
Abstract
Q fever is an important zoonotic disease caused by the pathogen Coxiella burnetii, which is inhaled into the body through the respiratory tract leading to acute symptoms. Severe acute Q fever may result in complications, such as pneumonia, hepatitis, or myocarditis, and some patients may develop chronic Q fever after incomplete treatment. Local persistent C. burnetii infection may lead to chronic Q fever that often requires surgery and anti-infection treatment for several years, seriously endangering patient health and increasing the economic burden for families. The clinicians’ lack of awareness of the disease may be one reason leading to a delay in treatment. Here, a case of Q fever in a 53-year-old male patient, which was diagnosed by next generation sequencing and exhibited a distinct computed tomographic feature, is reported, with the aim of improving clinical knowledge of this disease. Following diagnosis, the patient was treated with 0.1 g doxycycline, orally, twice daily, and 0.5 g chloramphenicol, orally, three times daily, leading to improvement of symptoms and discharge from hospital.
Introduction
Q fever is a zoonotic disease caused by Coxiella burnetii, with C. burnetii being identified as a potential cause of acute hepatitis in patients with hepatitis of unknown causes. 1 Next generation sequencing (NGS) may be helpful for the identification of C. burnetii in patients with infection, and doxycycline in combination with a fluoroquinolone has been effectively administered for treatment in some cases. 2 The incubation period may be as long as 2–4 weeks after exposure to C. burnetii, and the infection is usually self-limiting. 3 The most commonly identified sources of human infection are farm animals, such as cattle, goats, and sheep. Acute Q fever, caused by C. burnetii infection, usually manifests as influenza-like symptoms, such as high fever, headache, muscle soreness, and general fatigue. In severe cases, complications may occur, such as pneumonia, hepatitis, and myocarditis. Some patients may develop chronic Q fever, with multisystem involvement, and the clinical manifestations are varied and non-characteristic. 4 Q fever may involve the respiratory tract, usually manifesting clinically as atypical pneumonia. The most common abnormalities noted are segmental consolidation, and, less commonly, lobar consolidation.5,6 In some cases, when unclear radiographic findings are present or there is suspicion of a coexistent disease, chest computed tomography (CT) may be requested. The purpose of the present study was to evaluate and discuss CT features in a patient with Q fever pneumonia to improve clinical knowledge of this disease. To the best of the author’s knowledge, Q fever pneumonia with CT showing multiple small pulmonary nodules is rare.
Case presentation
A 53-year-old male patient was admitted to the People's Hospital of Ronchang District, Chongqing, China, in August 2022 due to ‘fever for 8 days’, with the highest temperature of 38.3°C, accompanied by fatigue and poor appetite. Three days before admission, the patient was treated at a different hospital, where a chest radiograph and abdominal colour ultrasound revealed no abnormalities, and the liver examination showed elevated transaminases. The patient recalled that his transaminase level at the previous hospital was approximately 200 U/L, but this could not be verified, as the results report was not provided. Treatment details were unknown, but the treatment effect was poor, so he was transferred to the People's Hospital of Ronchang District for treatment. A road builder in the wilderness, the patient had smoked approximately 10 cigarettes per day for nearly 30 years but had largely stopped smoking in recent years. Physical examination after admission revealed no obvious positive signs in the chest or abdomen.
After admission, relevant examinations were completed. HIV test, electrocardiogram, influenza antigen test, renal function test, five-indicator test for Hepatitis B, routine urinalysis, routine stool analysis, syphilis antibody test, hepatitis C antibody test, blood culture, sputum culture, and sputum smear test showed no obvious abnormalities. D-dimer level was 4.83 µg/mL, and erythrocyte sedimentation rate was 25 mm/h. Liver function test revealed the following: alanine aminotransferase, 141.00 U/L; alanine transaminase, 114.71 U/L; glutamyl transpeptidase, 123.54 U/L; total protein, 60.16 g/L; and albumin, 28.82 g/L. Toxic particles could be seen in white blood cells; C reactive protein level was 64.9 mg/L and procalcitonin level was 9.96 ng/ml. A complete blood count showed no atypical lymphocytes. Routine blood test results showed: platelets, 50 × 109/L; haemoglobin, 123 g/L; leukocytes, 4.9 × 109/L; and neutrophil ratio 58.80%. The radiology report from chest and upper abdomen CT stated the following findings: (1) chronic bronchitis, emphysema with pulmonary bullae; (2) multiple nodules in both lungs (Figure 1); and (3) no significant abnormalities on the upper abdomen CT.
