
Abstract
Objective
Treatment of syncope in older adults places a burden on healthcare systems. We used five risk stratification tools to predict short-term adverse outcomes in older patients with syncope.
Methods
This was a retrospective analysis of patients with syncope (age ≥60 years) in the emergency department of an urban academic hospital. The data were evaluated using the Risk Stratification of Syncope in the Emergency Department (ROSE), San Francisco Syncope Rule (SFSR), FAINT, Canadian Syncope Risk Score (CSRS), and Boston Syncope Criteria (BSC) tools. Sensitivity, specificity, accuracy, positive and negative predictive value (NPV), and positive and negative likelihood ratios of each tool were calculated and compared for adverse events within 1 month.
Results
In total, 221 patients (average age 75.6 years) were analyzed. Fifty-nine patients (26.7%) had experienced an adverse event within 1 month. For the ROSE, SFSR, FAINT, CSRS and BSC tools, sensitivities were 81.3%, 76.3%, 93.2%, 71.2%, and 94.9%, specificities were 88.3%, 87.7%, 56.8%, 71.6%, and 67.3%, and NPVs were 92.9%, 91.0%, 95.8%, 87.2%, and 97.3%, respectively.
Conclusion
The five assessed tools could be useful for physicians in screening older patients with syncope for the risk of short-term adverse events, according to the patient’s actual situation.
Keywords
Introduction
Syncope is a symptom of cerebral hypoperfusion and is defined as a short, sudden, self-limited episode of transient loss of consciousness with a brief period of unresponsiveness and failure to maintain postural tone, ultimately resulting in spontaneous recovery that requires no resuscitation measures. 1 Although the incidence rate of syncope varies among different regions worldwide, it accounts for approximately 1% to 5% of all emergency department (ED) visits and has shown an increasing trend in recent years.2–3 Syncope results in considerable cost to the health care system. Approximately 30% to 40% of patients with syncope are admitted to the hospital for further treatment, and this proportion can reach 50% for patients over 60 years old. Complications and physiological changes after syncope are worse for older patients, which makes clinical evaluation challenging for physicians.4–6
The management of patients with syncope can present a dilemma because its pathophysiological processes and causative factors are complex and varied. Early risk stratification during the initial evaluation is crucial to guide clinical decisions and prevent short-term adverse events.7–8 Several clinical models used in the ED are designed to assist physicians in making decisions at the bedside and performing risk stratification in patients; these include the Risk Stratification of Syncope in the Emergency Department (ROSE) tool, San Francisco Syncope Rule (SFSR), the FAINT tool, Canadian Syncope Risk Score (CSRS), and Boston Syncope Criteria (BSC). Considering that these tools were derived in a few centers and some models are newly developed, external validation is limited and some findings differ among clinical studies.9–16 Therefore, in the present study conducted in a developing country, we aimed to explore the value of the ROSE, SFSR, FAINT, CSRS, and BSC tools in identifying older patients with syncope who are at risk for short-term adverse events.
Methods
Study design and participants
This was a single-center retrospective observational cohort study performed in the ED of our hospital in China. The data were obtained from the files of patients who were observed and diagnosed with syncope (code R55.X04 using the International Classification of Diseases 10th Revision) at their first consultation in the ED between 1 September 2018 and 31 December 2021. There were no fixed decision tools for syncope management. The 1-month clinical outcomes were checked to evaluate the predictive values of the ROSE, SFSR, FAINT, CSRS, and BSC tools in detecting the risk of adverse events.
This retrospective study received an exemption of institutional review board approval. Verbal informed consent was obtained when patients saw a doctor in the hospital. We de-identified all patient details so patients could not be identified in any way. This retrospective study was conducted according to the principles outlined in the Declaration of Helsinki.
Study population and data collection
Patients aged 60 years or older presenting to the ED with syncope were eligible for this study; our previous study showed that this group has a higher proportion of adverse events in the first 1 month after presentation for syncope than those under 60 years of age. The exclusion criteria were as follows: 1) patients aged less than 60 years; 2) those with confirmed non-syncope syndromes (such as seizure, shock, sustained unconsciousness, head injury preceding the loss of consciousness, and stroke); 3) patients who had comorbidities with a low survival rate (such as advanced malignant neoplasm, dyscrasia, circulatory failure, respiratory failure, and hemorrhage requiring blood transfusion); 4) patients with a history of drug or alcohol abuse. Some patients were excluded owing to a new serious diagnosis or lack of sufficient clinical data. Older patients with syncope who had received all clinical examinations and laboratory tests required for the five syncope risk stratification tools were included in the study, even if they were discharged from the ED after seeing a doctor.
