
Abstract
Amyloidosis is a disease caused by amyloid deposition in tissues or organs. According to the extent of the lesion, it can be divided into systemic amyloidosis and localized amyloidosis. Amyloidosis originating in the larynx accounts for approximately 0.5% to 1.0% of benign lesions of the larynx; such lesions are relatively rare and mostly localized. Nasopharyngeal amyloidosis combined with laryngeal amyloidosis is even rarer. We herein present a case involving a patient with amyloidosis in the nasopharynx and larynx who presented with a foreign body sensation and hoarseness in the pharynx. Electronic fiber laryngoscopy revealed a smooth neoplasm in the left nasopharynx and left vocal cord. The patient underwent surgical treatment, and the postoperative pathologic examination results suggested amyloidosis. Special staining performed using Congo red and crystal violet was positive, confirming amyloidosis. The patient recovered after surgery, and no recurrence was present at the 3- and 6-month follow-ups.
Keywords
Introduction
Primary immunoglobulin light chain amyloidosis (AL amyloidosis) is an autoimmune disease of unknown etiology and multisystem involvement. Amyloid protein can deposit in various organs, resulting in structural and functional abnormalities and corresponding clinical symptoms and signs. The chemical composition of amyloid is 90% amyloid fibrin and 10% glycoprotein, and the deposited amyloid fibrils are the main cause of amyloidosis. Deposition of amyloid fibrils or nonfibrous oligomers induces atrophy and subsequent degeneration of adjacent cells in patients with amyloidosis. 1 The disease develops slowly and can recur if not properly treated. Treatment is based on the extent of the lesions, choice of operation for complete resection of the lesion, and postoperative long-term follow-up. The occurrence of amyloidosis in the head and neck is relatively rare. We herein report a case of simultaneous amyloidosis in the nasopharynx and larynx with no recurrence after surgical treatment.
Case report
A 51-year-old man was admitted to our hospital because of a 1-month history of hoarseness. One month prior to presentation, the patient had developed hoarseness of unknown etiology accompanied by a foreign body sensation in the pharynx. Nasal congestion and postnasal dripping were also present. Electronic fiber laryngoscopy revealed a smooth mass on the left side wall of the nasopharynx and a mass on the left vocal cord (Figure 1). Enhanced computed tomography (CT) showed an increased volume of the left torus tubarius, thickening of the left wall adjacent to the nasopharynx, and a soft tissue density shadow. The lower boundary of the nasopharyngeal mass reached the uvula, the size of the mass was approximately 1.2 × 1.1 cm, and the left vocal cord was irregular in shape (Figure 2). Based on the findings of combined electronic fiber laryngoscopy and enhanced CT examination, the neoplasm was considered a benign lesion. We adopted the following treatment plan for the patient: the nasopharyngeal and left vocal cord masses were removed using a plasma knife and support laryngoscope, respectively. The root pedicle of the mass in the nasopharynx was located on the left wall of the nasopharynx. The mass had a smooth surface, no obvious capsule, and brittle tissue texture, and it was completely removed using a low-temperature plasma knife. Further examination under supported laryngoscopy showed that the vocal cord mass was located in the anterior third of the left vocal cord and had a smooth surface, similar to the nasopharyngeal neoplasm. The lesions were considered identical and completely resected using microscopic scissors. On postoperative pathological examination, the nasopharyngeal and left vocal cord masses were inhomogeneously stained red, and amyloidosis was considered. We performed special staining to further clarify the biological properties of the nasopharyngeal and vocal cord masses, and the results were positive for Congo red and crystal violet staining (Figure 3). The patient was diagnosed with amyloidosis and remained clinically stable for 6 months of follow-up.
