
Abstract
Intraventricular haemorrhage (IVH) is a severe and acute type of stroke with a complex pathophysiology and is a therapeutic challenge. This case report described a man in his early 50’s diagnosed with IVH by computed tomography (CT). Although bilateral extraventricular drainage (EVD) was undertaken, a postoperative CT scan showed that while the left catheter was correctly positioned, the right catheter had been wrongly inserted into the cisterna ambiens. The procedure was equivalent to simultaneous EVD combined with cisternostomy. As a consequence, the haematoma was rapidly removed, the risk of infection and long-term hydrocephalus was reduced, and prognosis was improved. Large case-control studies or prospective studies are needed to evaluate the safety and effectiveness of this treatment modality.
Background
Intraventricular haemorrhage (IVH) is a severe and acute type of stroke with a complex pathophysiology and is a therapeutic challenge. 1 IVH is associated with high mortality and morbidity. 2 One study found that only 38% of patients survived the first year after the stroke, and most survivors had disabilities. 3 IVH can be classified as primary or secondary categories according to the source of the hemorrhage. 4 Haemorrhages that have ventricular involvement are defined as secondary IVH. Primary IVH occurs within the ventricles without parenchymal involvement and is rare, and accounts for only 3 to 7% of cases of intracerebral haemorrhage (ICH).4, 5 Risk factors for IVH include: hypertension; Moyamoya disease; cerebral aneurysms; arteriovenous malformation (AVM); small vessel disease; clotting disorders; antithrombotic use.6,7 For patients with both IVH and ICH, the expected mortality is 50% to 80%. 2 Poor prognosis of IVH involves elevated intracranial pressure (ICP), obstructive hydrocephalus, direct compression of haematoma, and exposure to toxic blood degradation products. Therefore, effective clearing of the intraventricular haematoma can significantly improve patients’ outcome.8,9
Several surgical procedures have been used for removal of the IVH, including craniotomy, endoscope assisted haematoma removal, haematoma evacuation by stereotactic puncture, and lumbar drainage.2,4 Their objective is to eliminate the intraventricular haematoma, reduce its damage and improve prognosis. Extraventricular drainage (EVD), whereby cerebrospinal fluid (CSF) and blood is drained to clear the haematoma, relieves early obstructive hydrocephalus and reduces damage caused by the haematoma, is a commonly used method. 10 However, complications, such as haemorrhage in the puncture tract, infection, repeated flushing or replacement of catheter due to blood clot blockage, can affect the drainage effect.10,11 Studies have shown that combining EVD with thrombolytic therapy shows beneficial effects in some patients with IVH but the risk of haemorrhagic complications is slightly increased.9,12,13
We report here, a case of a man in his early 50’s with primary IVH who was planned to have a bilateral EVD. However, a postoperative computed tomography (CT) scan showed that while the position of left catheter was correct, the right catheter had been incorrectly inserted into the cisterna ambiens. Both catheters were unobstructed at all times. We suggest that this unexpected procedure, that achieved a satisfactory curative effect, was equivalent to simultaneous EVD combined with cisternostomy.
Case report
A man in his early 50’s attended the emergency room of the Second Affiliated Hospital of Zhejiang University School of Medicine following a sudden headache for more than four hours and unconsciousness for 30 minutes. The patient reported that the headache started suddenly following carrying heavy objects and had gotten worse over the last hour and was accompanied with nausea and vomiting. Initially, the patient was sent to a local hospital for a head CT scan, which showed presence of IVH. He was subsequently transferred to our hospital. Over the first half an hour after arrival at our hospital, the patient developed further confusion. Physical examination showed: lethargy; irrelevant answers; Glasgow coma scale (GCS) score 9; equal size of bilateral pupils, 2.0 mm in diameter and of slow reflection to light; involuntary movement of limbs. The patient had a history of hypertension over the past five years but did not take medication for it and so his blood pressure (BP) was uncontrolled.
A head CT scan showed haematoma within the ventricular system including the lateral, third and fourth ventricles which were dilated. (Figure 1). CT angiography of the head showed no vascular malformations or aneurysms. A bilateral EVD was performed. On the left side, bloody CSF outflow was seen following introduction of a catheter 6.0 cm beyond its tip. However, on the right side, CSF outflow was not observed after repeated punctures to a depth of 6.0 cm. Following insertion of the catheter to 10.0 cm beyond its tip, there was a significant sense of breakthrough, and bloody CSF outflow was observed. Notably, CSF drainage fluctuated significantly on both sides (Figure 2).
