
Abstract
Giant choledochal cysts are rare, and so little data exist on the best surgical treatment method. We present here, a case of a giant choledochal cyst that was successfully excised by laparoscopic resection. A 37-year-old female presented with right upper abdominal pain and mild jaundice. On examination she had a right upper abdominal mass which on imaging was observed to be a giant choledochal cyst of type IVa, measuring approximately 129 mm × 190 mm. Her blood test results showed abnormal liver function. We successfully performed laparoscopic resection of the cyst, the patient recovered well and was discharged from hospital eight days post-operation without any complications. We wish to share the experience of this rare case and provide some clinical basis for future diagnosis and use of laparoscopic resection in the treatment of giant choledochal cysts.
Background
A choledochal cyst is an atypical congenital abnormality of the biliary tract system characterized by cystic dilatation of the bile duct and can occur extrahepatically, intrahepatically, or in both locations. 1 The cysts are notably more prevalent among East Asian populations compared to their occurrence in Western nations.1–3 The cysts vary in size but most do not exceed 6 cm. 4 There are five main types of choledochal cyst.4,5 Type I involves the dilatation of the entire common hepatic or common bile duct or segments of each, and is the most commonly encountered. It is further subdivided into type 1a – cystic (the most common type), type 1b – segmental, and type 1c – fusiform/cylindrical. Type II is saccular diverticulum in the extrahepatic bile duct, type III is a choledochocoele, type IVa is multiple cysts involving intra and extrahepatic bile ducts, type IVb is multiple cysts in the extrahepatic bile duct, and, type V is multiple cystic dilatations of the intrahepatic biliary tree which can be focal or diffuse (Caroli disease). Although rare, some cysts may be larger than 10 cm and are referred to as giant cysts.4,6 The rarity of these giant cysts has resulted in a limited number of cases being documented in medical literature and, therefore, there is a paucity of information about their treatment. We report here, a case of a 37-year-old female patient who was diagnosed with type IVa giant choledochal cyst which was successfully treated by laparoscopic resection. We wish to share the experience of this rare case and provide some clinical basis for future diagnosis and use of laparoscopic resection in the treatment of giant choledochal cysts.
Case report
A 37-year-old female presented to our hospital with an 11-day history of right upper abdominal pain, which had started following a meal. The pain was intermittent and dull, and occasionally radiated out to her right shoulder and back. The duration of the episodes varied, but they were consistently accompanied by nausea and vomiting. During her physical examination, it was noted that she had mild jaundice, evidenced by yellow staining of her skin, mucous membranes, and sclera. A palpable mass was detected in her right upper abdomen. The mass had a slight firm texture, could be moved, and caused tenderness upon pressure. The patient had previously enjoyed good health with no previous surgery, and there was no family history of a similar condition.
The patient’s liver function tests were abnormal and included elevated levels of the following: total bilirubin (147 μmol/l; normal range:5–28 μmol/l); direct bilirubin (88 μmol/l; normal range: 0–10 μmol/l); indirect bilirubin (59 μmol/l; normal range: 0–17 μmol/l); alanine aminotransferase (154 U/l; normal range: 0–40 U/l), aspartate aminotransferase (139 U/l; normal range: 0–40 U/l); alkaline phosphatase (185 U/l; normal range: 31–135 U/l); γ-glutamyl transpeptidase (219 U/l; normal range: 0–38 U/l); serum amylase (72 U/l; normal range: 0–200 U/l). Other blood test results were unremarkable. Ultrasonographic evaluation showed a cystic structure in the choledochal duct area (Figure 1a). A computed tomography (CT) scan further confirmed dilatation prominently in the common bile duct, which displayed cystic dilatation (Figure 1b). Magnetic resonance cholangiopancreatography (MRCP) showed dilatation of the intra- and extrahepatic bile ducts, especially the common bile duct, and cystic dilatation with a maximum size of approximately 129 mm × 190 mm. (Figure 1c). The surrounding structural tissues were also compressed.

Imaging Studies. (a) Ultrasonographic evaluation showed a cystic structure in the choledochal duct area. (b) A computed tomography (CT) scan confirmed dilatation prominently in the choledochal duct, which displayed cystic dilatation and (c) magnetic resonance cholangiopancreatography (MRCP) showed dilatation of the intrahepatic and extrahepatic bile ducts, especially the common bile duct, showing cystic dilatation with a maximum size of approximately 129 mm × 190 mm.