The required sample number for the study was estimated to be at least 84, considering the 30% prevalence of short-term serious outcomes and 0.1 desired precision. 17 The final decision regarding enrolled patients was made after patient evaluation forms were completed; the form included 32 variables derived from existing tools for syncope. The attending physicians, including an emergency medicine specialist, a cardiologist, and a neurologist, independently calculated patients’ scores based on the clinical and laboratory data according to the items included in each syncope risk stratification tool.
Clinical and laboratory data were extracted for analysis and stored in a predesigned database. All the authors calculated the scores together according to the ROSE, SFSR, FAINT, CSRS, and BSC tools to reduce personal interpretation bias. The ROSE tool considers patients to be positive and at high risk for adverse events if any of the following are present: B-type natriuretic peptide (BNP) level ≥300 pg/mL or bradycardia ≤50 beats per minute in the ED/pre-hospital period, a rectal examination showing fecal occult blood, anemia with a hemoglobin level ≤90 g/L, chest pain associated with syncope, an abnormal electrocardiogram (ECG) showing Q wave but not in lead III, or pulse oxygen saturation (SpO2) ≤94% on room air. 9 The SFSR deems patients to be positive and high risk with the presence of any of the following: a history of congestive heart failure (CHF), hematocrit level <30%, abnormal ECG, shortness of breath, and systolic blood pressure <90 mmHg. 10 In the FAINT tool, the presence of any history of heart failure, history of cardiac arrhythmia, an initial abnormal ECG result, elevated N-terminal pro-BNP, or elevated high-sensitivity troponin T (TnT) puts the patient in the non-low-risk group for adverse outcomes. The interpretation of abnormal ECG was similar to that in previous research. 11 Here, “FAINT2” stands for a cut-off value of “2” used for evaluation with the FAINT tool, which was set up according to the latest study. 12 The CSRS tool was developed by assigning points to each factor based on the relative magnitude of the coefficient, with a score ranging from −3 to 11; the score includes nine elements in the categories of clinical data, investigations, and presumptive ED diagnosis. A score of 1 or higher is judged as high risk.13–14 In the BSC tool, the presence of any factor, such as acute coronary syndrome, cardiac history, a family history of sudden death, valvular heart disease, signs of cardiac conduction disease, circulating volume depletion, persistent abnormal vital signs in the ED, and brain lesions, places the patient in the high-risk group. 15 A small cohort of 50 cases was assessed as a training group by three physicians to ensure that the scores were accurate, and kappa values were calculated (Supplemental Table 1).
All patients were followed up in a search of our hospital’s electronic medical record system to identify adverse outcomes within 1 month of the first referral to the hospital with complaints of syncope, or by telephone call if the patient had transferred to another hospital after their index presentation at our hospital. The loss to follow-up rate was roughly 5%. Short-term adverse outcomes were defined a priori as one of the following events: mortality, cardiac pulmonary resuscitation, acute myocardial infarction (AMI), cardiac arrest, severe arrhythmia,18–19 pacemaker implantation or implantable cardioverter-defibrillator, cardiac stent insertion, cerebrovascular accident, hemorrhage requiring urgent treatment, or pulmonary embolism. AMI was characterized as a rise in cardiac markers (cardiac troponin) above the 99th percentile of the upper reference limit, ECG changes (significant ST/T changes or left bundle branch block), or development of pathologic Q waves. Serious arrhythmias included ventricular fibrillation, ventricular tachycardia, sick sinus syndrome, sinus pause >3 seconds, Mobitz type II atrioventricular block, complete heart block, symptomatic supraventricular tachycardia, symptomatic bradycardia, atrial fibrillation with rapid ventricular rate, and atrial tachycardia.
