
Abstract
Objective
Radial head arthroplasty (RHA) is the principal treatment option for comminuted radial head (RH) fractures. Here, we present six cases of failed RHA using a modular monopolar press-fit RHA that was subsequently withdrawn from the market because it was associated with a high incidence of loosening.
Methods
We retrospectively collected data from six patients who had received Radial Head Prothesis SystemTM at our centre between July 2015 and June 2016. The average follow-up was 40 months.
Results
Aseptic loosening of the stem affected five (83%) of the six RHA. Four of these were symptomatic and RHA removal was performed. For these patients, the pain subsided and their elbow range of motion (ROM) improved.
Conclusion
While the ideal design for an RHA is still debatable, RHA is an efficient treatment option that restores elbow stability and function after a comminuted RH fracture. Importantly, removal of the prosthesis is an effective remedy following RHA associated elbow pain and decreased ROM.
Introduction
Radial head (RH) and neck fractures are common and account for approximately one third of all elbow fractures.1–3 They typically occur following a fall on an outstretched arm with the forearm in pronation, and fracture of the RH results from impaction on the capitellum. 4 Conservative treatment is used for nondisplaced fractures, with surgery reserved for more severe cases. The three surgical options are: open reduction and internal fixation (ORIF), excision of the head or radial head arthroplasty (RHA). Mason type III and IV fractures have a poor outcome if treated by ORIF when the fracture has more than three fragments. 5 RHA improves functional outcomes in complex fractures6–9 and is now commonly used as the primary treatment.
Different designs for RHA are available and can be classified in several ways. For example, one way is to define the RHA by stem fixation, of which there are four groups: press-fit; intentionally loose; cemented; expandable stems. 10 Additionally, RHA prostheses can be monopolar or bipolar, and constructed of cobalt-chromium, pyrocarbon, vitallium, titanium or silicone. Interestingly, there is no evidence to show superiority of one material over another. 10 However, the silastic prosthesis (i.e., the Swanson implant, Dow Corning Corporation, USA) has been found to have a high rate of revision,11,12 secondary to its propensity to create wear particles that induce an inflammatory response and synovitis. 13 The silastic prosthesis is also associated with a high rate of implant fractures 14 and has poor capacity to restore valgus stability because of its low stiffness.15,16
A modular, monopolar press-fit RHA (The DePuy Synthes Radial Head Prosthesis System, DePuy Synthes – Johnson & Johnson, New Brunswick, New Jersey, USA) was used at our centre from 2015 to 2016. The advantage of this implant was related to its modular components. This feature made it easy to use because it was adjustable to the anatomy of the patient and so reduced the risk of overstuffing 17 and residual instability, 18 which are known causes of RHA failure. However, during patient follow-up, a significant proportion of patients developed osteolysis and aseptic stem loosening. The prosthesis was subsequently withdrawn from the market for this reason. The aim of this article is to present a review of the six patients who received this prosthesis at our institution.
Patients and Methods
Between July 2015 and June 2016, six patients received Radial Head Prothesis SystemTM at our centre. All the surgeries were performed through a lateral Kocher approach by one surgeon (F.V.). Any associated ligamentous injuries were addressed at the time of surgery. The prothesis is modular and the radial head locks to the stem by taper locking with a connection screw that allows 10 stem options (i.e., five short straight stems and five long curved stems) and 24 heads (i.e., six different diameters with four different heights) to reconstruct the anatomy of the proximal radius. The heads are round and symmetrical in shape, and are composed of cobalt/chrome. The stems are made of titanium and designed to be press-fit, with a rough coated surface allowing bony ongrowth.
Post operatively, range of motion (ROM) was restricted with the use of a hinged brace or a removable cast with a flexion/extension of 30–130° and full pronation/supination at 90° of flexion. Physiotherapy was adapted according to the associated ligamentous injuries. Follow-up reports were used to evaluate the outcome of each patient, based on history, physical examination and X-rays. Osteolysis was localized on the X-rays and classified according to a modified Gruen 19 classification for the elbow 20 (Figure 1).

Modified Gruen 29 classification for the elbow.
The reporting of this study conforms to CARE guidelines. 21 All participants provided written informed consent. Patient data were anonymized prior to analysis. The study was approved by the hospital ethics committee (Commission Cantonale d’Ethique de la Recherche sur l’Etre Humain – Lausanne, N° 2017-01430).
Results
At the time of surgery, the average age of the five men and one woman was 47 years (range 27–63 years). In four cases, the mechanism of injury was high energy trauma and in two cases it was low energy trauma. For five cases, the indication for RHA was Mason IV fracture and in one case it was Mason III fracture. Five were implanted as primary treatment and one as a secondary treatment following failure of osteosynthesis. Average follow up, defined as the time between the injury and the last available appointment, was 40 months (range, 23–68 months).