Following patient consent, we performed laparoscopic resection of the choledochal cyst. For this procedure, a 1 cm incision was made below the navel to establish a pneumoperitoneum pressure of 12–14 mmHg, and a 10 mm trocar was placed as an observation hole to aid insertion of the laparoscope. Four trocars were placed as follows: below the right costal margin along the anterior axillary line (5 mm Trocar); lateral to the right rectus abdominis muscle at the right lower abdomen near the umbilicus (10 mm Trocar); below the left costal margin along the anterior axillary line (5 mm Trocar); lateral to the left rectus abdominis muscle at the left lower abdomen near the umbilicus (12 mm Trocar). However, due to the size of the giant cyst, the operation space was too small and affected the procedure. Therefore, we adjusted the last port to be slightly outward and downward (Figure 2a). Following entry of the laparoscope, we observed that the giant cyst was attached to the stomach, duodenum and pancreas. With the aid of an ultrasonic scalpel and bipolar electrocoagulation, we separated surrounding tissues and carefully avoided unnecessary damage to the attachment structure. We continued to strip the cyst to expose the anterior wall of the choledochal cyst.
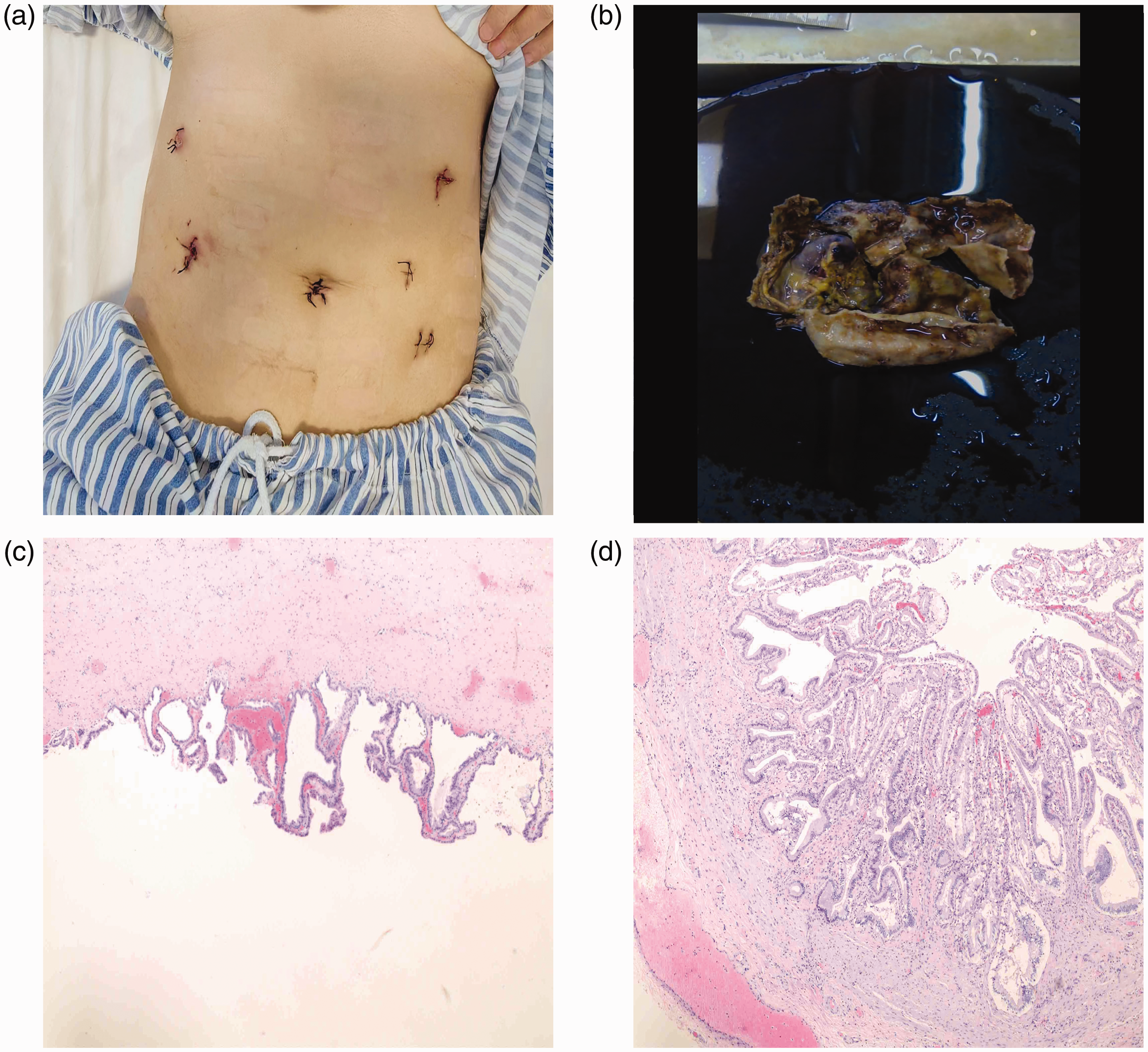
(a) Post-operative abdominal incisions. (b) The cyst wall appears greyish-yellow, with a smooth inner and outer surface. (c and d) The cyst wall consisted of smooth muscle and fibrous tissue, lined with mucinous columnar epithelium. Localized epithelial loss was noted, accompanied by thinning of the cyst wall with a glassy appearance.