Statistical analysis
Statistical analysis was carried out using IBM SPSS version 20 (IBM Corp., Armonk, NY, USA). Descriptive statistical analysis was performed to characterize the study population. Patients were divided into three age groups: 60 to 69, 70 to 79, and ≥80 years of age. Quantitative data are reported as mean ± standard deviation or standard error, and qualitative data are reported as frequency and percentage. Differences among variables were evaluated using the chi-square test and Fisher’s exact test, as appropriate.
To evaluate each clinical decision rule (CDR) in predicting outcomes, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (PLR), and negative likelihood ratio (NLR) were calculated to identify patients who experienced adverse outcomes during the follow-up period. Receiver operating characteristic (ROC) curves were generated, and the area under the ROC curve (AUC) was compared using a previously proposed method to assess the predictive value of each CDR.20–21 Spearman’s rank correlation coefficient (r) was calculated between risk stratification using each CDR and the follow-up presence of any adverse events within 1 month. 22 The significance level was set to p < 0.05.
Results
Characteristics of study participants
A total of 591 older patients who were referred to the ED with complaints of syncope were screened, and 358 patients were excluded owing to a lack of sufficient data or a new serious diagnosis; thus, 233 patients were enrolled. Our study was carried out among 221 patients with follow-up for 1-month clinical outcomes; 12 patients were lost to follow-up (Figure 1).
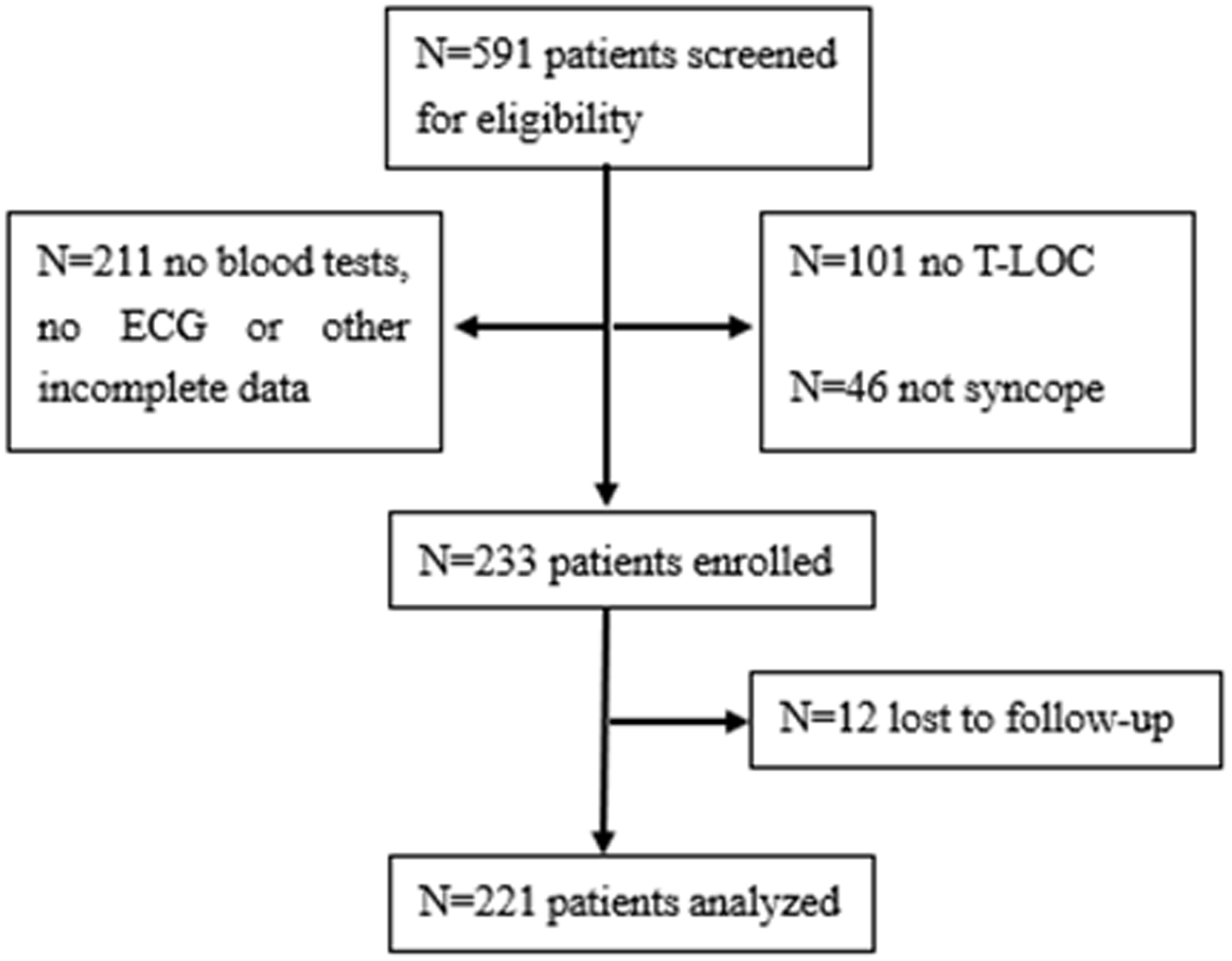
Flow diagram of the study.
