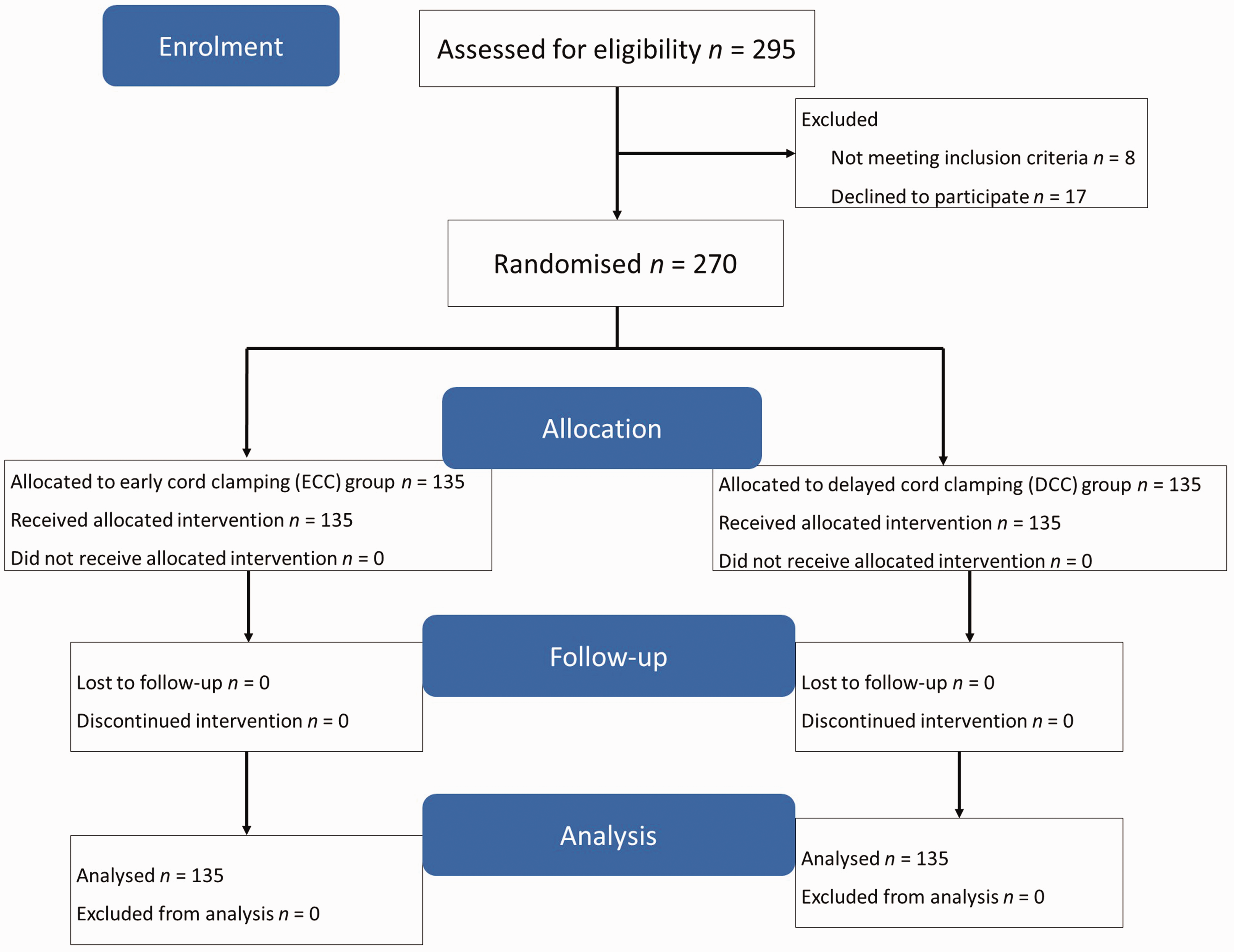
Consort flow diagram showing the enrolment, randomization, allocation and analysis of newborns and their mothers in this hospital-based, randomized controlled trial that aimed to determine the effect of early versus delayed cord clamping on haemoglobin levels of neonates.
