
Abstract
Myxedema coma is a rare and life-threatening endocrine emergency characterized by abnormalities in multiple organ systems. A 32-year-old woman with prolonged undiagnosed severe hypothyroidism was referred to our hospital owing to lower abdominal pain and menopause for more than 3 months. She underwent exploratory laparotomy and induced abortion under general anesthesia, and developed severe hypoxemia after extubation. She was diagnosed with myxedema coma, and was subsequently discharged with a good prognosis following treatment. This case suggests that myxedema coma should be considered a potential etiology of peri-operative hypoxemia. The findings in this case emphasize the importance of anesthesiologists’ comprehensive understanding of myxedema coma. Prompt diagnosis followed by treatment is essential to reduce the mortality rate associated with this condition.
Keywords
Introduction
Myxedema coma (MC) is a rare and life-threatening endocrine emergency resulting from severe depletion of thyroid hormones. As thyroid hormones are essential for the metabolism of cells and organs in the human body, MC is characterized by multiple organ system abnormalities. 1 MC typically presents with non-specific clinical manifestations and signs, including neurological symptoms, such as stupor or coma, hypothermia, hypoxemia, bradycardia, hyponatremia, and renal impairment. 2 In addition to the numerous etiologies of hypoxemia following extubation, it is imperative to consider MC as a potential peri-operative cause.
Herein, we report a young woman who suddenly presented with severe hypoxemia after extubation in the post-anesthesia care unit (PACU) as a result of MC, during which negative pressure pulmonary edema (NPPE) developed due to airway obstruction.
Case report
A 32-year-old woman with an unremarkable medical history was referred to our hospital owing to lower abdominal pain and menopause for over 3 months. She had experienced general weakness and gastrointestinal discomfort for several years. During this period, she visited a local hospital several times; however, thyroid function testing was not performed to confirm hypothyroidism.
Physical examination on admission showed that the patient’s facial skin was pale, and she had dry skin and edema of both ankles. Her vital signs were within normal limits. Electrocardiography revealed full-lead low-voltage activity, with mild T-wave changes. Chest computed tomography showed multiple microscopic nodules in both lungs and a small amount of pericardial effusion. Abdominal enhanced computed tomography indicated a pelvic mass and pelvic effusion. Echocardiography revealed mild tricuspid regurgitation and a small amount of pericardial effusion (3 mm each in the anterior and posterior pericardium). Laboratory data were as follows: hemoglobin, 83 g/L (reference range, 115–150 g/L); sodium, 140.5 mmol/L (reference range, 137–147 mmol/L); potassium, 2.92 mmol/L (reference range, 3.5–5.3 mmol/L); glucose, 3.53 mmol/L (reference range, 3.9–6.1 mmol/L); and albumin, 40.8 g/L (reference range, 40.0–55.0 g/L). Thyroid function tests were not performed to detect hypothyroidism in this patient.
On arrival in the operating room, the patient was monitored using electrocardiography, pulse oximetry, and non-invasive blood pressure measurement. Anesthesia was induced with sufentanil 35 μg, propofol 100 mg, esketamine 15 mg, and cisatracurium 16 mg. During tracheal intubation, slight edema was observed in the pharynx and vocal cords; however, this did not impede the placement of the tracheal tube. The patient received ventilation using the pressure-controlled ventilation-volume guaranteed mode. Anesthesia was maintained with propofol, remifentanil, and sevoflurane. Surgery was uneventful, and the duration was 2 hours. A total volume of 1500 mL of intra-operative fluids comprising 1000 mL of crystalloid fluids and 500 mL of colloids was administered. Intra-operative body temperature was maintained between 36.1°C and 36.5°C. Blood gas analysis indicated hypokalemia (Table 1), and 1 g of intravenous potassium supplementation was administered. An ultrasound-guided bilateral transversus abdominis plane block was administered with 40 mL of 0.375% ropivacaine after surgery, and the patient was transferred to the PACU.
Arterial blood gas analyses at different time points during surgery.