The mean age of the study group was 75.6 ± 8.5 years, and the median age was 75 years. Among the cohort, 50.2% were men and 49.8% were women. Compared with men, women were older (78.1 ± 8.5 years vs. 73.2 ± 7.9 years, respectively, p < 0.05). There were significant differences among the three age groups in terms of hemoglobin, hematocrit, CHF, SpO2, aspartate aminotransferase, blood urea nitrogen (BUN), creatinine, and the ratio of BUN/creatinine (Table 1).
Characteristics of older adults with syncope presenting to the emergency department

CHD, coronary heart disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disorder; OMI, old myocardial infarction; CVA, cerebrovascular accident; SpO2, oxygen saturation; BNP, B-type natriuretic peptide; TnT, troponin T; BUN, blood urea nitrogen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; INR, international normalized ratio; SE, standard error.
Among the 221 patients enrolled in our analysis, the cause was classified as neurally mediated syncope (NMS), cardiac syncope (CS), orthostatic hypotension, and syncope with unknown cause. By 1 month after the index ED visit, 59 patients (26.7%) had experienced a primary serious outcome; the sex and frequency data are outlined in Figure 2 and Supplemental Table 2. There was a significant difference in the incidence of adverse events between the NMS and CS groups (p = 0.014). For the NMS group, there was a significant sex-specific difference in the incidence of adverse events (p = 0.008).

Patient outcomes among the four categories of syncope.
Factors associated with incidence of all adverse outcomes
There were significant differences in the incidence of adverse events in patients with or without a history of hypertension, coronary heart disease (CHD), CHF, and chronic obstructive pulmonary disorder (COPD), as well as the levels of SpO2 and BNP. For levels of creatinine and international normalized ratio (INR), there were non-significant differences in the incidence of adverse events (Table 2, Supplemental Table 3).
Factors associated with adverse events.

CHD, coronary heart disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disorder; SpO2, oxygen saturation; BNP, B-type natriuretic peptide; INR, international normalized ratio.
Incidence of adverse outcome evaluated using different CDRs
All important elements of the ROSE, SFSR, FAINT, CSRS, and BSC tools were evaluated separately for their ability to predict predefined serious events; the number of high-risk patients identified using the different CDRs was 67, 65, 125, 88, and 109 respectively. The sensitivity, specificity, accuracy, PPV, NPV, PLR, NLR, and AUC of the predefined syncope risk scores to predict adverse events were also calculated (Table 3, Figure 3, Supplemental Table 4).
Comparative analysis of risk stratification tools.
