
Abstract
Differentiation between granulomatosis with polyangiitis (GPA) limited to the upper airways and cocaine-induced midline destructive lesion (CIMDL) may be particularly difficult because of their common histopathologic features and antineutrophil cytoplasmic antibody (ANCA) profiles. We herein present a case involving a young woman with an initial diagnosis of GPA based on upper and lower airway manifestations and constitutional symptoms, histopathologic evidence of granulomas, a positive cytoplasmic ANCA indirect immunofluorescent test result, and proteinase 3 positivity by enzyme-linked immunosorbent assay (ELISA). CIMDL was confirmed based on the appearance of a hard palate perforation, positivity for methylecgonine on urine toxicology, a positive perinuclear ANCA indirect immunofluorescent test result, and subsequent human neutrophil elastase (HNE) ANCA positivity by ELISA. Finally, based on the coexistence of CIMDL, constitutional symptoms, and lower airway manifestations, the diagnosis was modified to cocaine-induced GPA mimic. Urine toxicology for cocaine and HNE ELISA are indicated in young patients with GPA who develop limited airway disease to check for the presence of CIMDL and cocaine-/levamisole-induced ANCA-associated vasculitis. Continued abstinence from cocaine is the first-choice therapy for both CIMDL and cocaine-induced GPA mimic.
Keywords
Introduction
Multiple autoimmune diseases (particularly granulomatosis with polyangiitis [GPA], sarcoidosis, relapsing polychondritis, and immunoglobulin G4-related disease), fungal and bacterial infections (including invasive fungal rhinosinusitis, rhinosporidiosis, rhinoscleroma, syphilis, tuberculosis, leprosy, and leishmaniasis), malignancies (e.g., extranodal natural killer/T-cell lymphoma, nasal type), and drug abuse (particularly compulsive cocaine snorting) may cause significant necrosis of the nasal mucosa and underlying osteocartilaginous structures, resulting in nasal septal perforation and crusting. 1 With the exception of infections that are endemic to certain geographical regions, the above-mentioned conditions are rare and share overlapping symptomatology and histopathological findings. Systemic or characteristic organ manifestations, histologic examination with special stains, immunohistochemistry, and cultures may support the diagnosis of some of these diseases.
Differentiation between GPA limited to the upper airways and cocaine-induced midline destructive lesion (CIMDL) may be particularly difficult because of their common histopathologic features and antineutrophil cytoplasmic antibody (ANCA) profiles. CIMDL is a localized destructive midline condition that is initially centered on the anterior nasal cavity and subsequently exhibits centrifugal expansion.2,3 Furthermore, only classification criteria exist for GPA; therefore, its diagnosis is based on the combination of clinical, histopathological, and serological findings. 4
The present case report highlights the importance of conducting a thorough and extensive workup before conclusively diagnosing GPA and initiating immunosuppressant therapy. This caution is crucial because of the high prevalence of recreational drug use, which can result in syndromes that mimic GPA.
Case presentation
The reporting of this study conforms to the CARE guidelines. 5 Written consent for treatment and publication were obtained from the patient.
In April 2022, a woman in her late 30s presented to an ear-nose-throat (ENT) outpatient department because of nasal obstruction, bloody purulent discharge, scabs, and facial pain. Cranial computed tomography (CT) for evaluation of transient right-sided blurred vision in 2020 had shown mucosal swelling and an air–fluid level in the left maxillary sinus as incidental findings. At the initial ENT examination, extensive nasal crusting and a perforation of the anterior two-thirds of the nasal septum were found. During the subsequent 12 months, eight additional ENT examinations were performed. Colonization by Staphylococcus aureus developed in her nasal cavity. Despite conservative treatment (debridement, repeated targeted antibiotics, intranasal steroids, and saline nasal douching), her condition persisted. In March 2023, additional bony destruction of the left inferior and middle turbinates was detected by rigid nasal endoscopy. By that time, the patient had also developed constitutional symptoms including fatigue, weight loss, and polyarthralgia. Histopathological analysis of multiple nasal biopsy specimens (Figure 1(a)) showed active chronic inflammation with an abortive extravascular granulomatous component. Extensive geographical necrosis, bone destruction, and reactive fibroblast proliferation were also present. Some giant cells were detectable within the histiocyte-rich inflammatory infiltrate. A single birefringent foreign particle was found in the necrotic area. Necrotizing vasculitis was suspected only in a proportion of small vessels. Overall, the patient’s findings did not fulfill the morphological diagnostic criteria for GPA.

