
Abstract
Objective
Although the prevalence of autism spectrum disorder (ASD) is increasing, appropriate diagnosis and prevention strategies are still lacking. This case–control study was designed to explore the association between ASD and the rs1867503 and rs9951150 polymorphisms of the TF and TCF4 genes, respectively.
Methods
Ninety-six children with ASD and 118 healthy children were recruited and polymerase chain reaction–restriction fragment length polymorphism technique was applied for genotyping.
Results
The frequencies of the mutant allele G were 48% and 44% for the rs1867503 and rs9951150 polymorphisms, respectively. In our analysis, both TF and TCF4 polymorphisms were associated with an increased risk of developing ASD. AG heterozygotes (OR = 3.18), GG mutant homozygotes (OR = 2.62), AG + GG combined genotypes (OR = 2.98), and G mutant alleles of TF rs1867503 (OR = 1.94) were associated with a significantly elevated risk of ASD. Likewise, AG heterozygotes (OR = 2.92), GG mutant homozygotes (OR = 2.36), AG + GG combined genotypes (OR = 2.72), and G minor alleles of TCF4 rs9951150 (OR = 1.92) were associated with a significantly elevated risk of ASD.
Conclusions
Our results indicate that TF rs1867503 and TCF4 rs9951150 polymorphisms may be strongly associated with the development of ASD in Bangladeshi children.
Keywords
Introduction
Autism spectrum disorders (ASDs) are neurodegenerative disorders that are diagnosed primarily based on children’s behaviors and characterized by insufficient development of normal social interaction with other people, impaired development of communicative ability, a lack of imaginative ability, and repetitive and stereotyped movements.1–3 Anatomical and physiological changes such as frontal cortex overgrowth occur in the ADS brain during the prenatal period.4,5 Underdeveloped cognitive areas affect decision-making, communication, and language. 5 A 2017 statistic suggests that the prevalence of ASD among children was 168, 161, 152, 100, 100, 69, 67, 49, 27, and 9.2 per 10,000 in the United States, Japan, Canada, the United Kingdom, Ireland, Denmark, Australia, China, Brazil, and Portugal, respectively. 6 The latest published data indicate that the prevalence of ASD is greater than 2%. 7 The diagnosis of ASD nevertheless currently lacks a unifying theory. 8 Early theories about the cause of ASD mainly focused on substandard parenting. 8 Newschaffer et al. 9 suggested that the causes of ASD mainly fall into three categories: genetic, environmental, and neurobiological. Factors including toxicity, teratogenic effects, trauma, and infections can also cause ASD.
Several independent studies and substantial evidence confirm that transferrin (TF; chromosomal location: 3q22.1) is one of the genes that confer susceptibility to ASD.10,11 Transferrin is an iron-transporting plasma glycoprotein that controls iron levels in biological fluid. 10 The glycoprotein has two iron binding sites; these irons accumulate rapidly at the onset of myelination. A very recent study suggested that an elevated amount of oxalate in plasma plays a role in ASD by binding to the bilobal iron transport protein transferrin (hTF), thereby interfering with iron metabolism by inhibiting iron delivery to cells. 11 Therefore, the genetic modification of the transferrin gene may be linked to the development of ASD. 12 An investigation of the rs1867503 polymorphism of the TF gene reported that this genetic polymorphism plays a significant role in producing cognitive disorders such as ASD. 13
Another gene related to ASD is transcription factor 4, 18q21.2 (TCF4; also known as E2-2, SEF2, or ITF2), a basic helix–loop–helix transcription factor that is frequently associated with cognitive dysfunction.14–16 The autosomal dominant mutation or deletion of TCF4 results in Pitt–Hopkins syndrome , 18q deletion syndrome, and three rare ASDs (autistic disorder, Asperger syndrome, and pervasive developmental disorder).17–19 A previous study indicated that in neurodevelopmental pathways TCF4 target genes cluster mostly to schizophrenia, ASD, and ID risk genes. 20 Studies such as this have proven the association of these genes with ASD in some ethnic groups.
A study to validate the link between the TCF4 rs9951150 and TF rs1867503 variants and ASD in Bangladeshi children has not yet been conducted. We performed this study because the diagnosis and treatment of ASD in Bangladeshi children are not adequately prioritized despite a prevalence nearly equal to that in other parts of the world. The study was conducted using polymerase chain reaction (PCR)-based amplification followed by a restriction fragment length polymorphism (RFLP) method to detect the associations of TF rs1867503 and TCF4 rs9951150 with ASD. We anticipate that this study will help further elucidate ASD and improve procedures for its diagnosis and treatment.