Sociodemographic and clinical characteristics of the mothers (n = 270) enrolled in a hospital-based, randomized controlled trial that aimed to determine the effect of early cord clamping (ECC) versus delayed cord clamping (DCC) on haemoglobin levels of neonates.

Data presented as n of patients (%).
No significant between-group differences (P ≥ 0.05).
The gestational age at presentation ranged from 37–40 weeks. There were no significant differences in the neonatal characteristics of the newborns between the ECC and DCC groups (Table 2).
Neonatal characteristics of the neonates (n = 270) enrolled in a hospital-based, randomized controlled trial that aimed to determine the effect of early cord clamping (ECC) versus delayed cord clamping (DCC) on haemoglobin levels of neonates.
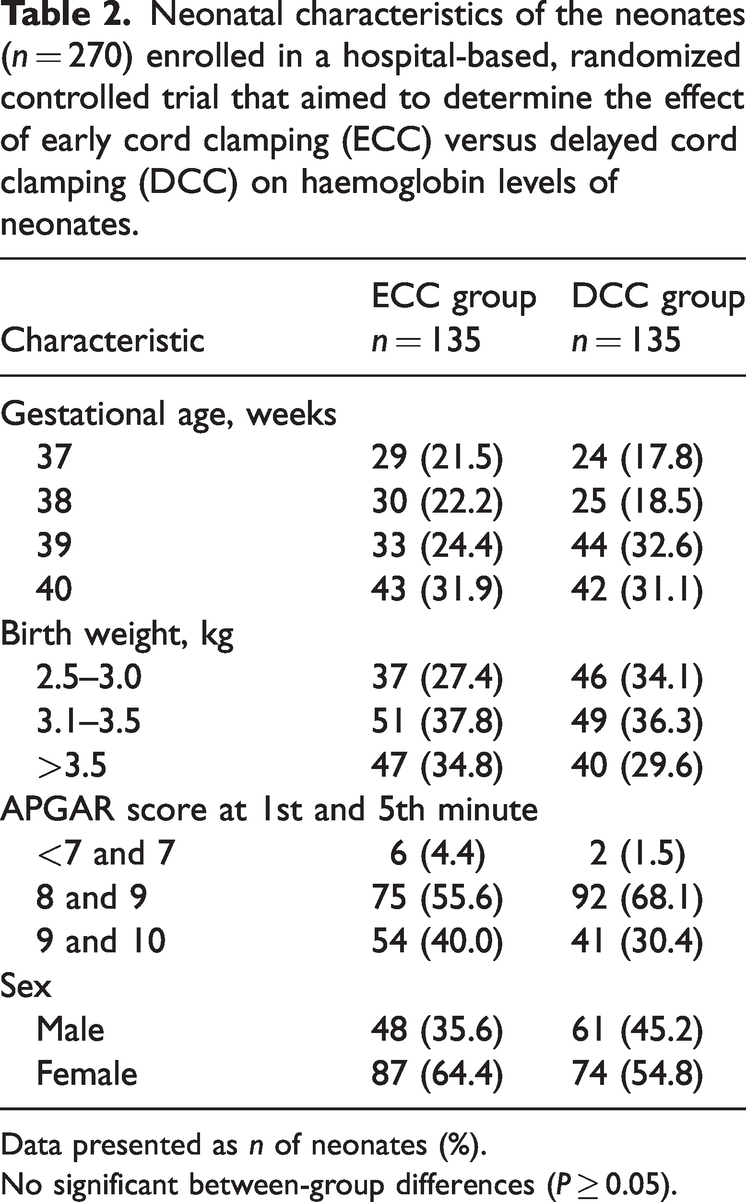
Data presented as n of neonates (%).