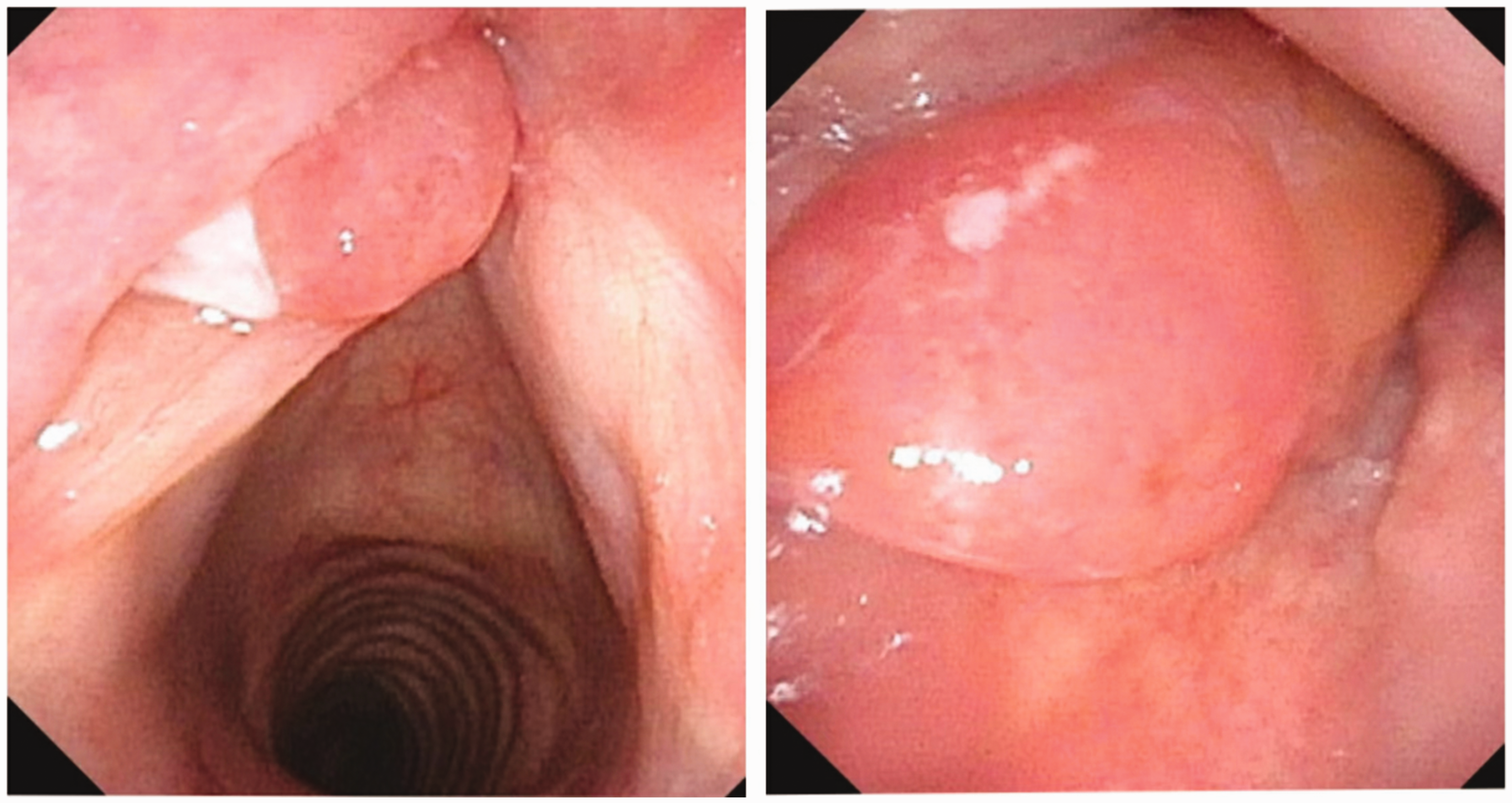
(a) Laryngoscopy showed a mass on the left vocal cord, approaching the anterior third of the left vocal cord and exhibiting a smooth surface and (b) A mass was observed in the left lateral wall of the nasopharynx with a smooth surface and clear boundary.

Soft tissue density nodules were present in the left nasopharyngeal region.
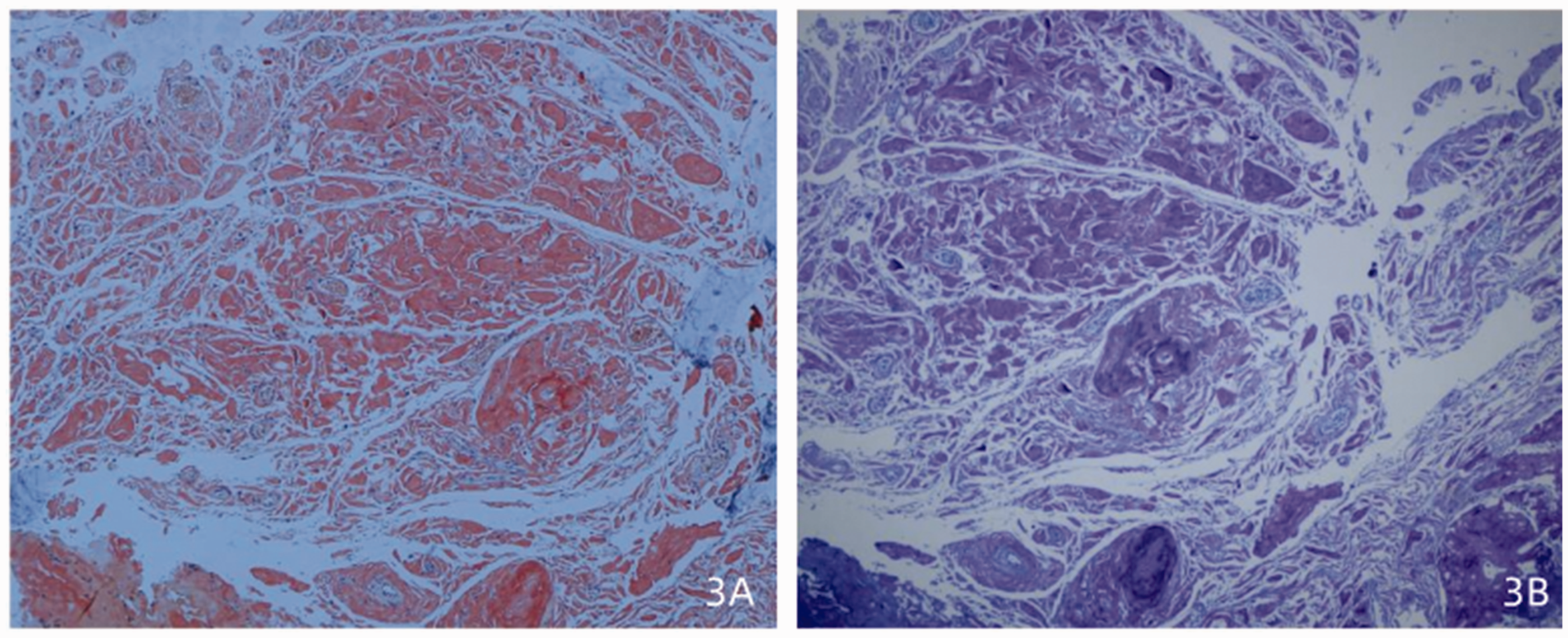
Histopathological section of the nasopharynx of the patient. (a) Extracellular amyloid deposition stained brick red (Congo red, ×100) and (b) Extracellular deposition of amyloid protein stained bluish-purple (crystal violet, ×100).
