
Abstract
Persistent hyperplastic primary vitreous (PHPV) is a rare congenital developmental ocular disorder caused by incomplete regression of the embryonic hyaloid vasculature; bilateral presentations are even rarer. We report a 6-year-old child with bilateral PHPV who visited our hospital for strabismus, without exhibiting leukocoria, microphthalmia, and systemic diseases. These unique characteristics distinguish our case from other cases of PHPV. It is crucial to increase awareness of congenital eye disease in children and the importance of performing fundus examination with the pupils dilated.
Keywords
Background
Persistent hyperplastic primary vitreous (PHPV), also known as persistent fetal vasculature (PFV), results from persistence of the embryonic hyaloid vasculature and manifests variably with a combination of anterior and posterior segment abnormalities. PHPV is unilateral in approximately 90% of patients and is inherited sporadically without associated systemic conditions. 1 Clinical manifestations primarily comprise a small eye, shallow anterior chamber, glaucoma, and fundus abnormalities. 1 There are three forms of PHPV: anterior, posterior, and combined (both anterior and posterior). 1 Herein, we report a child who initially presented with strabismus as a symptom and who had bilateral and combined-type PHPV. The reporting of this study conforms to the CARE guidelines. 2
Case report
A 6-year-old boy came to the Department of Ophthalmology of our hospital with a complaint of binocular dyskinesia for the past 6 years. He had been diagnosed with strabismus previously at a local hospital but had not received treatment. The symptoms had worsened over time. The child was born at full-term by vaginal delivery, with no history of requiring supplemental oxygen. There were no systemic abnormalities or family history of eye problems. During the examination, the child’s best-corrected visual acuity in the right eye was 0.7 (−3.00 DS/−0.50 DC × 125). In the left eye, the child’s vision was limited to counting fingers at a distance of 70 cm (−9.00 DS/−3.50 DC × 115). His corneal reflexes were symmetrical, and the prism test showed LH’ = 10 and LH = 15. The synoptophore result showed a lack of stereopsis and fusion function. Slit lamp examination with dilated pupils showed post-capsule opacity in both eyes, with the left eye being more severely affected. The posterior segment examination revealed a fibrous band arising from the optic disc in the left eye and a grayish proliferation in the temporal retina in the right eye (Figure 1). Optometry was performed under cycloplegia, but visual acuity did not improve in the left eye, suggesting the presence of stimulus deprivation amblyopia. Ocular B-mode ultrasonography indicated that the axial length of the right eye was 23.67 mm and that of the left eye was 23.61 mm, suggesting the presence of myopia. More importantly, ultrasonography revealed a strong echogenic band-like structure extending from the posterior surface of the lens to the optic nerve head in the vitreous chamber of the left eye (Figure 1). No abnormality was found in the vitreous chamber of the right eye (Figure 1).
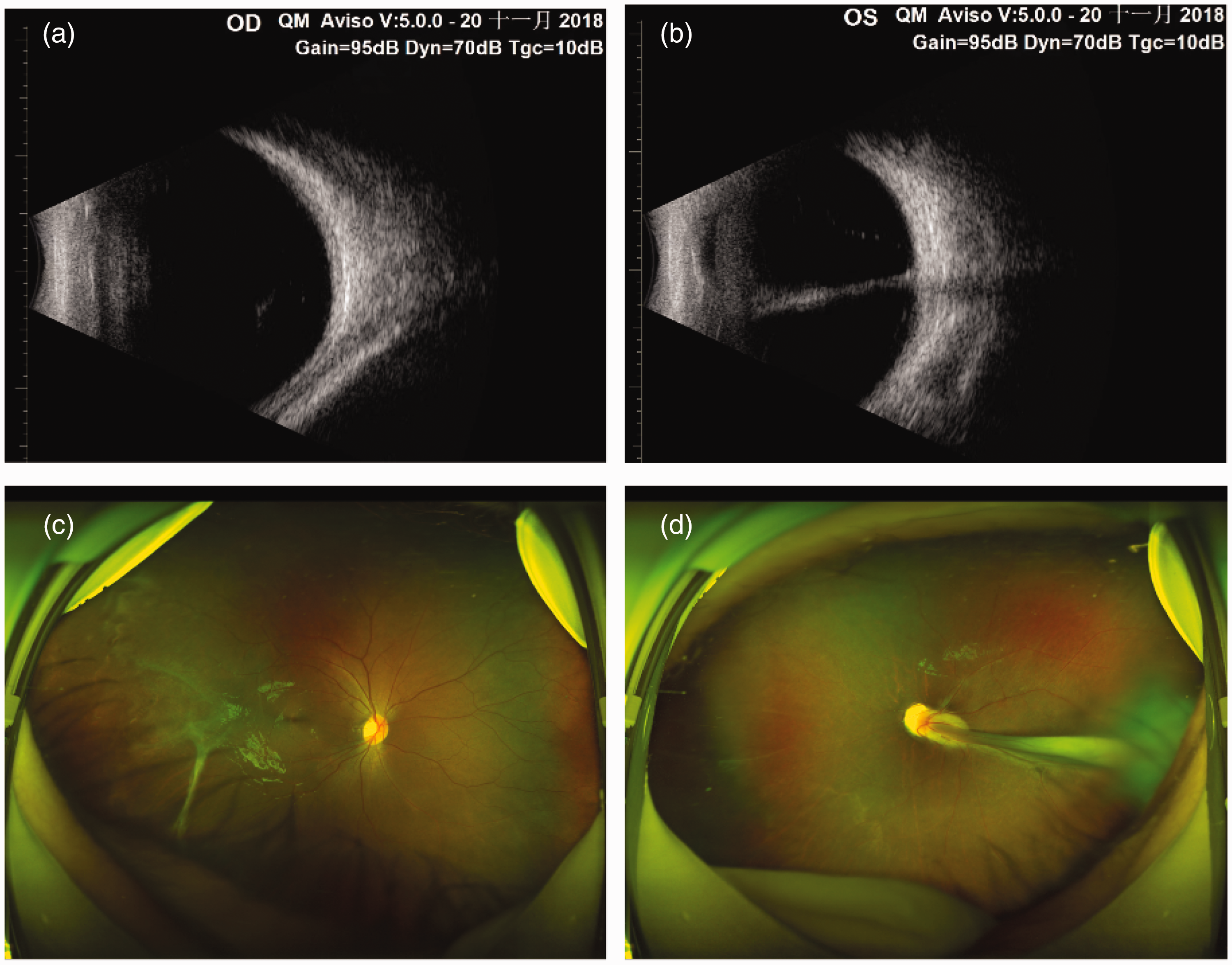
Imaging findings. (a) No abnormalities are visible in the vitreous chamber of the RE. (b) A strong echogenic band-like structure is visible extending from the posterior surface of the lens to the optic nerve head in the vitreous chamber of the LE. (c) A grayish proliferation in the temporal retina is visible in the RE and (d) A fibrous band arising from the optic disc is visible in the LE. RE, right eye; LE, left eye.
On the basis of the above eye examination findings, a diagnosis of bilateral PHPV (combined type) was made. Unfortunately, despite being informed of the guarded visual prognosis, the child’s parents declined to proceed with the recommended surgery.
Discussion