No significant between-group differences (P ≥ 0.05).
Table 3 shows the mean difference in haemoglobin levels of the neonates at birth between the ECC and DCC groups. There was no significant difference in the mean haemoglobin at birth between the two groups. However, there were significant differences in the mean haemoglobin at 48 h postpartum between the two groups (P < 0.01); and in the change in haemoglobin at birth and 48 h postpartum within each group (P < 0.01 for both comparisons). There was no association between the maternal sociodemographic and clinical profile and the neonatal haemoglobin level at 48 h in the ECC and DCC groups (data not shown). A total of 28 of 135 (20.7%) neonates in the DCC group had low neonatal Hb (<14 g/dl) compared with 50 of 135 (37.0%) neonates in the ECC group at 48 h postpartum (P < 0.01).
Mean difference of the haemoglobin (Hb) level of the neonates (n = 270) enrolled in a hospital-based, randomized controlled trial that aimed to determine the effect of early cord clamping (ECC) versus delayed cord clamping (DCC) on haemoglobin levels of neonates.

Student’s t-test was used to compare continuous variables.
SD, standard deviation; MD, mean difference; CI, confidence interval; SE, standard error.
Discussion
The principal findings from this current study showed that there was no significant difference in the mean haemoglobin level between the ECC group and the DCC group at birth. However, the mean haemoglobin level of the neonates at 48 h postpartum was significantly higher in the DCC group than the ECC group. In addition, the change in haemoglobin level from birth to 48 h postpartum in each group was significant. There was no significant association between maternal and neonatal sociodemographic and clinical characteristics and neonatal haemoglobin level at 48 h postpartum in both groups.
This current study demonstrated that the mean haemoglobin level of the neonates at 48 h postpartum was significantly higher in the DCC group than in the ECC group, which suggests that DCC significantly improved the haemoglobin levels of neonates at 48 h postpartum. This particular finding was consistent with other studies that observed that DCC allows more transfusion of blood from the feto-placental compartment through the cord to the newborn; and this is a cost-free iron boost with major beneficial roles in preventing anaemia among neonates and infants as well as promoting infant brain development.11,12,23–26 However, there was no significant difference in the mean haemoglobin level between the ECC group and the DCC group at birth. This was consistent with a previous similar randomized control trial. 27 The reason for this could be that the effect of the extra volume of whole blood transfused from the placenta to the neonate might not have been reflected in the DCC group then, at birth, when the haemoglobin levels were measured. Usually, after receiving red blood cells, haematocrit equilibration takes place gradually, leading to a stable packed cell volume. 28
Furthermore, the mean haemoglobin level at birth was higher than that at 48 h postpartum for the ECC group, while the mean haemoglobin level at birth was lower than that at 48 h in the DCC group. These findings suggest that those who underwent ECC had a relative drop in their haemoglobin level over the first 48 h postpartum. This drop could be explained by the fact that the neonates who underwent ECC did not benefit from placental transfusion following the initiation of respiration at birth, unlike those who underwent DCC. Hence, it was noted at 48 h postpartum that the majority of the babies (50 of 78 neonates; 64.1%) who had haemoglobin concentrations <14 g/dl belonged to the ECC group, while the majority of those who had haemoglobin concentrations > 14 g/dl belonged to the DCC group (107 of 192 neonates; 55.7%). In contrast to the findings of this current study, a study undertaken in Pakistan observed that there was a significant difference in haemoglobin level even at birth between neonates who had ECC and those who had DCC. 25 It is not clear why there is a difference between the current study and the previous study, but it might be due to a difference in the sample sizes of the two studies; there were 135 in each group in the current study compared with 100 in each group in the other study. 25 Furthermore, the duration of ECC in the other study was not defined (not specific) and their DCC was after the cessation of cord pulsation, 25 which might have taken a longer duration, allowing a greater volume of blood to be transfused through the feto-placental compartment to the neonates. In this current study, ECC was defined as 30 s and DCC as 2 min. Variations in the study locations and populations could have also contributed to the difference in the outcomes of the two studies.