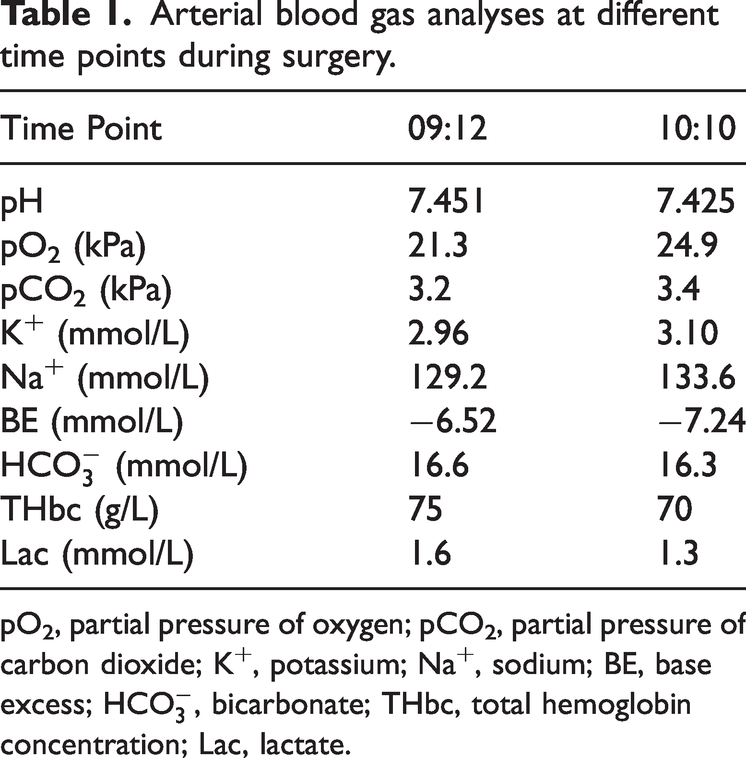
pO2, partial pressure of oxygen; pCO2, partial pressure of carbon dioxide; K+, potassium; Na+, sodium; BE, base excess;
In the PACU, the patient gradually recovered body movements. Considering the patient’s age and acceptable respiratory recovery, the anesthesiologist removed the endotracheal tube. However, the patient developed agitation, increased muscle tone, paroxysmal convulsions, and a progressive decrease in blood oxygen saturation after extubation. The anesthesiologist immediately initiated mask-assisted ventilation followed by repeat doses of fentanyl 0.05 mg and haloperidol 2.5 mg, as well as propofol 50 mg. The seizures resolved following the administration of propofol, but the agitation and unconsciousness resumed upon expiration of the drug’s effects. Owing to persistent hypoxemia, the patient was re-intubated. However, peri-laryngeal edema resulted in difficulties during tracheal intubation, although intubation was ultimately successful. Blood gas analysis after intubation (Table 2) indicated hypokalemia and markedly low hemoglobin concentration. An urgent transfusion of 2 units of suspended red blood cells and 1 g of intravenous potassium were administered. Norepinephrine was administered intravenously with an injection pump to maintain circulatory stability in response to the patient’s persistent hemodynamic instability. Despite receiving high-level ventilator support with pure oxygen, the patient’s oxygenation continued to deteriorate. Cardiac and abdominal color Doppler ultrasonography revealed a small amount of pericardial effusion, and pelvic effusion measuring 43 × 26 mm. Chest radiographs indicated pulmonary edema and gastric distention. The anesthesiologist assessed the risk of aspiration and inserted a nasogastric tube for decompression prior to transferring the patient to the intensive care unit (ICU).
Arterial blood gas analyses at different time points in the PACU.