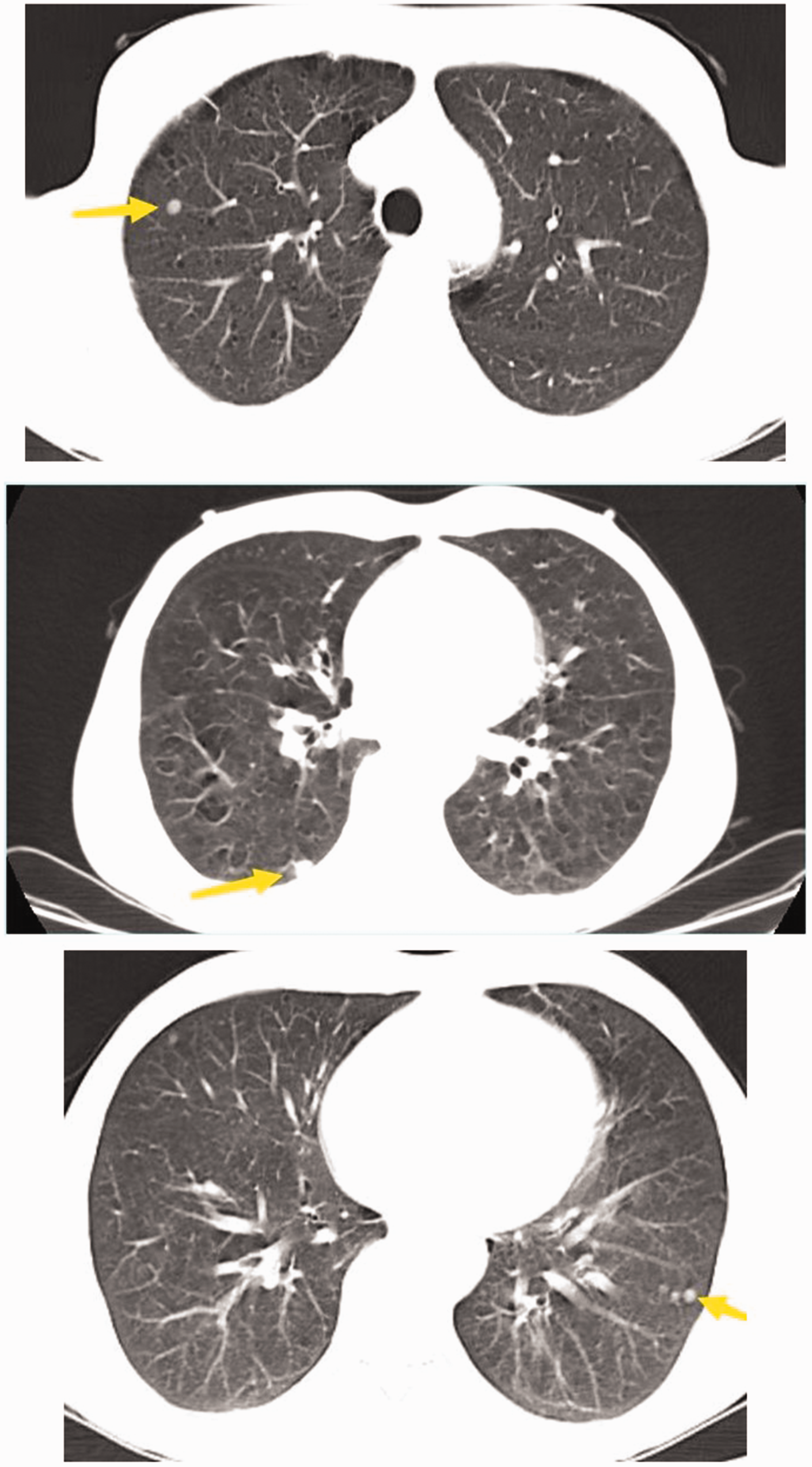
Initial chest computed tomography images from a 53-year-old male patient with Q fever who presented with fever for 8 days previously, accompanied by fatigue, poor appetite and elevated transaminases, showing multiple nodules in both lungs (arrows).