Histopathology and indirect immunofluorescence. (a) Histopathology showed extensive geographical necrosis (hematoxylin–eosin, 10×) with CD68-positive giant cells (upper right inset, 94.7×). Necrotizing vasculitis had arisen in only a small vessel (lower left inset, hematoxylin–eosin, 63×) and (b) indirect immunofluorescence ANCA test on ethanol-fixed granulocytes (400× magnification) demonstrated a weak diffuse cytoplasmic ANCA pattern and a strong perinuclear ANCA pattern. ANCA, antineutrophil cytoplasmic antibody.
It should be noted that indirect immunofluorescence for ANCAs showed a weak diffuse cytoplasmic (C-ANCA) pattern and a strong perinuclear (P-ANCA) pattern (Figure 1(b)), while enzyme-linked immunosorbent assay (ELISA) was highly positive for proteinase 3 (PR3) (324 U/L; reference range, <10 U/L) and negative for myeloperoxidase (MPO) antibodies. The patient was referred to our department of rheumatology with a diagnosis of GPA, and we performed further investigations to screen for its other manifestations. Chest CT showed multiple sub-centimeter peripheral nodules, but no evidence of renal involvement was found. The QuantiFERON-TB Gold test showed weak positivity (with interferon-gamma release of 0.44 IU/mL), but Ziehl–Neelsen staining, Mycoplasma tuberculosis complex-specific polymerase chain reaction, and subsequent mycobacterial cultures of the bronchoalveolar mucus excluded tuberculosis. The maximum C-reactive protein concentration was 55.30 mg/L, and her blood cell counts were normal except for mild leukocytosis and thrombocytosis. Considering the 2022 American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) classification criteria for GPA, the patient’s findings were highly specific for GPA (score of 14). 4 Her initial Birmingham Vasculitis Activity Score (version 3) was 14 points. 6 Tests for other autoantibodies (antinuclear antibody, Sm, Sm/RNP, SS-A, SS-B, Scl-70, and Jo-1) and infections (Treponema pallidum, Aspergillus, and hepatitis B and C viruses) were negative.
The patient tested positive for human immunodeficiency virus (HIV) without obvious signs of acquired immunodeficiency syndrome and with a normal CD4 count (176–407 cells/µL). Following the introduction of combined glucocorticoid therapy (starting dose of 1 mg/kg and stepwise reduction by month 3), the patient began oral methotrexate therapy (15 mg/week) for remission induction as well as highly active antiretroviral therapy (HAART).
Within 4 weeks (during the oral glucocorticoid tapering period), the patient presented to our ENT department with recurring constitutional symptoms and complaints of rhinolalia and nasal reflux. Examination revealed an incipient saddle nose deformity (Figure 2(a)), mild broadening of the nasal root and dorsum (Figure 2(b)), a newly developed 23-mm hard palate perforation (Figure 2(c)), and persistent nasal crusting. Sinus CT showed extensive destruction of the left lateral nasal wall, the cartilaginous and bony nasal septum, and the hard palate defect (Figure 3). The patient was referred to our department of rheumatology again with active GPA and suspected CIMDL, although she denied cocaine consumption. Rituximab was initiated for remission re-induction at 375 mg/m2 body surface area per week for 4 weeks. Five days later, a urine toxicology test was positive for methylecgonine, a metabolite of cocaine. The patient admitted to “occasional” snorting of cocaine during the past 2 years. Repeated ELISA of minor ANCA antibodies was highly positive for human neutrophil elastase (HNE) ANCA (ratio, 7.7; reference range, <1.0). Antibodies to lactoferrin, cathepsin G, and bactericidal/permeability-increasing protein were not detected. Three weeks after the last rituximab dose, control nasal endoscopy showed extensive osteocartilaginous destruction (Figure 2(d)) with resolution of the nasal crusting. Her persistent hard palate perforation was treated with an obturator prosthesis. At the time of this writing, the patient was in clinical remission on maintenance therapy with methotrexate, and she claimed cocaine discontinuation.