PACU, post-anesthesia care unit; pO2, partial pressure of oxygen; pCO2, partial pressure of carbon dioxide; K+, potassium; Na+, sodium; BE, base excess;
That night, the patient’s hemodynamics and oxygenation continued to deteriorate, with chest radiography revealing evidence of pulmonary edema and pneumonia. After discussion with the multidisciplinary team, fluid resuscitation therapy was initiated, with infusions of red blood cells and fresh-frozen plasma, high-dose norepinephrine, and methylprednisolone succinate. The next day, the thyroid function test results were as follows: thyroid-stimulating hormone (TSH) >100 mIU/L; total triiodothyronine <0.308 nmol/L; total thyroxine (T4) <11.712 nmol/L; free triiodothyronine <1.648 nmol/L; and free T4 <5.148 pmol/L. The diagnosis of MC was established by two endocrinologists. The plasma cortisol concentration of 519.08 nmol/L effectively ruled out adrenal insufficiency. Therefore, levothyroxine sodium tablets were administered via a nasogastric tube, and methylprednisolone succinate was administered. After receiving systemic treatment, the patient’s thyroid function and lung condition improved dramatically (Figure 1). After 10 days, she was successfully extubated and subsequently transferred from the ICU to the general ward. On the basis of the thyroid function test results, the endocrinologists diagnosed primary thyroid insufficiency as the underlying cause of the MC. Thyroid autoimmune antibody testing revealed markedly elevated levels of anti-thyroglobulin antibodies and anti-thyroid peroxidase antibodies beyond normal ranges, suggesting that primary thyroid insufficiency was caused by autoimmune injury. A daily regimen of 75 μg levothyroxine sodium tablets was maintained following discharge. At the 2-month post-discharge follow-up, the patient reported no persistent symptoms or complications, and her thyroid function had returned to normal levels.
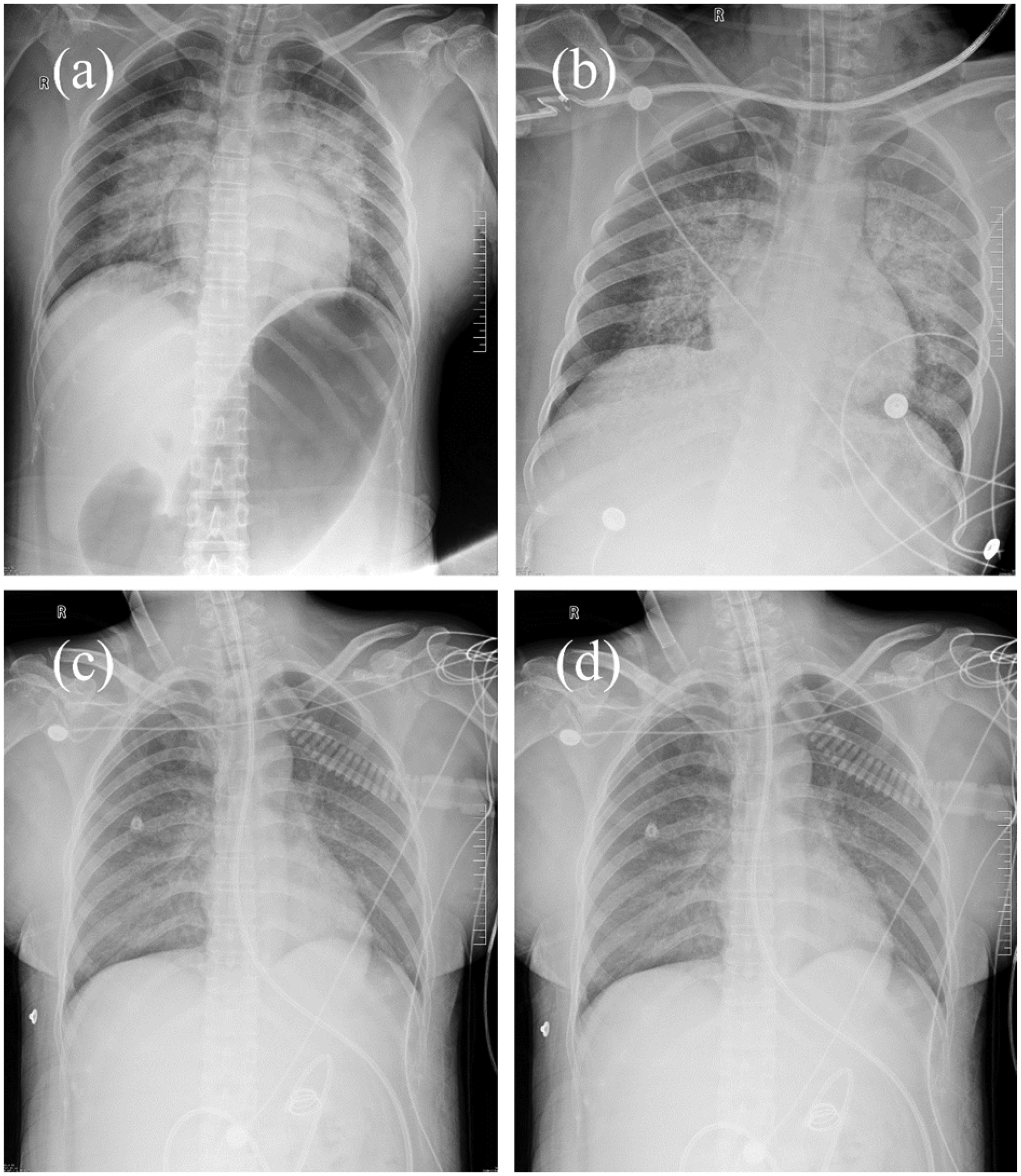
Chest radiography at different time points: (a) In the PACU, (b) day after surgery, (c) 4 days after surgery, and (d) 7 days after surgery.