In the current study, there were no significant associations between maternal sociodemographic/clinical profile and neonatal haemoglobin at 48 h postpartum in both the ECC and DCC groups. This finding is consistent with a previous study, which also revealed that there was no significant difference in maternal or neonatal outcomes or characteristics between those randomized to ECC or DCC. 6 This is an interesting finding in the sense that it demonstrated that the use of either ECC or DCC was not significantly associated with maternal or neonatal characteristics, including the use of uterotonics and the prevention or treatment of primary postpartum haemorrhage.6,24 In view of all these findings, it suffices to say that the practice of DCC is safe enough for both the neonates and their mothers.6,24
This current study corroborated many other studies, both from developing and developed countries, in elucidating the fact that the practice of DCC should be the better cord clamping method since it is more beneficial to the neonates and, at the same time, harmless to the mothers. DCC has saved the neonates and infants from anaemia and its consequences, thereby conserving the little resources of families in developing countries, with which other necessary needs of the children will be catered for. Yet, it is not routinely practiced in the environment where it is most needed. This matter should be viewed with the utmost seriousness. Hence, the practice of DCC should be encouraged and adopted in our centre (ESUT Teaching Hospital) and other hospitals in developing countries.
This current study had several limitations. First, the follow-up could not be extended to 3- or 6-monthly measurements of the haemoglobin levels of the infants. Secondly, it was also not possible to determine their neurological and motor developments postpartum. Thirdly, it was not possible to assess the haematocrit and ferritin levels, the latter of which could have given insight into the iron stores of the neonates. These could be explored in further robust studies, possibly in a multicentre trial in our environment. It should be noted that the fact that there was no difference in the neonatal and maternal characteristics of the participants between the two groups, especially in terms of mean gestational age and mean maternal age, suggests that the participants were well selected and hence randomized to either the ECC or DCC groups under the same conditions. These conditions might have eliminated bias that could have adversely affected the results of the study. This is desirable and should be observed as one of the strengths of the study. Furthermore, the medical laboratory scientist who analysed the samples was blinded to the treatment groups.
In conclusion, delayed DCC following delivery is associated with a higher neonatal haemoglobin level at 48 h postpartum than ECC. The practice of DCC is beneficial in preventing anaemia among neonates and infants; hence, it should be encouraged, especially in resource-poor settings like ours where maternal and neonatal anaemia are very high. In view of the benefits and safety of DCC, skilled birth attendants may adopt and consolidate this practice all over the world, especially in developing countries. Health talks to pregnant women should include the need for mothers to embrace this idea owing to its advantages in reducing neonatal anaemia and its attendant morbidity and mortality, as well as reducing the need for blood transfusion and resource conservation. Counselling on DCC practice may be fitted into the programme of education and the birth planning process for pregnant women. Advocacy for DCC should be raised and implemented by policymakers at various levels of governance.
Footnotes
Acknowledgements
The authors are grateful to all the research participants and the staff that were involved in the study.
Author contributions
Kelechi P. Enyinna, the principal investigator, was involved in conceptualization, manuscript writing and revision and data collection. George U. Eleje and Boniface U. Odugu were involved in supervision, manuscript writing and revision. Calistus O. Nevo, Ifeanyichukwu Ofor, Chukwuka C. Eze, Darlington S. Okoh, David C. Ikwuka, Fredrick I. Awkadigwe and Kelvin E. Ortuanya were involved in manuscript writing and revision and data collection. Chigozie G. Okafor, Ikechukwu I. Mbachu, Chidinma C. Okafor, Divinefavour E. Malachy, Hyacinth T. Eze and Chukwuemeka C. Okoro were involved in manuscript writing and revision and data analysis. All authors proofread and approved the final copy for submission to the journal.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The cost of the research was borne by the researchers.