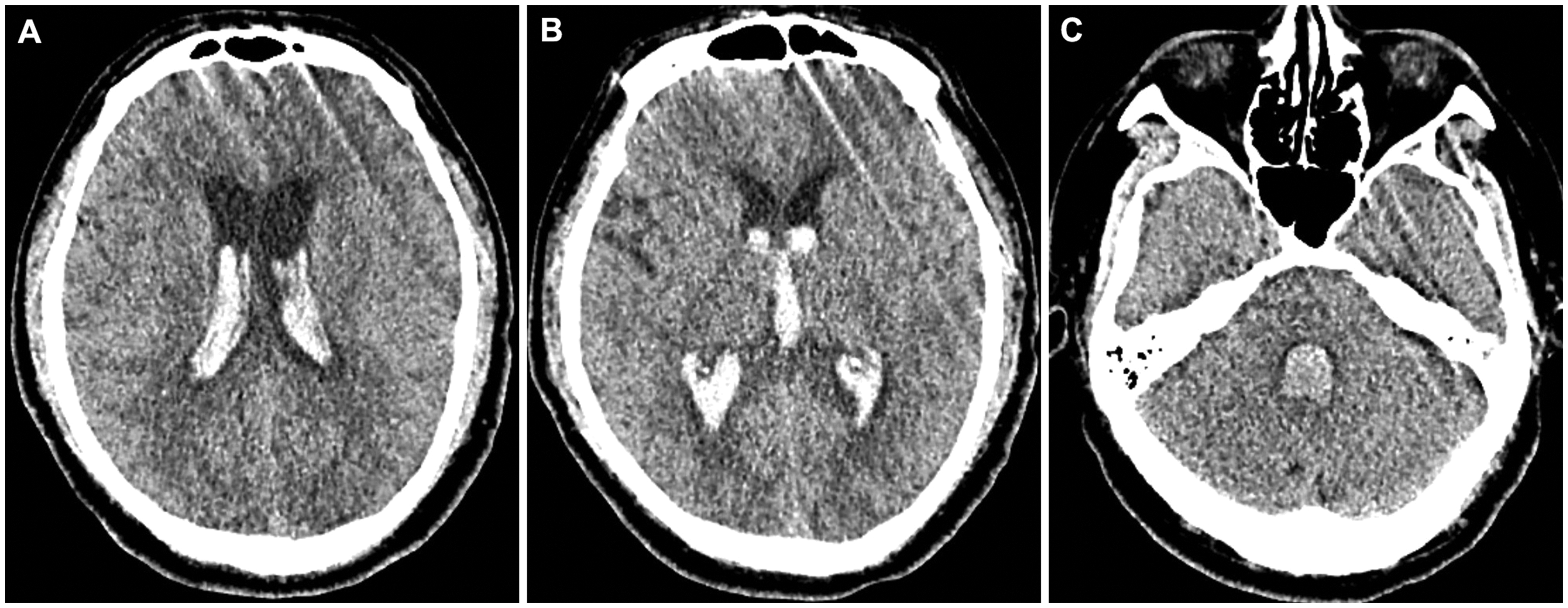
Head CT scan showed haematoma within the ventricular system including the lateral, third and fourth ventricles which were dilated. (a) Lateral ventricular body level; (b) third ventricle level and (c) fourth ventricle level.

(a) The scalp incision mark for the extraventricular drainage (EVD); (b) the catheters were placed into the ventricles and (c) bloody cerebrospinal fluid (CSF) in the catheters on both sides.
Post-operation, the patient was admitted to the intensive care unit (ICU), and a total of 200 ml CSF was drained every day. A further head CT scan showed that the left catheter was located in the ventricle, whereas the right catheter had passed through the lateral side of the right lateral ventricle, posterior limb of inner capsule, and entered the cisterna ambiens (Figure 3).

Head CT scan post operation showed that the left catheter was located in the ventricle, while the right catheter had passed through the lateral side of the right lateral ventricle, posterior limb of inner capsule, and entered into the cisterna ambiens. (a) Lateral ventricular body level; (b) third ventricle level; (c) cisterna ambiens level and (d) fourth ventricle level.
Post-operation, the patient's consciousness gradually improved. Three days later, the patient's GCS score was 12, and his muscle strength in his left upper limb was grade 3. After two more days a head CT scan showed that the haematoma was significantly reduced, and only a small amount remained in the posterior horn of the lateral and fourth ventricles. There was no obvious enlargement of the ventricles, suggesting that the CSF circulation was unobstructed (Figure 4). On the sixth day post-operation, the right catheter was removed and the patient was transferred out of ICU; his left catheter was removed a day later. His muscle strength of his left upper limb gradually recovered and reached grade 5. On Day 10 post-operation, a head CT scan showed that the haematoma had completely dissipated; there were no obvious signs of ventricular dilatation and the cerebral sulci and cistern were clear (Figure 5). Two days later, on Day 12, the patient was discharged from hospital.

Head CT scan showed that the haematoma had significantly reduced, only a small amount remained in the posterior horn of the lateral and fourth ventricles. There was no obvious enlargement of the ventricles. (a) Lateral ventricular body level; (b) third ventricle level and (c) fourth ventricle level.

Head CT showed that the haematoma was completely dissipated, there was no obvious ventricular dilatation, and the cerebral sulci and cistern were clear. (a) Lateral ventricular body level; (b) third ventricle level and (c) fourth ventricle level.
