
Abstract
Cardiovascular syphilis manifests many years after primary infection. Here, we report the successful treatment of a patient who developed syphilitic aortitis with bilateral coronary ostial stenosis and aortic insufficiency. The patient underwent right coronary artery bypass grafting, left main coronary ostial “open” stent placement, and mechanical aortic valve placement during open-heart surgery.
Keywords
Introduction
Syphilis is a chronic infectious disease that has been recognized by both clinicians and the public for centuries. 1 Cardiovascular complications of syphilis, which typically manifest 10 to 20 years after primary infection, include aortitis, aortic insufficiency, coronary stenosis, and aortic aneurysm. 2 Syphilitic ostial coronary stenosis as a disease entity was reported in the literature as early as 1929. 3 It was the third most common presentation of cardiovascular syphilis, accounting for 26% of cases, in Heggtveit’s historical autopsy series in 1964. 4 In Bruenn’s classic treatise on syphilitic coronary lesions, ostial coronary stenosis commonly involved both orifices. 5 Furthermore, coronary syphilis was strongly associated with aortic regurgitation and likely reflected the severity of the contiguous inflammatory process. 5 Here, we report a surgical case of bilateral coronary ostial lesions and aortic regurgitation due to cardiovascular syphilis.
Case report
The reporting of this study conforms to the CARE guidelines. 6 A 57-year-old woman presented to our medical center complaining of exertional chest tightness, chest pain, and difficulty breathing for 20 days. Her medical history did not include hypertension, coronary artery disease, or diabetes mellitus. She denied prior tobacco or alcohol use. Serologic assays at admission showed that the detection value of Treponema pallidum antibody (TP-Ab) was 197.9 as a cutoff index (COI), and the Treponema pallidum particle agglutination test result (TPPA) was positive. Subsequent transthoracic echocardiography (TTE) revealed aortic valve thickening and severe eccentric regurgitation; valve leaflet stiffness; ascending aortic sinus measurement: 30 mm; left ventricular end-diastolic diameter: 55 mm; and ejection fraction (EF): 61% (Figure 1). Coronary angiography highly suggested stenosis at the opening of the left coronary artery (Supplementary Video 1). Curiously, an angiography catheter and a guidewire were both used during coronary angiography; however, the right coronary artery could not be located successfully (Supplementary Video 2). Coronary computed tomography angiography (CCTA) was then performed, and the results suggested mild occlusion at the origin of the right coronary artery and moderate (approximately 66%) stenosis at the origin of the left coronary artery (Figure 2). On the basis of these findings, cardiovascular syphilis was highly suspected considering the positive serological test result for syphilis and the absence of clinical symptoms frequently found with other types of aortitis, such as Takayasu aortitis, giant cell arteritis, and Behcet’s disease.

Preoperative echocardiography of the patient. (a) The ascending aortic sinus measures approximately 30 mm. (b) The peak flow velocity across the aortic valve was approximately 2.8 m/s, and the mean pressure gradient was 17 mmHg. (c) The left ventricular end-diastolic diameter was approximately 55 mm. (d) The aortic valve exhibited severe eccentric regurgitation. (e) The inner diameter of the ascending aorta measured approximately 39 mm and (f) The left ventricular ejection fraction was 61%.

(a) Preoperative computed tomography angiography image showing moderate (approximately 66%) stenosis at the origin of the left coronary artery (red arrow). and(b, c) Preoperative computed tomography angiography image showing mild occlusion at the origin of the right coronary artery (red arrow in each panel).
Cardiac surgery was performed after 3 weeks of penicillin therapy (2.4 million units by intramuscular injection once weekly). Intraoperative transesophageal echocardiography (TEE) of the aortic cusps showed obvious thickening and contracture. The ascending aorta was mildly thickened, without obvious dilatation (Figure 3). Therefore, we did not address the ascending aortic vessels. Cardiac arrest was successfully induced by retrograde cardioplegic solution. After the aorta was opened, the origin of the left coronary artery was severely narrowed under direct vision, with a diameter of approximately 1 mm, while the origin of the right coronary artery was not obvious under careful direct vision. After consulting cardiovascular physicians, we chose an innovative approach named “open” stent placement. During the procedure, a 0.014’ (0.36-mm) guidewire was used to place a 4.0/13-mm stent in the left main coronary artery during open-heart surgery (Figure 3). Coronary artery bypass grafting (CABG) was performed to graft the right coronary artery with a left saphenous vein graft (SVG). Proximal anastomosis of the SVG was performed under direct vision at the proximal ascending aorta as the wall of the proximal ascending aorta was not thickened. The aortic valve was replaced with a 23-mm Regent® mechanical valve (St Jude Medical, Inc., St Paul, MN, USA). Histopathological analysis of the excised aortic valves showed dense fibrous connective tissue accompanied by mucoid degeneration, collagenization, and visible neutrophil infiltration (Figure 4). The postoperative recovery was smooth and without obvious complications. CCTA before discharge revealed good coronary hemodynamics (Figure 5). During the 2-year follow-up after discharge, the patient experienced no cardiac symptoms.