Nasal findings. (a) An incipient saddle nose deformity was visible in profile. (b) The nasal root and dorsum were mildly broadened in the front-view photograph. (c) A 23-mm hard palate perforation was observed within 4 weeks of initiation of remission induction therapy by glucocorticoid and methotrexate and (d) nasal endoscopy was performed with a 0° rigid endoscope 5 weeks after the initiation of remission re-induction therapy by rituximab. C, choana; IT, inferior turbinate; MS, maxillary sinus; MT, superior turbinate; PP, palatal perforation; S, septum; ST, superior turbinate.
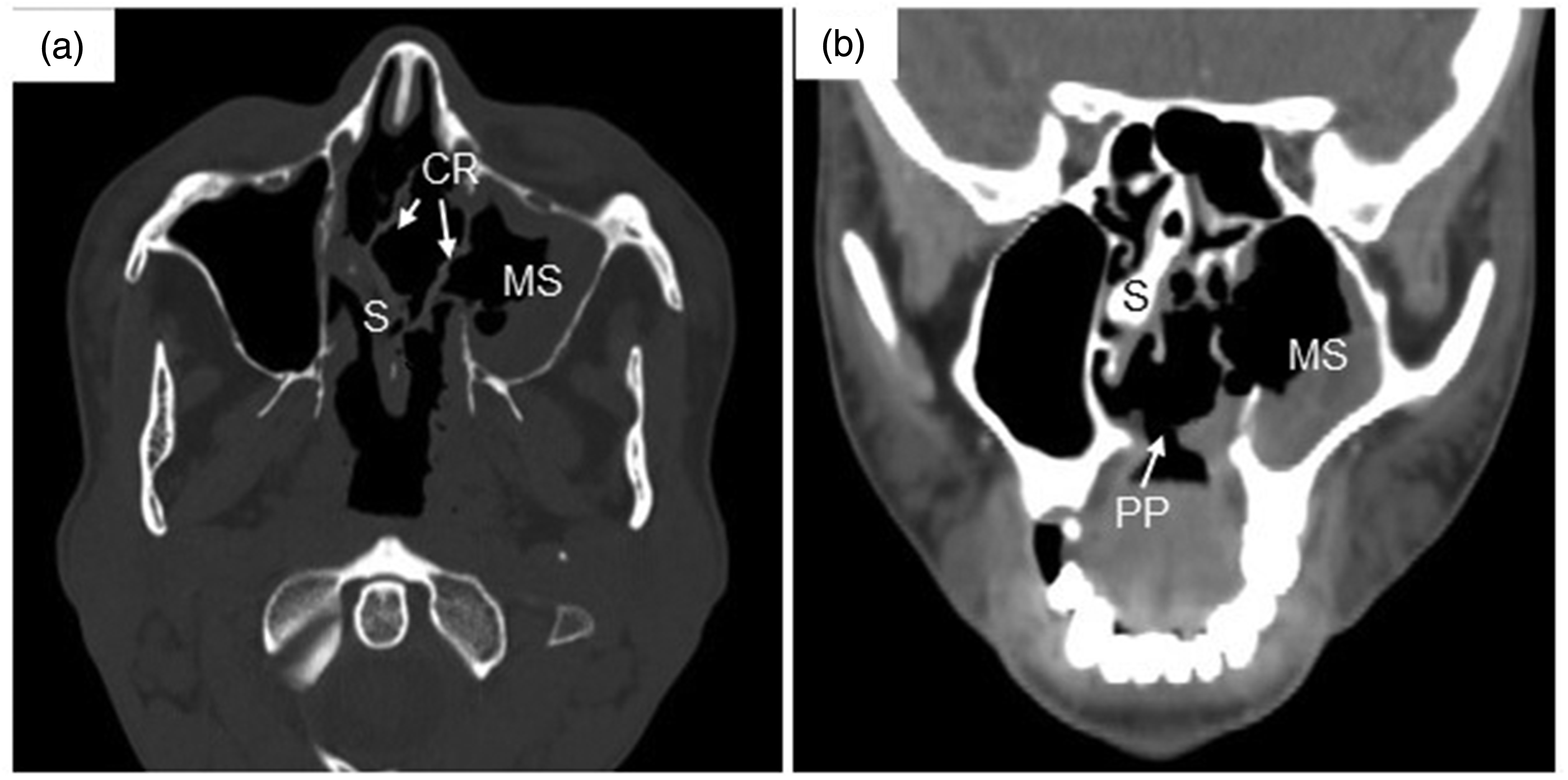
Sinus computed tomography findings (a) axial and (b) coronal plane images. CR, crusts; MS, maxillary sinus; PP, palatal perforation; S, septum.