Methods and Materials
Study design and sample and data collection
Two groups of children were selected for this case–control study. The first group consisted of 96 children with ASD (aged 3–15 years) who were recruited as cases from schools for children with ASD in Chittagong and Dhaka using the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition. We de-identified all patient details. A total of 118 healthy children (aged 3–15 years) were recruited as controls from areas in Dhaka and Chittagong, Bangladesh. All participants were randomly selected to investigate the risk of ASD due to the TF rs1867503 and TCF4 rs9951150 polymorphisms.
Genotyping analysis was performed in the Laboratory of Pharmacogenomics and Molecular Biology, Department of Pharmacy, Faculty of Science, Noakhali Science and Technology University, Noakhali, Bangladesh. Ethical clearance was obtained from the ethical committee of the Noakhali Science and Technology University (ID-01/2018) and written consent was obtained from each participant before inclusion in the study. We collected consent from guardians for minors or those lacking the capacity to consent. Consent was obtained verbally and in writing (signature or fingerprints). The consent form was translated into the native language to ensure accurate understanding by participants.
The study was conducted in accordance with the International Conference of Harmonization for Good Clinical Practice and was in compliance with the Declaration of Helsinki and its further amendments. 21 Moreover, the study was performed following the Strengthening the Reporting of Observational Studies in Epidemiology guidelines, as described by von Elm et al. 22
Selection of genes and single nucleotide polymorphisms
We selected additional ASD-susceptible genes and polymorphisms by analyzing their possible association with ASD. Transferrin factor is important for iron transportation 12 and lower iron levels are linked with ASD.23,24 A genome-wide association study found a link between the rs1867503 polymorphism and ASD. 13 Another study reported the association of TCF4 with autism. 20 Moreover, the frequency of the minor allele must be greater than 15% according to the 1000 Genomes database in the studied population.
DNA extraction and genotyping
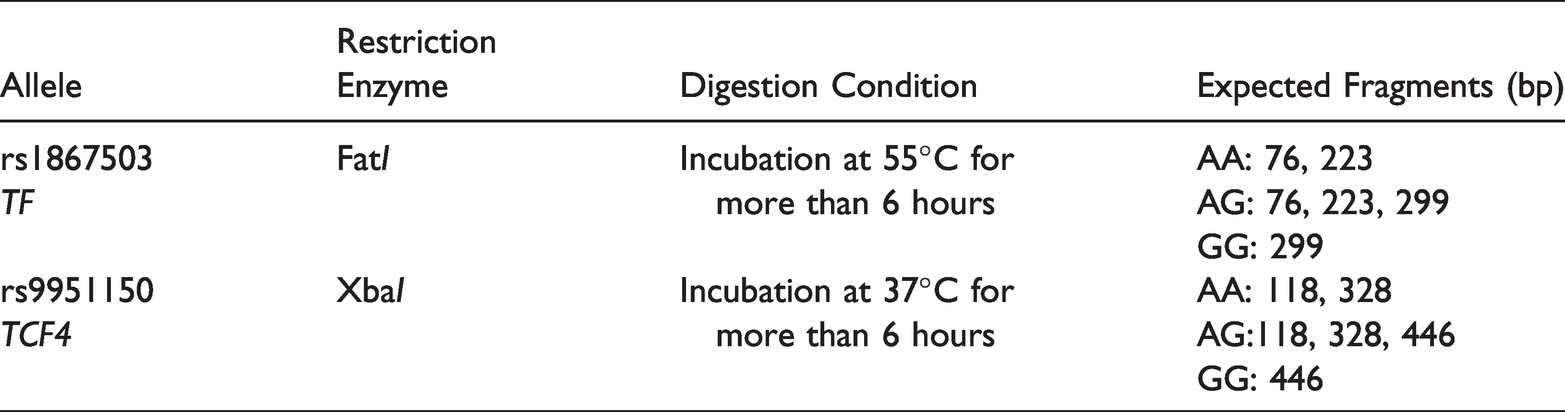
Approximately 3 mL of blood was drawn from all patients and controls into a tube containing ethylenediaminetetraacetic acid disodium and stored at −80°C until the isolation of genomic DNA.25,26 Genomic DNA was isolated from 96 children with ASD and 118 controls using the FavorPrep™ DNA isolation kit (Favorgen Biotech Corporation, Ping-Tung, Taiwan). The genotyping of the selected single nucleotide polymorphisms (SNPs) was performed using the PCR-RFLP method. The PCR conditions for rs1867503 consisted of an initial denaturation at 95°C for 3 minutes, 35 cycles of 95°C for 20 s, 55°C for 30 s, 72°C for 30 s, and a single-step final extension at 72°C for 5 minutes. The PCR conditions for the amplification of rs9951150 were similar except that the annealing temperature was 57°C instead of 55°C. After completion of PCR amplification, PCR products of 299 and 446 bp in size were obtained for rs1867503 and rs9951150, respectively, and were visualized in 1% (w/v) agarose gel. Targeted polymorphisms were identified by digesting with respective restriction enzymes under the conditions mentioned in Table 1.