Discussion
Amyloidosis was first described by von Rokitansky 2 in 1842. Virchow 3 later discovered that the protein is stained purple with iodine and sulfuric acid, hence the name amyloidosis. Amyloidosis is a heterogeneous disease characterized by bundles of β-folding proteins that lead to the transformation of soluble proteins into insoluble pathogenic proteins. This ultimately affects the normal function of proteins and can lead to organ failure. 4 More than 30 proteins form amyloid deposits in humans; however, only 14 of them cause amyloidosis. 5 The most common types of systemic amyloidosis are immunoglobulin light chain (AL), reactive (AA), mutant or wild-type transthyretin (ATTR), fibrinogen (AFib), and apolipoprotein A-I (AApoAI). Clinically, the disease can be systemic or localized depending on its scope. 5 Systemic amyloidosis has a high incidence and mostly occurs in the heart, kidney, and digestive tract. Localized amyloidosis has a low incidence and can occur in the bladder, spleen, and head and neck. Amyloidosis in the head and neck is rare, with the larynx being the most commonly affected site. 6 The patient in the present case had nasopharyngeal amyloidosis with laryngeal involvement, which is extremely rare. Amyloid protein can involve different organs and lead to different clinical symptoms. Deposition of amyloid protein in different locations of the head and neck can cause hoarseness, a foreign body sensation in the pharynx, dysphagia, cough, and nasal obstruction. 7 Patients with AL amyloid cardiomyopathy develop dyspnea and right heart failure. Urinary protein is a free monoclonal immunoglobulin light chain that can cause renal damage. The clinical manifestations in the present case were mainly nasopharyngeal and laryngeal symptoms. The diagnosis is based on biopsy and Congo red staining. 8 The nascent polypeptide chains of amyloid consist of ribosomes and are arranged in alpha or beta chains. Moreover, the body does not have an enzyme to digest the β-fold structure of macromolecules; therefore, the structure of the β-amyloid protein can cause amyloid amyloidosis to have polar birefringence characteristics, exhibiting apple-green birefringence under a polarizing microscope. Amyloidosis manifests as a benign lesion with slow development, gradually developing and affecting body functions. In the early stage, imaging examinations such as laryngoscopy, CT, and magnetic resonance imaging can be used to determine the shape and growth range of the tumor for early treatment. Systemic amyloidosis is mainly treated with chemotherapy, whereas localized lesions are mostly treated with surgical resection to eliminate symptoms. The prognosis of patients with systemic amyloidosis is poor. 9 It has been reported that with the extension of the chemotherapy cycle, the effective rate of chemotherapy drugs for systemic amyloidosis does not increase; however, their adverse effects increase significantly, leading to organ decompensation and functional failure. 10 After surgical treatment, the long-term efficacy of local amyloidosis in the head and neck is satisfactory, but the recurrence rate is high mostly because of incomplete excision of the lesion. 11 In the present case, the patient’s hoarseness improved and foreign body sensation in the pharynx disappeared after surgical treatment. The patient was followed up at 3 and 6 months after the operation and showed good recovery in the operative area and a stable clinical condition.
Conclusions
Amyloidosis is rare and manifests as solid lesions with no specific clinical manifestations. Clinicians must be vigilant and attain the diagnosis as soon as possible to avoid misdiagnosis. Local amyloidosis can be treated by surgery, and the prognosis is good; however, it should be monitored regularly to prevent recurrence.
Footnotes
Authors’ contributions
Yu Feng: data collection and manuscript preparation, Maocai Li and Dong Liu: manuscript preparation, Yongya Du and Lili Gong: acquisition of images, Lianqing Li: manuscript preparation and review. All authors read and approved the final manuscript.
Consent for publication
The patient provided written informed consent for the publication of this case report.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics approval
This article was approved by the Ethics Committee of Liaocheng People’s Hospital (approval no. 20180603; approval date: 20 July 2022).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.