Initially, all six patients had a good outcome with minimal pain and improvement in ROM. However, X-rays showed the presence and progression of osteolysis around the stem in five (83%) cases. In two of these cases, osteolysis first started at the tip of the stem (area numbers 3-4-5; Figure 2), in two other cases it started at the proximal part of the stem (area numbers 1-2 and 6-7; Figure 3) and in the remaining case it started all around the stem. First signs of lucency were visible as soon as three months post operatively. In these five cases, the osteolysis progressed around the stem, culminating with a loose stem 6–12 months following surgery (Figure 4). Four of the cases were symptomatic (i.e., pain during loading of the elbow) and removal of the prosthesis was conducted in these patients.
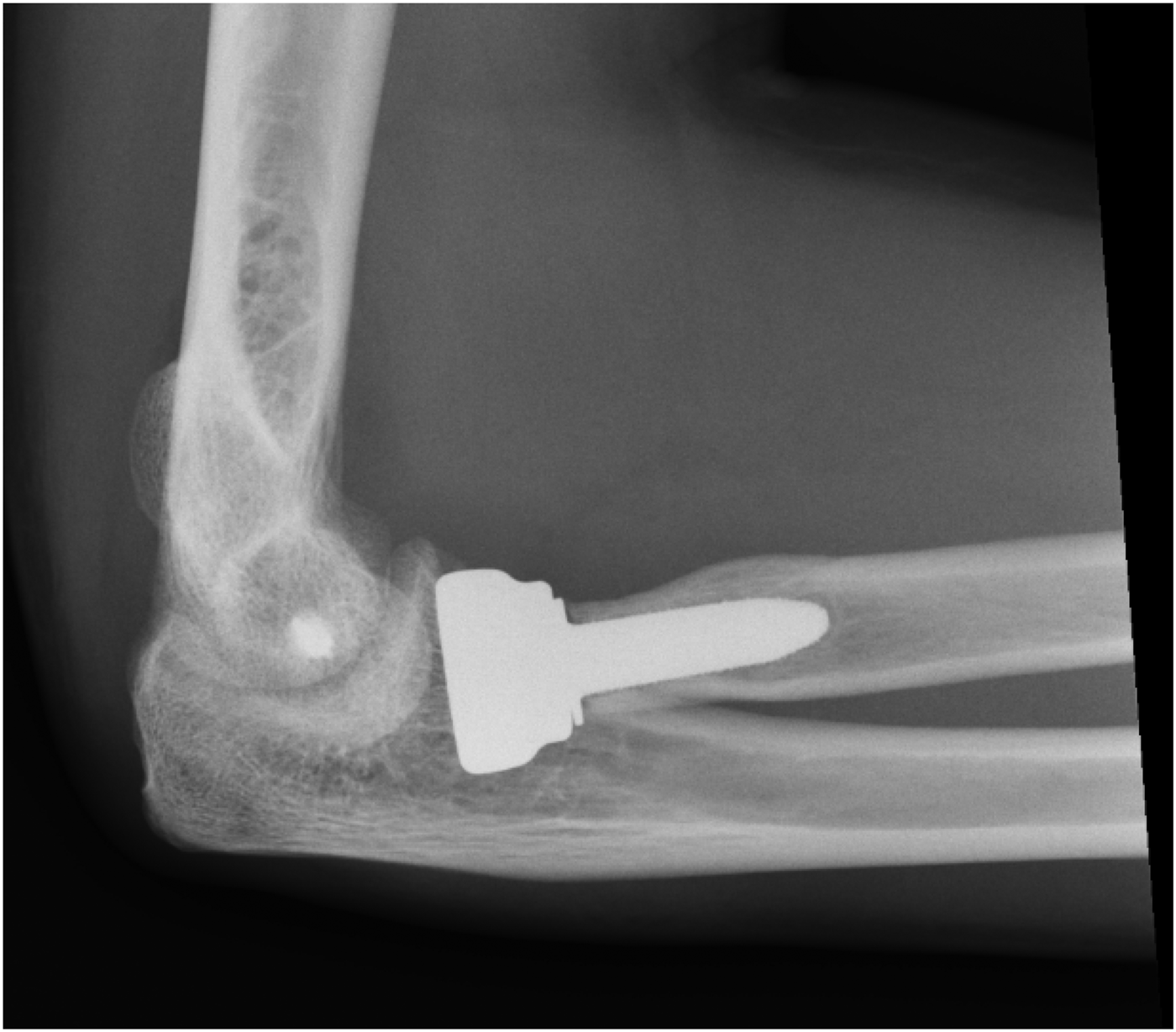
Osteolysis at the tip of the stem.