The most frequent manifestation of PHPV is the presence of white pupillary reflex (leukoria) and microphthalmia, without accompanying systemic symptoms. 3 Bilateral presentations are rare and are associated with systemic and syndromic associations, such as trisomy, Norrie’s disease, and Warburg’s syndrome. 4 Systemic abnormalities, including cleft lip, cleft palate, polydactyly, and microcephaly, could potentially be associated with chromosomal abnormalities. Although a relationship between genetic abnormalities and PHPV has not been reported, several cases of PHPV have been observed in the same family, suggesting the presence of an autosomal dominant or recessive factor. 5 In this particular case, apart from the eye symptoms, there were no observable manifestations. The incidence rate of bilateral PHPV is <10%. 6 This disease can be further classified into three types by location: anterior, posterior, and combined. 7 The most frequently observed clinical manifestations are leukocoria, microphthalmos, and cataract. 8 In our patient, the clinical symptoms were bilateral, but the axial length and anterior chamber were normal, there was no microphthalmos or systemic diseases, and none of the symptoms matched those reported in other cases.
Lens opacity often accompanies PHPV. 1 In our patient, B-mode ultrasonography revealed a distinct mushroom-like echo between the posterior part of the crystalline body and the anterior part of the vitreous body. The umbrella part of the mushroom was located behind the lens and in proximity to the posterior capsule. The stalk of the mushroom was connected to the optic papilla through the vitreous cavity. No calcified areas were observed in the interior of the eye. Considering these findings and the findings from the slit-lamp examination, the diagnosis of PHPV was established for this patient.
Intraocular lens implantation is recommended for individuals with PHPV, with the initiation of prompt and intensive amblyopia therapy. 9 However, our patient was assessed medically quite late, by which time amblyopia had already developed in the left eye. The local doctors who examined the child previously diagnosed the condition as strabismus, possibly owing to the child’s young age and inability to cooperate with eye fundus examination. This case stresses that every child presenting with a squint should undergo detailed posterior segment evaluation with pupillary dilatation.
In some regions in our country, especially in the northwest region, economic development is comparatively delayed. Therefore, it is crucial to highlight the importance of early diagnosis and treatment for congenital and hereditary eye conditions. Enhancing the diagnostic capabilities of primary healthcare practitioners is also of great importance. Access to frequent medical lectures about these diseases would be helpful. Additionally, providing primary doctors with photographs and auxiliary examination findings from cases of PHPV can improve physicians’ understanding of the disease. Surgery is the primary treatment for PFV syndrome, with the aim of reconstructing visual pathways, in infants with congenital cataracts. Visual rehabilitation training is very important postoperatively. It is necessary for doctors, patients’ families, and patients to collaborate throughout the diagnostic and therapeutic process.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231222214 - Supplemental material for “Strabismus in children” is not simple – bilateral persistent hyperplasia primary vitreous: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231222214 for “Strabismus in children” is not simple – bilateral persistent hyperplasia primary vitreous: a case report by Yuqiu Zhang in Journal of International Medical Research
Footnotes
Acknowledgements
This study was supported by Lanzhou University No. 2 Hospital.
Author contributions
Yuqiu Zhang designed and performed the research, analyzed the data, and wrote this case report.
Data availability statement
All data generated or analyzed during this study are included in this published case report.
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Ethics statement
Ethics approval is not required for case reports in our institution Verbal and written informed consent was obtained from the child’s parents for publication of this case report. The patient’s details have been de-identified.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.