Combining the patient's medical history and relevant examination, a number of potential primary diagnoses emerged. Pneumonia was initially considered, as the patient had a fever with pulmonary nodules shown on chest CT, but there was no obvious cough or sputum production. Liver abscess was considered next, as the patient was febrile with abnormal hepatic function, but there were no significantly abnormalities shown on upper abdominal CT. Other diseases, such as autoimmune disorders, thyroadenitis, and haematological diseases, remained to be considered.
The most common cause of fever is bacterial infection. As the pathogen in the present case was unknown, the patient was initially administered 3 g piperacillin/sulbactam by intravenous (i.v.) drip, twice daily for 4 days (15–18 August 2022) for empirical anti-infection therapy, to cover common bacteria. However, the fever (Figure 2), poor appetite and fatigue remained after anti-infection treatment, so the dual antibiotic treatment was upgraded to strengthen anti-infection by adjusting to 4.5 g piperacillin/tazobactam by i.v. drip, three times daily for 3 days (18–20 August 2022) and 0.4 g moxifloxacin by i.v. drip, once daily for 11 days (from 18 August 2022 to discharge). During this treatment, further aetiological investigation was underway. Total abdominal enhanced CT (Figure 3) showed a small cyst in the left lobe of the liver. Tests for common tumour markers in men, such as carcinoembryonic antigen, cytokeratin 19 fragment, carbohydrate antigen 242, prostate-specific antigen, and alpha-fetoprotein, returned normal results. Therefore, cancerous fever was not considered. Results of autoantibody spectrum tests and markers of immunity, such as immunoglobulin (Ig)A, IgG, IgM, and complement C3 and C4, were also normal. Thus, fever caused by autoimmune diseases was not considered. In addition, thyroid function was normal, so fever caused by thyroiditis was not considered.

Body temperature curve from a 53-year-old male patient with Q fever who presented with fever for 8 days previously, accompanied by fatigue, poor appetite and elevated transaminases.

Abdominal enhanced computed tomography image from a 53-year-old male patient with Q fever who presented with fever for 8 days previously, accompanied by fatigue, poor appetite and elevated transaminases, showing a small cyst in the left lobe of the liver (arrow).
At this point the diagnosis remained unknown, and anti-infective treatment was ineffective, thus, it was necessary to perform a bone marrow needle biopsy for haematological disease. The senior physician (YC-W) at the Department of Respiratory and Critical Care Medicine, People’s Hospital of Rongchang District reviewed the CT film and considered the existence of hepatomegaly, although no obvious other lesions were evident. Of note, radiologists checking the CT images of patients in the respiratory department mainly focus on the lung condition, and the CT showed no abscesses or cysts in the liver. On reviewing and analysing the data of this patient again, the abdominal CT was found to show hepatomegaly, and as the patient exhibited abnormal liver function, fever, thrombocytopenia, and small pulmonary nodules on the chest CT, a pathogen invading multiple organs, including the lungs, was considered. An electronic bronchoscopy was then performed (19 August 2022). A little white sputum was observed in the airway, the airway mucosa was hyperaemic and swollen, and the interridge was widened. Lavage was performed in the posterior basal segment of the outer inferior lobe of the right lung and the basal segment of the outer inferior lobe of the left lung. Routine examination of the lavage fluid showed no bacteria, fungi or tuberculosis. Lavage fluid was sent for NGS (Hangzhou Jieyi Medical Laboratory Co., Yuhang District, Hangzhou, Zhejiang Province, China), and at the same time, peripheral blood was drawn for NGS.