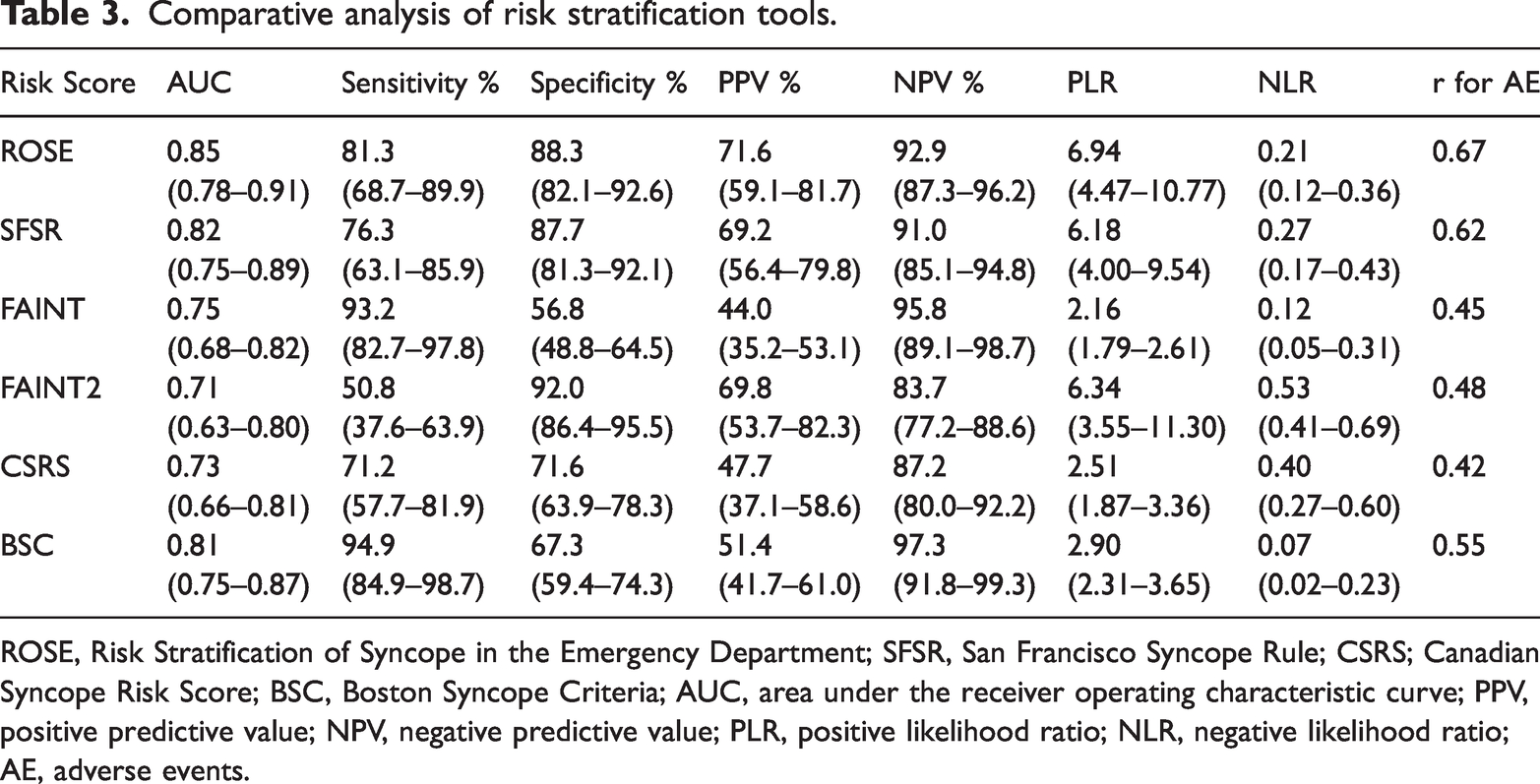
ROSE, Risk Stratification of Syncope in the Emergency Department; SFSR, San Francisco Syncope Rule; CSRS; Canadian Syncope Risk Score; BSC, Boston Syncope Criteria; AUC, area under the receiver operating characteristic curve; PPV, positive predictive value; NPV, negative predictive value; PLR, positive likelihood ratio; NLR, negative likelihood ratio; AE, adverse events.

Receiver operating characteristic curves for risk stratification tools.
Correlation analyses between assessment with different CDRs and adverse events in 1 month
Spearman’s rank correlation coefficient (r) in the analyses regarding application of the ROSE, SFSR, FAINT, FAINT2, CSRS, and BSC tools for adverse events during follow-up was 0.67, 0.62, 0.45, 0.48, 0.42, and 0.55, respectively.
Discussion
To the best of our knowledge, this is the first reported cohort study on the application of five key CDRs for older patients with syncope in a developing country. Because the number of patients with syncope-related adverse outcomes increases sharply after age 60 years20–21 and older patients often have multiple comorbid conditions, it is crucial to distinguish at-risk patients to administer timely and precise therapies. We conducted this study to compare clinical application of five CDRs for risk assessment in older adults with syncope. A total of 221 enrolled patients were followed up for 1 month and the occurrence of adverse outcomes was compared against the ROSE, SFSR, FAINT, CSRS, and BSC CDRs.