Restriction enzyme digestion conditions and expected fragments.
Statistical Calculation
SPSS software package version 16.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The deviation of variable allele frequencies in the control group from that of the patient group was assessed according to the Hardy–Weinberg equilibrium (HWE) and the chi-square test (χ2). The genotype and allelic frequencies were reported as percentages. We evaluated the association of SNPs with ASD using genetic models including additive models and recessive and dominant models.27,28 SPSS was further used to estimate odds ratios (ORs) and their 95% confidence intervals (CIs). For all analyses, a p-value of less than 0.05 was used to determine statistical significance. Statistical power was calculated using an online sample size estimator (OSSE; http://osse.bii.a-star.edu.sg/).
Results
All cases and controls were from the same ethnic group and were Bangladeshi by birth. The genotype frequencies of TF rs1867503 and TCF4 rs9951150 were analyzed for 96 children with ASD and 118 healthy children. The distribution of demographic characteristics among study participants is summarized in Table 2. Among children with ASD, 70.83% were boys and 29.17% were girls, whereas 38.98% were boys and 61.02% were girls among controls. Average ages were 10.06 years and 10.81 years in the ASD and control groups, respectively.
Distribution of demographic variables of autism spectrum disorder children and controls.

Post-study statistical power calculation with OSSE (http://osse.bii.a-star.edu.sg/) using the minor allele frequencies of 48% in cases and 32% in controls for rs1867503 to achieve 80% power showed that the 292 samples (146 cases + 146 controls) were required to achieve 80% statistical power. Given the sample size (96 cases and 118 controls), the statistical power of the study was 66.3%.
In the case of the rs1867503 SNP of the TF gene, 27.08% of children with ASD and 52.54% of controls carried the AA genotype. Fifty percent of children with ASD and 30.51% of controls carried the AG genotype, whereas 22.92% of children with ASD and 16.95% of controls carried the GG genotype. The frequencies of the G allele were 47.92% and 32.20% among children with ASD and controls, respectively. The chi-square values for the ASD and control groups were 0.0003 and 10.71, respectively. The frequency distribution of ASD cases and controls did not obey the HWE (p < 0.05; Table 3).
Allelic frequencies and Hardy–Weinberg equilibrium of rs1867503 genotypes among children with autism and healthy controls and their association with ASD.

p < 0.05 is considered statistically significant and p > 0.05 indicates consistency with Hardy–Weinberg equilibrium.
The G allele frequencies were 43.75% in patients and 28.81% in controls for the TCF4 gene’s rs9951150 SNP. The genotype frequencies of the rs9960767 variant were as follows: AA, 33.33%; AG, 45.83%; and GG, 20.83% in patients and AA, 57.63%; AG, 27.12%; and GG, 15.25% in controls. Only the genotype distribution data of ASD cases followed the HWE (p > 0.05: Table 4).
Allelic frequencies and Hardy–Weinberg equilibrium values of rs9951150 genotypes among children with autism and healthy controls and their association with ASD.

p < 0.05 is considered statistically significant and p > 0.05 indicates consistency with Hardy–Weinberg equilibrium.