The NGS result (available 20 August 2022) showed that Epstein–Barr virus (EBV) and C. burnetii were detectable in peripheral blood, and C. burnetii was detectable in lavage fluid. EBV is carried by more than 95% of adults. After EBV infects the human body, most people have no symptoms, and only a few people will develop infectious mononucleosis, and lymph node and tonsil enlargement. If mononucleosis occurs, the mononucleosis count in routine blood analysis will be significantly increased, and a skin rash may appear, however, the patient in the present case did not exhibit any of these symptoms. The relative abundance of Q fever detected on the NGS report was 50.56%, and the relative abundance of EBV was 1.67%. Therefore, we considered that simple EBV infection could not explain the patient's condition. EBV colonization and contamination were possible. The patient was diagnosed with Q fever and administered 0.1 g doxycycline, orally, twice daily, according to treatment advice. 7 The patient's temperature increased again on 24 August 2022 (Figure 2), so 0.5 g chloramphenicol, orally, three times daily, was added to the treatment regimen (from 25 August to discharge). On 29 August 2022, the patient's symptoms were relieved, liver function and platelet count returned to normal, and levels of procalcitonin (Figure 4) and C-reactive protein (Figure 5) were significantly decreased. The patient was discharged.

Change in procalcitonin level in a 53-year-old male patient with Q fever who presented with fever for 8 days previously, accompanied by fatigue, poor appetite and elevated transaminases.

Change in C-reactive protein level in a 53-year-old male patient with Q fever who presented with fever for 8 days previously, accompanied by fatigue, poor appetite and elevated transaminases.
Ethics committee approval was not required for this case report, due to the retrospective nature of this study. Signed informed consent was obtained from the patient for publication of this case and his anonymised data. The reporting of this study conforms to CARE guidelines. 8
Discussion
Coxiella burnetii, the causative agent of Q fever, is highly virulent and may cause systemic infection by inhalation of a few bacteria into the respiratory tract. Although acute Q fever is self-limiting and has a low mortality rate, 50% of patients with acute Q fever are reported to require hospitalization, and if treatment is incomplete, chronic Q fever may develop. 4 Chronic Q fever affects the quality of life of patients, and its diagnosis and treatment are difficult, sometimes even requiring surgical intervention;4,9 therefore, early diagnosis and timely treatment are essential. Q fever diagnosis depends on the comprehensive evaluation of epidemiology, clinical manifestations and serum examinations, and a patient history of residence and occupation in an epidemic area are of great reference value for diagnosis, as the disease is easily misdiagnosed. According to the Johns Hopkins ABX guide 2012: diagnosis and treatment of infectious diseases, third edition, 10 and The Sanford Guide to Antimicrobial Therapy, 11 tetracycline, chloramphenicol, erythromycin, roxithromycin, and quinolones are recommended to treat Q fever. In the present case, many examinations were performed, but the diagnosis remained unclear until the NGS result was obtained. In general, quinolones are not the first choice for treating Q fever, and monotherapy may not be effective.12,13 In the present case, piperacillin plus moxifloxacin was first used for anti-infection, but piperacillin was ineffective against Q fever and was subsequently discontinued. With moxifloxacin combined with doxycycline and eventually chloramphenicol, the condition finally improved.
In the present case, multiple small pulmonary nodules were shown on CT, which may have been an inflammatory manifestation of C. burnetii infection in the lungs. The CT manifestations of the chest differed from the common Q fever pneumonia, where typical CT findings of Q fever pneumonia consist mainly of multilobar airspace consolidation. 14 Predominant high-resolution CT findings in patients with acute Q fever pneumonia are bilateral peripheral areas of consolidation and nodules with irregular contours and halos of ground-glass opacity. 15
In conclusion, the clinical manifestations, imaging, and laboratory examinations of acute Q fever are non-specific, so that Q fever may easily be missed and misdiagnosed. When unexplained fever was explored in the present case, CT showed multiple small nodules in the lung accompanied by abnormal liver function, and Q fever could be considered. If the diagnosis is clear and the patient receives timely treatment, the curative effect is generally good.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231183553 - Supplemental material for Q fever represented as multiple pulmonary nodules: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231183553 for Q fever represented as multiple pulmonary nodules: a case report by Yu Zhai in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231183553 - Supplemental material for Q fever represented as multiple pulmonary nodules: a case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605231183553 for Q fever represented as multiple pulmonary nodules: a case report by Yu Zhai in Journal of International Medical Research
Footnotes
Acknowledgement
The author would like to thank Dr Yong-Chang Wu, senior physician at the Department of Respiratory and Critical Care Medicine, People’s Hospital of Rongchang District, for his contribution in diagnosing the patient.
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.