Overall, 26.7% of our study cohort had an adverse outcome within 1 month of presentation at our ER for syncope. In our study, the incidence of adverse events was affected by comorbidities of hypertension, CHD, CHF, and COPD, as well as levels of SpO2 and BNP. This suggests that older patients with syncope and hypertension, CHD, CHF, or COPD will be more likely to have an adverse event within the first month. Comorbid COPD has not been mentioned in relation to other syncope assessment tools until now. Our study findings also suggested that creatinine and INR levels potentially influence short-term adverse events. SpO2 or respiratory status is a variable in the ROSE, SFSR, and BSC tools; CHF is a variable in the SFSR, FAINT, and BSC tools; CHD is a variable in the CSRS and BSC tools; and BNP is a variable in the ROSE and FAINT tools. Additionally, the SFSR, CSRS, and BSC tools all emphasize the measurement of blood pressure. 23 However, creatinine and INR have not been included in any CDRs until now; however, liquid metabolism in the body and coagulation status may affect the body’s circulatory perfusion before syncope.
For the four diagnostic categories for syncope, the number of patients and adverse events were greater in cardiac patients with syncope than those in other patients, which is in accordance with previous studies among patients with advanced age. 24 Patients with NMS showed a sex-specific difference in the incidence of adverse events, but patients with CS displayed no similar results. Compared with CS, NMS is a type of benign syncope, and neural regulation differs according to sex and age. In contrast, CS is a serious symptom with high mortality; therefore, the type of syncope itself has specific characteristics and clinical prognosis.25–27 In our research, more than half of adverse events within 1 month were related to AMI and arrhythmia. Cardiac syncope is associated with higher mortality, irrespective of age and sex. The five CDRs in our investigation all include cardiac elements in their assessment, highlighting the importance of cardiogenic parameters and of cardiac syncope in older populations.
The ROSE and SFSR tools showed higher specificities and NPVs and the AUCs were greater than 0.8, meaning that these tools may be important in identifying and screening non-high-risk patients with syncope; this is roughly consistent with previous clinical studies of each CDR.9–10 Additionally, the correlation coefficients of these two CDRs with short-term adverse events were greater than 0.60, which suggests reliable correlation. AUCs of the FAINT, FAINT2, CSRS, and BSC tools were all greater than 0.7. The FAINT and BSC tools had higher sensitivities and NPVs than the other tools whereas the CSRS tool had moderate results in our clinical application. Therefore, the FAINT and BSC tools may have advantages in identifying high-risk patients with syncope. The BSC tool includes the most comprehensive elements for syncope assessment until now, indicating high risk if any one item is positive. The correlation coefficient of the BSC tool was close to 0.6, which suggests substantial correlation. The CSRS tool assigns various points to each factor based on the relative magnitude of the coefficient. External validation of this tool was completed in 2020 in an Australian cohort of 283 patients; 28 therefore, larger and broader investigation of clinical applications are needed in the future. The correlation coefficient of the CSRS tool was greater than 0.40, which suggests moderate correlation.