In the case of the rs1867503 SNP of the TF gene, children carrying the AG genotype were at 3.18 times higher risk (OR = 3.18, 95% Cl = 1.69–5.97) of developing ASD compared with children carrying the AA genotype (p < 0.05). Children with the GG genotype were at 2.62 times higher risk (OR = 2.62, 95% Cl = 1.22–5.60) of developing ASD compared with children carrying the AA genotype (p < 0.05). Children carrying the combined AG + GG genotype (dominant model) were at 2.98 times higher risk (OR = 2.98, 95% Cl = 1.67–5.31) for the development of ASD compared with children carrying the AA genotype (p < 0.05). However, children carrying the G allele were at 1.94 times higher risk (OR = 1.94, 95% Cl = 1.31–2.87) of developing ASD compared with children carrying the A allele (p < 0.05; Table 3 and Figure 1).

Forest plot of the TF gene’s rs1867503 allele in the study population.
Table 4 shows the allelic frequencies of TCF4 rs9951150 genotypes among children with ASD and healthy controls and their association with ASD. Children carrying the AG genotype were at 2.92 times higher risk (OR = 2.92, 95% Cl = 1.57–5.43) of developing ASD compared with children carrying the AA genotype (p < 0.05), whereas children carrying the GG genotype, were at 2.36 times greater risk (OR = 2.36, 95% Cl = 1.10–5.06) of developing ASD compared with children carrying the AA genotype (p < 0.05). Children with the combined AG + GG genotype (dominant model) were at 2.72 times greater risk (OR = 2.72, 95% Cl = 1.55–4.76) for the development of ASD compared with controls carrying the AA genotype (p < the 0.05), whereas children carrying the G allele were at 1.92 times greater risk (OR = 1.92, 95% Cl = 1.29–2.87) of developing ASD compared with controls carrying the A allele (p < 0.05). No associations were observed between ASD and the recessive model (GG vs. AA + AG) of both SNPs in the population studied (Figure 2).

Forest plot of the TCF4 gene’s rs9951150 allele in the study population.
Finally, the genotype data for TF rs1867503 and TCF4 rs9951150 for cases and controls were distributed according to sex. No significant difference was observed in the genotype distribution between males and females for both SNPs (p > 0.05; Table 5).
Sex-based distribution of TF rs1867503 and TCF4 rs9951150 genotype data.

Discussion
Though the prevalence of ASD increases daily, appropriate diagnosis and prevention strategies are still lacking. 29 The heritability of ASD is 90%. However, identifying relevant genes responsible for the development of ASD remains challenging. 30 Multiple studies are underway to identify responsible genes. Hundreds of genes have already been positively linked to the development of ASD; these genes follow various biochemical pathways to perform their functions.10–12 Ours was the first-ever attempt to investigate the association of TF and TCF4 gene polymorphisms with ASD in Bangladesh and our initial findings are discussed.
Several studies have suggested the role of TF (rs1867503) and TCF4 (rs9951150) in a variety of psychiatric symptoms and diseases including phobic anxiety, obsessive-compulsive disorder, schizophrenia, and attention-deficit hyperactivity disorder. The TF polymorphism causes an increase or decrease of oxygen free radicals, which cause damage to neurons with the excess production of lipid peroxidation and are thus responsible for the oxidative stress associated with neurodegenerative disorders. 31 This polymorphism further causes the additional formation of ferrous, which stimulates hydroxyl formation and leads to brain cell damage. 32 The presence of a larger amount of the antioxidant superoxide dismutase—a marker of lipid peroxidation—was observed in a healthy group of Egyptian children than in an ASD group, indicating the polymorphism of transferrin.33,34
In this research, 118 healthy volunteers and 96 individuals with ASD were studied for the rs1867503 SNP of the TF gene. We observed a significant association between rs1867503 and ASD in Bangladeshi children. Children carrying the AG and GG genotypes were at 3.18 and 2.62 times greater risk, respectively, for the development of ASD compared with children carrying the AA genotype (p < 0.05). A statistically significant (p < 0.05) association with ASD was further observed in children carrying the combined AG + GG genotype (OR = 2.98, p = 0.0002), whereas children carrying the G allele were at 1.94 times greater risk for the development of ASD compared with controls carrying the A allele (p < 0.05). A comparative study conducted by Chauhan et al. 33 indicated an elevated level of lipid peroxidation in children with autism compared with their siblings without autism. The authors further detected increased oxidative stress, which is caused by reduced transferrin. A reduction in transferrin is also responsible for language difficulties in children with ASD. A study by Luck et al. 12 concluded that oxalate in plasma could play a role in ASD by interfering with iron transport by binding with transferrin (hTF) and that high levels of oxalate can cause iron deficiency anemia in children with ASD. Our SNP finding study also suggests such a relationship with ASD.