Subsequently, the cyst was incised to allow drainage of bile for decompression. After extracting its contents, we entered the cyst through the incision in its anterior wall and coagulated the posterior wall of the cyst. We observed the presence of newly formed capillaries attached to the cyst wall. Importantly, the magnification capability of the laparoscope assisted us in dissecting this newly formed capillary bundle. In performing dissection of the distal end of the cyst, the lead surgeon lifted the wall of the duct upwards. The assistant surgeon moved the liver upwards, and suction was used to push downwards on the duodenum and head of the pancreas to maintain proper tension that existed between the wall of the cyst and the surrounding tissues. The cyst wall was carefully detached from its surroundings by pressing firmly against the side of the dilated cyst wall. This was done to avoid damaging the pancreas. We dissected the common bile duct and subsequently sutured the dissected area. The proximal end of the cyst was transected using a similar method. Subsequently, continuous suturing of the residual end was performed using 3-0 barbed suture. Following incision and repair of the bile duct at the proximal common hepatic duct, the hepatic duct and the jejunum were anastomosed. The jejunum-jejunum anastomosis was performed at a distance of 40–45 cm from its proximal end. After washing the abdominal cavity, drainage tubes were placed, at the Winslow hole below the biliary-enteric anastomosis, at the anterior wall of the biliary-enteric anastomosis, and at the vicinity of the jejunum-jejunum anastomosis. Finally, the abdomen was closed.
The removed cyst was sent for pathological examination (Figure 2b). The cyst wall appeared greyish-yellow, with a smooth inner and outer surface. Microscopically, the cyst wall consisted of smooth muscle and fibrous tissue, lined with mucinous columnar epithelium. Histopathology of the specimen showed localized epithelial loss, accompanied by thinning of the cyst wall with a glassy appearance (Figure 2c and 2d).
Repeat blood tests post-operation showed several parameters had decreased from pre-operation values. These were: total bilirubin, 77 μmol/l; direct bilirubin 45.6 μmol/l; indirect bilirubin 31 μmol/l; alkaline phosphatase 123 U/l; GGT, 190 U/l. However, some values had increased (i.e., alanine aminotransferase, 205.3 U/l and aspartate aminotransferase 207.9 U/l). The elevation in these liver enzymes is typically a physiological response to surgery because the procedure may cause some degree of liver damage. The elevation in values is usually transient, and the levels of both enzymes gradually return to normal as the patient recovers. Although, the white blood cell (WBC) count was also slightly higher than pre-operation levels, this was considered to be related to stress following surgery, and values quickly returned to normal levels. A follow-up CT scan post-operation, showed the drainage tube was unobstructed (Figure 3). On the first day post-surgery, the drainage amounts from the three tubes were 200 ml, 180 ml, and 70 ml, and the colour of the fluid was pale red. Drainage gradually decreased daily and tubes were removed on Day 5. The patient recovered well and was discharged from hospital on Day 8 without any complications. She attended follow-up visits after one and three months post-operation, and her recovery was assessed as excellent. The reporting of this study conforms to CARE guidelines. 7 The patient provided consent for publication of her anonymised data. Ethical committee approval was not required for this case report.

The drainage tube was unobstructed. On the first day after surgery, the drainage amounts from the three tubes were 200 ml, 180 ml, and 70 ml, and the colour of the fluid was pale red. The drainage gradually decreased each day until the tubes were removed on Day 5.
Discussion
Although the aetiology of choledochal cysts is uncertain, some researchers have attributed their phenomenon to an anomalous formation of the pancreaticobiliary ductal junction. 8 Due to a narrow diameter of the pancreatic duct and the presence of high pressure, pancreatic secretions flow back to the choledochal duct. Consequently, the mixture of pancreatic fluid and bile, activates pancreatic enzymes. As the pressure increases, the activated pancreatic enzymes trigger the occurrence of inflammation, and gradually degrade the bile duct wall. This ultimately leads to bile duct dilatation and development of abnormalities. Although uncommon, with an incidence of 1 in 100,000–150,000 live births in the western population, the incidence of choledochal cysts in Asian nations has been reported to be as high as 1:1000.1,9 Women are more frequently affected, with a male-to-female ratio of 1:3 or 1:4.1,9 The majority of cases are diagnosed in childhood, with approximately 25% of cases detected in adulthood. 9 With regard to giant choledochal cysts, there is a lack of data because of their extremely low incidence.