The FAINT tool was established up for older patients in 2020. Preliminary results of recent multicenter external validation in Europe and the United States suggest that this tool is safe for evaluating older patients with scores of 0 or 1. 12 The cut-off value of “1” was used in the original study for patient evaluation, which means that 24 patients would be “misjudged” as positive in our study with a cut-off score of 1, which may lead a greater proportion of low-risk patients to seek further clinical examinations. Therefore, we additionally set “2” as another cut-off score for evaluation using the FAINT tool (FAINT2) for comparison with other CDRs in older patients. The FAINT results indicated that the sensitivity and NPV were higher and the specificity was lower, which was consistent with the original studies by Probst. 11 However, results of the FAINT2 tool indicated that the specificity and PLR were higher and the sensitivity was lower. Both AUCs were greater than 0.7, and the correlation coefficients of the FAINT and FAINT2 tools were both greater than 0.4, indicating moderate correlation. The original research on the FAINT tool improved the evaluation sensitivity at the expense of specificity. Considering that the proportion of cardiac syncope is greater among older patients, its complications are more dangerous in this population when it occurs. The higher sensitivity of the FAINT tool may avoid the possibility of missing the risk of adverse events, at best, but more relevant medical resources are required. Therefore, the FAINT tool may be much more valuable for older people with any history of cardiovascular disease under the condition of sufficient medical resources. Probst explained that the main point of the FAINT tool is that it does not omit serious adverse cardiac events, so establishing its high sensitivity and low NLR were the original intentions of that study. However, this tool is unsuitable for screening low-risk patients at present because international multicenter validation has not been completed. The FAINT tool has been evaluated in a clinical study of older patients with syncope with the largest sample size until now, but the population included patients aged 60 years and above with syncope or near syncope (the sensation of impending loss of consciousness without actually losing consciousness), and the patient refusal rate was as high as 53.2% when the study was implemented. The FAINT tool includes two biochemical elements related to cardiac function and myocardial damage. Compared with the ROSE tool (which includes only BNP levels) and the SFSR tool (without biochemical elements), the FAINT tool certainly improves laboratory testing and medical costs, and it may be helpful in reducing the diagnosis rate of “unexplained syncope” in the clinic. Therefore, analysis of the net effect of the FAINT tool in health economics is worth further exploration. The FAINT tool is also much simpler to use in assessment than the CSRS and BSC tools. The five tools evaluated in our study all facilitate assessment for older patients with syncope in practice. To date, however, no syncope risk stratification tool is available that can be used independently of physician judgment; these tools only play a role in decreasing the cognitive load for physicians when making clinical decisions.
Overall, the proportion of 1-month adverse events in our study was 26.7%. This was higher than the rate reported in the original studies evaluating the ROSE, SFSR, FAINT, CSRS and BSC tools but similar to other reports from developing nations.17,29,30 The discrepancy in the proportion of short-term adverse events may be related to the different levels of public health services and disease prevention abilities in the cohort population. Additionally, this may be related to the characteristics of enrolled patients: the median age of patients in this study was 75 years, and 64.3% were over 70 years old, with an incidence of adverse events higher than that of patients aged 60 to 69 years (33.8% vs. 13.9%). The incidence of syncope in the older population generally increases with age. However, the body is generally in a greater state of decline with increasing age, so the physiological stress response after syncope may be partly affected and complications could be more complex, leading to much greater risks of adverse events.6,31–34
The limitations of this study include that it was conducted at a single center with limited resources in China; thus, our patient group cannot represent the entire population in developing countries. Second, data regarding the onset symptoms of patients with syncope before they arrived at the hospital were not available in our study. Third, this study only focused on patients aged 60 years or older presenting to the ED. Fourth, a proportion of ED patients lacked sufficient clinical laboratory data required for assessment using the risk stratification tools, which may affect external validity.
Conclusions
Our study aimed to clarify the advantages and disadvantages of five risk stratification tools in identifying patients with syncope at risk of short-term adverse events. Flexible application of the ROSE, SFSR, FAINT, CSRS, and BSC tools may improve the efficiency of clinical evaluations to help physicians more scientifically judge the risk of short-term adverse outcomes according to the actual clinical situation of older patients with syncope.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231220894 - Supplemental material for Application of five risk stratification tools for syncope in older adults
Supplemental material, sj-pdf-1-imr-10.1177_03000605231220894 for Application of five risk stratification tools for syncope in older adults by Hong Mu, Jiexin Liu, Cheng Huang, Hefei Tang, Sisi Li, Chang Dong, Tiecheng Yang, Limin Liu and Bin Xu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231220894 - Supplemental material for Application of five risk stratification tools for syncope in older adults
Supplemental material, sj-pdf-2-imr-10.1177_03000605231220894 for Application of five risk stratification tools for syncope in older adults by Hong Mu, Jiexin Liu, Cheng Huang, Hefei Tang, Sisi Li, Chang Dong, Tiecheng Yang, Limin Liu and Bin Xu in Journal of International Medical Research
Footnotes
Authors’ contributions
HM participated in the study design, analyzed and interpreted the data, and drafted the manuscript. JXL, TCY, LML, and BX participated in the study design, performed critical revision of the manuscript for important intellectual content, contributed statistical expertise, obtained funding, helped with technical and material support, and supervised the study. CH, HFT, SSL, and CD participated in acquisition of the data and technical support. All authors read and approved the final manuscript.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No. 82000323). Open Access funding was provided by Beijing Tiantan Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.