The TCF4 polymorphism disrupts the columnar and laminar structure of the cortex, which is activity-dependent. The polymorphism further hampers calcium activity, which is responsible for neuronal excitability. These activities result in various autistic syndromes in children. 35 A study of TCF4 regulation concluded that TCF4 encodes a basic helix–loop–helix transcription factor that merges with other factors to activate or suppress gene expression, causing two rare ASDs: Pitt–Hopkins syndrome and 18q deletion syndrome. 36 Our study validates some of the findings of previous researchers.35,36
In the case of the rs9951150 SNP of TCF4, children carrying the AG and GG genotypes were at 2.92 and 2.36 times greater risk of developing ASD compared with controls carrying the AA genotype (p < 0.05). Children carrying the combined AG + GG genotype were at 2.72 times greater risk for the development of ASD compared with controls carrying the AA genotype (p < 0.05), whereas children carrying the G allele were at 1.92 greater risk for the development of ASD compared with controls carrying the A allele (p < 0.05).
This study also reported a higher frequency of ASD in males (70.83%) compared with females (29.17%) in our study (male:female ratio = 2.43:1). Previous studies showed differences between male participant and female participants. 37 This difference may be attributed to the lack of accurate and early diagnosis; this assumption must be confirmed before drawing implications from the findings. 37 The minor allele frequencies in the Bangladeshi population were 32.20% and 28.8% for rs1867503 and rs9951150, respectively, in healthy controls and 47.92% and 43.75% for rs1867503 and rs9951150, respectively, in children with ASD. According to the 1000 Genomes database, the frequency we reported for rs1867503 is higher than that in the African population (21.9%) and close to that of the East Asian population (30.9%) for rs9951150. This study is significant considering the low number of autism-based genetic association studies in Bangladesh, where genetic studies on children with ASD are scarce because of the paucity of research funds. Our study population has a distinct genetic lineage that has been investigated earlier. 26 Moreover, a lack of proper healthcare support was found to improve the quality of life of children with ASD. We hope that our study will encourage healthcare providers and policymakers to appropriately diagnose children with ASD and provide them with the necessary genetic-based treatment.
Our finding supports the conclusion that the rs1867503 and rs9951150 SNPs are strongly associated with the development of ASD. We hope that our identification of the genetic basis of ASD in Bangladeshi children will help elucidate ASD etiology. Given that all cases and controls were from the same ethnic group and were Bangladeshi by birth, statistical biases due to ethnicity were unlikely. However, some study limitations should be noted. Only two known SNPs were selected from a public database; novel SNPs were not studied. Another limitation is that our study population was not large enough for the study to generate nationally generalizable results. Although we detected a strong association of SNPs with the development of ASD, a large-scale study may provide stronger evidence in the future.
Conclusion
This case–control study reveals that TF rs1867503 and TCF4 rs9951150 polymorphisms may be significantly associated with ASD in Bangladeshi children. Ours is the first study of these polymorphisms in Bangladesh. The results are significant despite a limited number of cases and controls. We expect that the findings of this study will guide further large-scale studies.
Footnotes
Acknowledgements
The authors are thankful to the Laboratory of Pharmacogenomics and Molecular Biology and the Department of Pharmacy, Noakhali Science and Technology University, for providing lab support to conduct this research work.
Author Contributions
MA, MSH, MAA: Blood sample collection; MAA, MB, NS, MAR: DNA extraction; MA, MSH, MAA, MB, NS, MAR, MS: PCR analysis and initial draft preparation; MA, MAB, MB, NS, MAR, MS: Data analysis, critical review, and interpretation of results; SSB and GMA: Conception and manuscript editing; MSI: Conception, supervision, institutional approval, editing, final check, and submission.
Availability of data and materials
All relevant data and study materials have been provided in the manuscript. Further information on data and study materials will be available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare no conflicting interests in preparing this article.
Funding
The authors disclosed receipt (pending publication) of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Department of Pharmacy, University of Asia Pacific and Research Cell, Noakhali Science and Technology University, Bangladesh. This work was also funded by the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Saudi Arabia under grant no. (KEP-4-140-42); therefore, the authors thank the Deanship of Scientific Research for its technical and financial support.