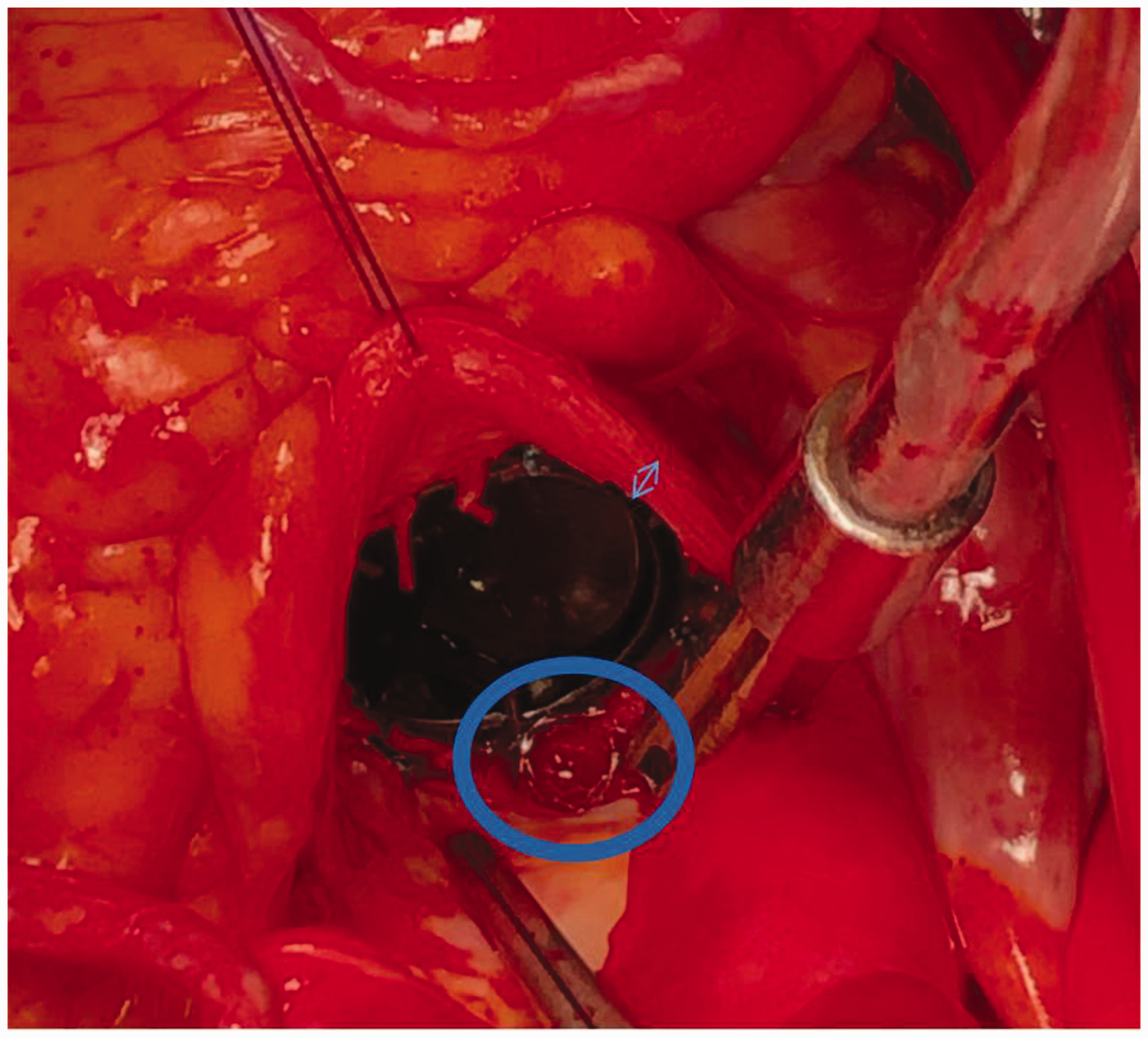
Intraoperatively, the ascending aortic wall was slightly thickened (blue arrow), and a stent was successfully implanted in the left coronary artery (blue circle).