Discussion
At the time of diagnosis of vasculitis in our case, the 2022 ACR/EULAR classification criteria should not have been applied prior to excluding alternate diagnoses that mimic vasculitis. 4 CIMDL and cocaine-/levamisole-induced vasculitis are representative GPA mimics.
According to the World Drug Report by the United Nations Office on Drugs and Crime, the prevalence of cocaine consumption in Hungary is low (0.3% among women and 0.5% among men in the 18- to 64-year age group in 2019). 7 The most frequent route of administration of powdered cocaine is snorting; thus, nasal adverse effects are very common. 8
Time- and dose-dependent local vasoconstriction, mechanical trauma from high-velocity inhalation, and the application of foreign bodies to remove scabs result in tissue necrosis; this may be compounded by S. aureus superinfection.2,8 Although the above causes affect all compulsive cocaine users, only a subset (<5%) develop CIMDL. The key factor in the pathogenesis of CIMDL is an ANCA-associated vasculitis caused by the cocaine itself and levamisole, a cocaine adulterant. 8 Both cocaine and levamisole may contribute to the development of ANCAs by inducing the release of potentially inflammatory neutrophil extracellular traps. 9 In patients with CIMDL, ANCAs primarily react with HNE displaying P-ANCA staining in the indirect immunofluorescence test, but they do not react with MPO in ELISA. HNE shares epitopes with PR3, resulting in false positivity in PR3-ELISA and finally a discordant P-ANCA–PR3 pattern. 9 However, a concordant C-ANCA–PR3 pattern is highly specific for GPA. 10 Our patient showed both patterns.
Several histopathological features are shared between CIMDL and GPA, 3 including mixed inflammatory infiltrates, microabscesses in vessel walls, vascular microthrombosis, fibrinoid necrosis. The characteristic histopathological findings of GPA (necrosis, intravascular and extravascular granulomas, and vasculitis) are evident in only 20% of ENT biopsy specimens from patients with GPA. Apoptotic cells are considered highly specific for CIMDL. 11 In our case, the histologic examination did not show an abundance of apoptotic cells; however, specific tests for apoptosis (e.g., in situ terminal deoxynucleotidyl transferase-mediated dUTP nick end labeling [TUNEL]) were not performed. Taking multiple large biopsies from the edges of lesions may help to differentiate GPA and CIMDL.2,8
Some reports of CIMDL have described centrifugal expansion starting from the nasal septum and extending to the inferior and middle turbinates and the hard palate.8,12 This pattern was followed up in our patient by serial ENT examinations and CT scans. According to the four-grade destruction location-based classification proposed by Nitro et al., 13 our case corresponds to grade 3 CIMDL. Extensive local destruction is unlikely in GPA, and hard palate perforation is more strongly indicative of CIMDL. 11
In our case, the diagnosis of CIMDL was unequivocal (positive urine toxicology, extensive destruction and perforation of the palate, HNE-ANCA positivity), and simultaneous GPA was seemingly also confirmed (upper and lower airway manifestations and constitutional symptoms, histopathologic granulomas, and C-ANCA–PR3 pattern). However, the GPA diagnosis raises a further differential diagnostic issue: the combination of two drug-associated ANCA vasculitides, namely those induced by cocaine and levamisole. Levamisole, currently used as a veterinary anthelmintic agent and historically used as an immunomodulatory and adjuvant chemotherapeutic agent, has been reintroduced for human use in the past two decades. It is now being used in about 70% of illicit cocaine samples to augment bulk and enhance cocaine-induced euphoria.14,15 Levamisole induces a systemic ANCA-associated small vessel vasculitis characterized by retiform purpura of the ears and lower extremities, agranulocytosis, constitutional symptoms, and renal and pulmonary disease with sub-centimeter pulmonary nodules in the latter. 