Discussion
MC typically develops in older women with pre-existing hypothyroidism and is precipitated by surgery, cold exposure, infection, and sedative medications. 3 , 4 The diagnosis of MC remains a challenge because of non-specific clinical manifestations, especially peri-operatively, which is associated with delayed treatment and increased mortality. Early diagnosis and treatment can reduce the mortality rates from the previously-reported range of 60% to 70% to approximately 20% to 25%. 5
A persistent challenge is the absence of definitive diagnostic criteria for MC. Clinicians commonly diagnose MC on the basis of clinical symptoms and signs in conjunction with laboratory tests; universally-accepted diagnostic criteria have not been established. The Japanese Thyroid Association proposed the following diagnostic criteria for MC: hypothyroidism, disturbance of consciousness, hypothermia, circulatory failure, hypopnea, and hyponatremia. 6 A diagnostic scoring system has been developed for MC that comprises six criteria, namely, metabolic disturbances; abnormalities in thermoregulation and the circulatory and central nervous systems; digestive system dysfunction; and precipitating events. 7 Another objective diagnostic tool has been developed for MC that comprises the Glasgow coma scale score, TSH levels, temperature, pulse, and a precipitating event. 8 These methods have demonstrated high sensitivity and specificity in identifying MC, although a consensus has not been reached. Additionally, a patient’s previous history of thyroidectomy or radioiodine therapy is an important clue to a possible MC diagnosis. Our patient presented with similar clinical symptoms and signs to those in the above-mentioned systems, such as hypoxemia, circulatory failure, and disturbance of consciousness. The final diagnosis was confirmed by thyroid function testing. Although diagnostic criteria for MC have not been validated, these are necessary to help clinicians recognize MC.
There is no single mechanism by which MC leads to hypoxemia. The effects of MC on the respiratory system are complex. The impairment of respiratory muscle function is characterized by a decline in muscular strength. 9 The response of the respiratory center to hypoxia and hypercapnia is diminished, resulting in alveolar hypoventilation. 10 Notably, Ladenson et al. found that impaired ventilatory response occurred mainly in female patients with high TSH levels. 11 Owing to the accumulation of mucopolysaccharides, patients typically present with peri-laryngeal edema and enlargement of the tongue, resulting in airway obstruction. 12 Pulmonary ventilation may be restricted in these patients by the presence of pleural or pericardial effusions, and by ascites. 13 Additionally, patients frequently present with co-existing obstructive sleep apnea and obesity, which lead to respiratory failure. 14 The etiologies of post-operative hypoxemia are diverse, encompassing factors such as diminished chest wall and diaphragmatic activity caused by surgical site pain, hemodynamic impairment, and the effect of anesthetic drugs. 15 In our patient, the severe hypoxemia after extubation was clearly due to MC; however, the hypoxemia was also exacerbated by NPPE secondary to airway obstruction. Likewise, residual neuromuscular blockade should also be considered. MC itself is rare, and its association with hypoxemia is even more uncommon. Therefore, our case is valuable to help in the identification of severe hypoxemia after extubation.