High-power histomicrographs of the aortic valve specimen. The left panel shows dense fibrous connective tissue accompanied by mucoid degeneration and collagenization. The right panel shows visible neutrophil infiltration (hematoxylin and eosin, ×100, both panels).

Postoperative CTA showing that the stent at the opening of the left coronary artery is unobstructed (a, c; red arrows), and blood flow between the right coronary artery and ascending aorta has been bypassed (b, c; red arrows). CTA, computed tomography angiography.
Discussion
The cardiovascular manifestations of syphilis are asymptomatic aortitis, aortic insufficiency, coronary ostial stenosis, aortic aneurysm, and gummatous myocarditis. 2 Cardiovascular syphilis is associated with the tertiary stage of syphilis infection and usually occurs 10 to 20 years after the initial infection.2,7 Coronary ostial stenosis is reported in 20% to 26% of patients with syphilis. 2 Although cardiovascular syphilis can cause symptoms of angina, myocardial infarction is rare as there is generally ample time for collateral vessel formation. 2 Our patient reported exertional angina preceding her presentation to hospital. Unfortunately, coronary angiography could not determine whether there was rich collateral circulation, owing to the operator’s technique; therefore, we performed CCTA. Coronary ostial lesions with aortic regurgitation have been reported in 14% of patients with syphilitic aortitis. 4 An autopsy of 90 patients with syphilitic aortitis revealed that 15% had significant right coronary ostial stenosis, while 2% had left coronary ostial stenosis. 8 Bilateral coronary ostial stenosis with aortic regurgitation is seen rarely, clinically. 9
Syphilis was once essentially extinct in China, but the incidence has recently increased gradually. For most cardiologists, this disease is relatively unfamiliar; however, the index of suspicion should be high in patients with isolated ostial coronary stenosis. Syphilitic cardiovascular disease indicates late syphilis, and clinical symptoms and signs generally appear 10 to 30 years after infection, lack specificity, and are difficult to diagnose. 10 Especially in elderly patients with risk factors for cardiovascular disease, it is difficult to distinguish cardiovascular syphilitic lesions from those caused by atherosclerosis. 10 We carefully inquired about the patient’s medical history, and confirmed that she did not previously have the typical characteristics of syphilis stage 1 and stage 2. Currently, there is still no gold standard for the diagnosis of syphilitic cardiovascular disease. According to relevant guidelines, 10 the diagnosis of syphilitic cardiovascular disease requires an epidemiological history, typical clinical manifestations, and positive serological test results. Clinically, patients with syphilis tend to be diagnosed with syphilitic cardiovascular disease if they have only coronary artery stenosis. However, if the patient also has stenotic lesions below the coronary ostia, the possibility of coronary atherosclerotic heart disease is considered greater. 11 The patient in this case lacked the typical risk factors for coronary heart disease. On the basis of the medical history, laboratory test results, and echocardiography, CCTA, and coronary angiography findings, the final diagnosis was syphilitic cardiovascular disease. Intramuscular benzathine penicillin G once per week for 3 weeks is the standard regimen for cardiovascular syphilis.12,13
Unlike atherosclerotic coronary artery disease, there is no consensus on the treatment of syphilitic ostial stenosis owing to the limited number of cases reported in the literature. Myriad surgical techniques to address these lesions have been reported, including bypass grafting, percutaneous coronary intervention, endarterectomy or ostioplasty, and patch augmentation.12,14–17 Prior studies have reported lower restenosis rates among patients treated surgically for cardiovascular syphilis compared with percutaneous coronary intervention (PCI). 18 Furthermore, the left internal mammary artery was reported to be the conduit of choice for surgical treatment and superior to an SVG. 18 Surgical treatment of left main coronary artery stenosis caused by syphilis is mainly reported as bypassing the left anterior descending artery and the left internal mammary artery, while there are few reports describing CABG involving the left circumflex artery.18,19 A series of studies have shown that when syphilitic aortitis involves left main coronary artery lesions, the long-term effect of PCI on ostial and middle segment lesions of the left main coronary artery is equivalent to that of CABG.18,20,21 Therefore, we innovatively implanted a stent at the opening of the left coronary artery under direct vision surgery in this case. We consider that implanting the stent under direct vision reduces the procedure time considerably compared with CABG, and this in itself was interesting because cardiac surgeons may implant coronary stents. To our knowledge, no studies have reported such a unique approach. Our approach adds an option to the armamentarium of open-heart surgery for isolated ostial stenosis of the left (or right) coronary trunks if difficult CABG is expected.