9 In fact, CIMDL and levamisole-induced vasculitis cannot be distinguished, resulting in a syndrome mimicking GPA. In our patient, the symptoms of levamisole-induced vasculitis could not be detected apart from pulmonary nodules. Our patient’s lesions were more likely cocaine-induced mimics of GPA. 16 A recent study retrospectively analyzed 42 patients (median age, 41 years) disclosing cocaine use or producing positive urine toxicology for cocaine and showing symptoms suggestive of ANCA-associated vasculitis. 16 Most of the patients were ANCA-positive by ELISA and/or indirect immunofluorescence, and 53% of the patients tested positive for PR3 by ELISA but none tested positive for MPO. Concordant C-ANCA–PR3 and discordant P-ANCA–PR3 patterns were detected in nine and seven patients, respectively. HNE ELISA was not performed. The authors termed this condition “cocaine-induced GPA,” referring to a cocaine-induced mimic of GPA as elucidated in the discussion of their paper. These patients with cocaine-induced GPA mimic were 20 years younger than patients with idiopathic GPA and showed predominantly ENT symptoms. 16
Although the prevalence of autoantibodies in HIV-infected patients is high (20%–83%), vasculitis is reportedly rare (<1%) in the current HAART era. 17 In a recent review, the rate of ANCA positivity in HIV-infected patients ranged from 13% to 83%; however, clinical vasculitis was absent in most patients, and only one patient showed sinusitis. 18 In our patient, the HIV positivity was diagnosed simultaneously with the systemic ANCA-associated vasculitis, and HAART was started without delay. The CD4 cell count remained normal, and the HIV-1 RNA copy numbers detected by real-time polymerase chain reaction were consistently low (<20 copies/mL). Therefore, we do not attribute a significant role of HIV infection in the etiology of ANCA-associated vasculitis.
The cornerstone of therapy in patients with CIMDL and cocaine-induced mimic of GPA is continued abstinence from cocaine (and levamisole).8,16 Immunosuppressive therapy has no role in CIMDL. 8 For cocaine-induced mimic of GPA, one strategy is to offer immunosuppression if the patient remains symptomatic after cocaine cessation; however, other clinicians use immunosuppression routinely if GPA is diagnosed. 16 Immunosuppression was indicated in our patient because of her severe constitutional symptoms and lower airway manifestation. An obturator prosthesis is an ideal option to overcome oronasal reflux, but surgical reconstruction may be required after 6 to 12 months of abstinence. 8
In conclusion, CIMDL should be suspected in patients with extensive sinonasal destruction, centrifugal expansion, and particularly palatal perforation. Urine toxicology for cocaine is indicated in young patients diagnosed with GPA with limited or dominant upper airway disease. HNE-specific ELISA is recommended to support the diagnosis of cocaine- and levamisole-induced ANCA-associated vasculitis. Continued abstinence is the first-choice therapy for both CIMDL and cocaine-induced mimic of GPA.
Footnotes
Author contributions
Drafting of the manuscript: TM and SS. Revision of the manuscript: HM, GS, and ZS. Collection and/or analysis of the data: TM, GN, JS, HM, and SS. All authors read and approved the final manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare the there are no conflicts of interest.
Ethics statement
This study was approved by the Hungarian Scientific Research Council Ethical Committee (approval No: 6768/2024). The study was performed according to the Good Clinical Practice guidelines and the latest Declaration of Helsinki. The patient’s clinical data are kept in accordance with the EU General Data Protection Regulations, or other counterparts, on the processing of personal data and the protection of privacy (2016/679/EU). Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.