The patient had a good prognosis and no obvious sequelae. Examination of CT scans taken one and three months post-operation showed no signs of brain hydrocephalus or any other obvious abnormalities. In the third month post-operation, the patient’s GCS score was 15 and his Modified Rankin Score (mRS) score was 0.
The reporting of this study conforms to CARE guidelines. 14 Written informed consent was obtained from the patient for publication of his anonymised data. This report was approved by the clinical ethics committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (NO.2022-0694).
Discussion
EVD is a suitable procedure for IVH and acute hydrocephalus, and can quickly relieve elevated ICP and save lives. 10 Importantly, it can be used with a device to monitor ICP. 10 In addition, EVD can also be used to release CSF before an operation, which is helpful for neurosurgeons. EVD is one of the basic skills that neurosurgeons should master.15,16 The puncture point is called Kocher point, and is located 10.0–11.0 cm behind the nasal root, 3.0 cm near the midline and 1.0 cm before the coronal suture. 17 The catheter should be directed at an angle that is perpendicular to the intersection of lines drawn from the ipsilateral medial canthus and the ipsilateral external auditory meatus. The catheter should enter the skull vertically, to a depth approximately 6.0 cm away from the scalp. After the catheter tip passes through the ependyma, there will be a sense of breakthrough, and the CSF should flow out. Following removal of the needle, the catheter should be inserted for another 1.0 cm to reach Monro foramen. 18 If the catheter advances more than 7.0 cm, the puncture angle may be incorrect or the tip of the catheter may enter the temporal angle, longitudinal fissure, third ventricle, lateral fissure and even basal cistern. If this happens, it will be necessary to adjust the catheter position and tilt it slightly towards the middle and rear of head. 18 Insertion of the EVD is a ‘blind procedure’ and based on approximate external anatomical features. Therefore, inexperienced doctors are prone to inaccurate positioning that can result in puncture failure, especially in patients with small ventricles. Stereotactic, navigation, and even robot assistance may be required in some instances. 19 In our case, we punctured based on experience without any auxiliary methods. After failing to puncture with multiple angle adjustments, our only option was to puncture deeper, and we finally achieved CSF outflow. The puncture into the cistern was an accidental gain. Our right catheter had passed through the lateral side of the right lateral ventricle, posterior limb of inner capsule, and entered into the cisterna ambiens. Usually, if cisternostomy is planned, stereotactic navigation is essential.
We can learn three important lessons from our case study. Firstly, the puncture point was too lateral, and the ventricle dilatation was not obvious, which lead to a lateral puncture path and failure to enter the ventricle. Secondly, there was no sense of breakthrough or CSF outflow after the catheter had been inserted to a depth of 7.0 cm. In hind sight, we should have adjusted the puncture direction and started again rather than continued along our original path. Deep punctures can easily damage important structures in the brain. Thirdly, when there is no navigation system, stereotactic devices or other assistance during an operation, it is necessary to measure distances carefully between the anterior horn of the lateral ventricle and the midline on a CT scan.
Cisternostomy has been increasingly used in cases of traumatic brain injury (TBI), subarachnoid haemorrhage, arteriovenous malformation (AVM) rupture, tumour, cerebral haemorrhage, and hydrocephalus.21–23 Cisternostomy reduces ICP by opening the cistern in the skull base, including the optic chiasmatic cistern, carotid cistern, endplate cistern, anterior pontine cistern, to release CSF. Cisternostomy causes CSF to move from the swollen brain to the cistern through the Virchow-Robin space, so that the ICP can be decreased effectively. To our knowledge, there is no previous report of cisternostomy for the treatment of IVH. We suggest that cisternostomy has several advantages in the treatment of IVH. For example, the drainage is in line with the normal flow direction of CSF, conforming to physiological requirements. Compared with lumbar drainage, the risk of cerebral hernia will be minimal. In addition, by opening the cistern in the skull base for continuous drainage, a large number of blood clots and bloody CSF can move back in the Virchow-Robin space, and the obstruction of CSF circulation path can be relieved; this will not only reverse CSF shift oedema and reduce ICP, but also improve vascular compliance and reduce the risk of vasospasm. 24 Another advantage of cisternostomy is that the drainage will help remove harmful metabolites such as, lactic acid, oxygen free radicals, tumour necrosis factor-α, (TNF-α), interleukin-10 (IL-10), IL-6 and other inflammatory mediators.25,26 This will reduce the harmful cellular environment, oxidative stress, inflammatory response, and brain oedema.
In the case study presented here, the left catheter was placed correctly into the lateral ventricle, but the right catheter was placed incorrectly into the cistern, which was equivalent to EVD combined with cisternostomy. Therefore, the ventricle and subarachnoid space were drained simultaneously. As a consequence, the haematoma was rapidly removed, and the patient recovered quickly so reducing the risk of subsequent hydrocephalus. Large case-control studies or prospective studies are needed to evaluate the safety and effectiveness of this particular treatment for IVH.