This study involved individualized treatment for a case of syphilitic aortic insufficiency combined with lesions of the left and right coronary artery ostia. We successfully implanted a stent in the opening of the left coronary artery during direct vision “open” surgery. CABG was performed for the right coronary artery, with mechanical aortic valve replacement. The recovery was satisfactory during 2 years of follow-up; however, long-term follow-up is required. It is worth noting that the limitation of this case was the lack of pathological examination of the ascending aortic lesion. For similar patients, when addressing aortic valve or coronary artery disease, tissues from multiple locations should be collected for pathological examination, which will help in the final diagnosis and treatment of the disease.
Conclusion
There are many manifestations of cardiovascular syphilis. Isolated ostial coronary stenosis should alert clinicians to the possibility of cardiovascular syphilis. Our case involved individualized treatment for this patient with syphilitic aortic valve regurgitation combined with lesions of the left and right coronary artery ostia. “Open” stent placement adds an option to the armamentarium of open-heart surgery for isolated ostial stenosis of the left (or right) coronary trunks. Long-term and regular follow-up is valuable for the treatment of such diseases.
Teaching points
Cardiovascular syphilis involves the ascending aorta, resulting in aortic aneurysm, aortic regurgitation, and coronary ostial stenosis. Unlike atherosclerosis, coronary ostial stenosis is caused by aortic wall thickening, and coronary lesions distal to the ostia occur rarely. The surgical strategy should be individualized. The “open” stent placement approach adds an option to the armamentarium of open-heart surgery for isolated ostial stenosis of the left (or right) coronary trunks. Long-term follow-up is mandatory after surgery to monitor for aortic dilatation involving the sinuses of Valsalva, prosthetic valve dehiscence, or graft failure/stent restenosis caused by persistent infection of the aortic wall.
Supplemental Material
sj-mp4-1-imr-10.1177_03000605231204496 - Supplemental material for Treatment of syphilitic aortitis with coronary artery bypass grafting and “open” stent placement
Supplemental material, sj-mp4-1-imr-10.1177_03000605231204496 for Treatment of syphilitic aortitis with coronary artery bypass grafting and “open” stent placement by Tiansheng Tang, Changjuan Wu, Ziao Wang, Jun Wei, Dafa Zhang and Weiyong Sheng in Journal of International Medical Research
Supplemental Material
sj-mp4-2-imr-10.1177_03000605231204496 - Supplemental material for Treatment of syphilitic aortitis with coronary artery bypass grafting and “open” stent placement
Supplemental material, sj-mp4-2-imr-10.1177_03000605231204496 for Treatment of syphilitic aortitis with coronary artery bypass grafting and “open” stent placement by Tiansheng Tang, Changjuan Wu, Ziao Wang, Jun Wei, Dafa Zhang and Weiyong Sheng in Journal of International Medical Research
Footnotes
Acknowledgement
The authors are grateful to the patient for providing consent to publish the details of her case.
Author contributions
Drafting the manuscript: TT. Designing the study: DZ. Revising the manuscript: ZW and WS. Collecting and/or analyzing the data: CW and JW. All authors read and approved the final manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
This study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College (Yijishan Hospital) (approval number: YR20230135). The patient provided written informed consent to participate in this study. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
This work was supported by three new projects of the First Affiliated Hospital of Wannan Medical College (Yijishan Hospital) [grant number Y21020] and the Young and Middle-aged Scientific Research Fund Project of Wannan Medical College [grant number WK201042F].
Supplementary material
Supplementary Video 1 Coronary angiography highly suggested stenosis at the opening of the left coronary artery
Supplementary Video 2 Coronary angiography showing that the right coronary artery could not be located successfully using an angiography catheter and guidewire
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.