Owing to the high mortality and complexity associated with MC, patients often require transfer to the ICU for treatment. Thyroid hormone replacement is a crucial component of treatment, yet there remains controversy surrounding its use in MC therapy. As T4 is the inactive form and exhibits a smooth action with few adverse effects, it is generally recommended as the first-line therapy for thyroid hormone replacement. Nevertheless, T4 monotherapy may not be optimal owing to its inherent limitations. T4 conversion to triiodothyronine (T3) may be less efficient in patients with MC. 16 The onset of action of T4 is also slower than that of T3. Moreover, T3 exhibited a faster ability to cross the blood–brain barrier in a study involving baboons compared with T4. 17 However, T3 monotherapy can result in significant and unpredictable fluctuations in serum T3 levels, which are associated with adverse cardiac effects. 18 Thus, the American Thyroid Association recommends treatment with T4 alone or combination therapy with both T4 and T3. 19
In patients with MC, there is usually edema of the intestinal wall, which impedes drug absorption. 20 Therefore, parenteral administration of T3 and T4 is generally recommended. It is crucial to administer glucocorticoids prior to thyroid hormone replacement owing to the potential for thyroid hormone therapy to enhance cortisol clearance and precipitate adrenal insufficiency. 21 Supportive therapy is also crucial for patients with MC, comprising airway and circulatory support, correction of electrolyte disturbances, and passive warming. In our patient, as parenteral preparations of T4 or T3 were unavailable, levothyroxine was administered via nasogastric feeding tube. In some reported cases, enteral administration of levothyroxine is a viable treatment option for MC in the absence of parenteral preparations of T4 or T3. 3 , 22 Fortunately, our patient’s final outcome and prognosis were favorable.
NPPE is the result of fluid translocation from the capillaries into the interstitial and alveolar spaces by negative intrathoracic pressure generated by forceful inspiration to overcome upper airway obstruction. 23 NPPE is reported mainly in adults as a consequence of post-operative laryngospasm. 24 The typical clinical presentation comprises hypoxemia, pink frothy sputum, and abnormalities on chest radiographs. 25 In most cases, NPPE resolves rapidly within 24 to 48 hours once the airway obstruction is resolved. 26 In the present case, chest radiographs revealed bilaterally symmetrical and diffuse interstitial and alveolar infiltrates (Figure 1), which are consistent with typical imaging findings of NPPE. Furthermore, echocardiography did not reveal evidence of cardiac systolic or diastolic dysfunction; thus, cardiogenic pulmonary edema was ruled out. During endotracheal intubation, severe peri-laryngeal edema was observed in our patient, which was caused by MC and resulted in upper respiratory obstruction. The primary etiology of NPPE is attributed to the generation of strong inspiratory negative pressure resulting from upper respiratory tract obstruction. 27 Following tracheal intubation and subsequent mechanical ventilation, resolution of the upper airway obstruction in our patient led to gradual resolution of the pulmonary edema (Figure 1).
The young woman in the present case may have had undiagnosed severe hypothyroidism for several years, considering her previous signs and symptoms. Although there was no intra-operative hypothermia, surgery and anesthesia precipitated the onset of MC in this patient. The anesthesiologist was unaware that the patient had developed MC after the operation, and removed the endotracheal tube. Following extubation, the patient experienced severe hypoxemia exacerbated by NPPE due to airway obstruction. Notably, prompt diagnosis and treatment resulted in a favorable prognosis, without complications. Therefore, early identification and timely intervention for hypothyroidism in high-risk patients are crucial in preventing MC.
Conclusion
Although MC is a rare endocrine emergency, anesthesiologists’ awareness should be enhanced, particularly regarding the potential of MC to cause peri-operative hypoxemia. Prompt diagnosis followed by treatment is essential to reduce the mortality rate associated with this condition.
Footnotes
Acknowledgements
The authors thank the anonymous reviewers and the editor for their valuable comments.
Author contributions
Jintao Sun and Qiaoyi Peng collected the data and wrote the original manuscript. Yuefeng Huaguo and Li Hu collected the data. Hongmei Zhou guided the writing of the manuscript. All authors read and approved the final version of the manuscript.
Data availability statement
All of the analyzed data are included in the article. Further inquiries can be directed to the corresponding author.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
We present this case in compliance with the CARE reporting guidelines checklist. 28 This report complies with the tenets of the Declaration of Helsinki and was approved by the medical ethics committee of The Second Affiliated Hospital of Jiaxing University (approval number: JXEY-2022ZFYJ085). The patient’s informed consent was obtained for the publication of this case report and accompanying images.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.