Although symptoms of abdominal pain, palpable abdominal mass, and jaundice are present in approximately 20% cases, for many adult patients the clinical presentation of choledochal cysts is often vague and nonspecific.1,9,10 However, the main manifestations of giant choledochal cysts do tend to include abdominal pain and a palpable mass.6,11,12 In addition, the occurrence of jaundice is also greater in cases with a giant choledochal cyst compared with cases of generally sized choledochal cysts. 6 Consistent with these findings, our patient experienced right upper abdominal pain, mild jaundice, and a smooth-surfaced cystic mass was detected during her physical examination.
Among patients with generally sized choledochal cysts, complications such as pre-operative acute pancreatitis are more commonly observed in children with poor pancreaticobiliary connections (30%), while studies have shown that adults experience acute pancreatitis in only 9% of cases. 13 Post-operative complications often involve hepaticoenterostomy anastomotic leakage and anastomotic stenosis, which are relatively common. 14 Although uncommon, approximately 3–5% patients developed biliary cancer after surgical excision. 14 Importantly, for patients with type I or type IV cysts, there is a relatively high risk of malignant tumors.8,15 Little data exist on complication rates associated with giant choledochal cysts. In our case, the patient did not have any pre-operative, or, post-operative complications. Pathological examination of the specimen following excision showed no signs of anastomotic leakage, anastomotic stenosis, or malignancy. We believe that post-operative complications such as anastomotic leakage and anastomotic stenosis may be caused by improper surgical manoeuvres. In our case, the drain position was skilfully placed, it drained well and anastomosis was successful. The drainage tube was removed five days after surgery and the patient was discharged from hospital three days later without any complications.
In terms of diagnosis of the giant cyst, we used blood investigations and imaging techniques. Blood tests can show abnormal liver function in patients with cholangitis caused by the choledochal cysts. 9 Increases in serum amylase can indicate the presence of pancreatitis, and changes in coagulation profile and renal function may reflect the severity of the disease. 9 For biliary system diseases, abdominal ultrasound is the preferred auxiliary examination, and CT scans are often used to understand the structure of the biliary tract. 9 Due to its high specificity of approximately 90% to 100% and sensitivity of 70% to 100%, MRCP is considered the best option for pre-operative diagnosis and identification of the biliary tract. 9 In our case, blood test results showed elevated liver function parameters. These findings together with imaging examinations, confirmed our diagnosis of a giant choledochal cyst and it was classified as type IVa.
Typically, surgical management through cyst excision is the mainstay of treatment for choledochal cysts. Its purpose is to remove the cyst completely and restore biliary enteric drainage into the duodenum or through Roux-en-Y hepatojejunostomy. 16 While reports on excision of giant choledochal cysts are scarce, open surgery appears to be a common surgical technique. However, two studies have shown that laparoscopic dissection of giant cystic cysts is feasible and surgeons can successfully completed the procedure without complications.3,17 Indeed, several studies have concluded that that laparoscopic surgery for choledochal cysts is safe, feasible, and advantageous.9,18 In our case, after evaluating the feasibility of using laparoscopy for stripping surgery and excluding surgery-related contraindications, we successfully performed laparoscopic resection of a giant choledochal cyst. Based on our pre-operative imaging examinations, the cyst had expanded to below the confluence of the right and left hepatic ducts. Similar to a previous study, the proximal resection line was extended to the fusion point of the left and right hepatic ducts for the removal of a type IVa cyst. 19 However, we preserved approximately 1 cm of the common bile duct, where the diameter measured approximately 1.5 cm. This decision was made due to the large size of the cyst. To prevent complications, such as cyst rupture and damage to surrounding tissue, a front wall incision suction decompression technique was used.
In summary, giant choledochal cysts are rare. Surgical resection of giant cysts is challenging with risks of post-operative complications such as biliary leakage, pancreatitis, pancreatic leakage and fistula. 1 We successfully performed a laparoscopic resection of type IVa giant choledochal cyst with a size of about 129 mm × 190 mm. The patient recovered well, and at three months after the operation was assessed as having excellent good health.