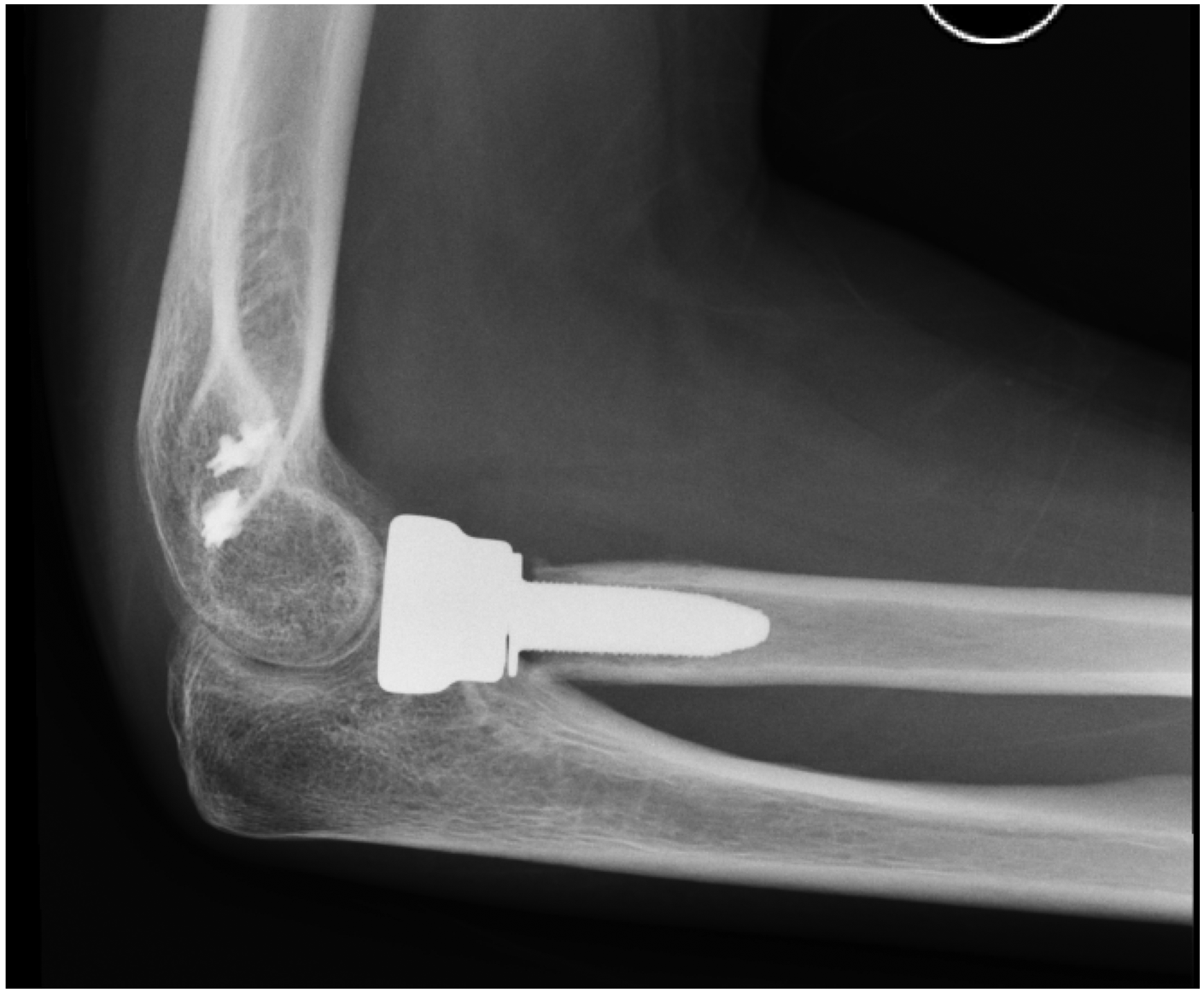
Osteolysis at the proximal part of the stem.

Complete loosening of the stem.
Removal of the prosthesis allowed clear regression of elbow pain, and subsequently three patients reported a pain free elbow with the exception of one patient who complained of mild exertional pain when gardening or snow shovelling. All elbows were stable after removal of the prosthesis and none developed wrist pain. The average ROM in flexion improved from 142° to 148° and the extension deficit decreased from 30° to 16°, which represents a total gain of 20° of motion, and from 78-0-83° to 84-0-94° for pronation/supination, a gain of 15° (Figures 5 and 6).

Evolution of the arc of motion in flexion/extension in the six patients.

Evolution of the arc of motion in pronation/supination in the six patients.
Discussion
Complex fractures of the RH are frequent among young and active patients and so are a therapeutic challenge because osteosynthesis has a poor result in Mason III or IV fractures. 5 The two main treatment options for complex fractures are removal of the head or RHA. Removal of the RH leads to decreased strength and function. 22 Moreover, symptomatic proximal translation of the radius23–26 and generalized instability are seen with associated ligamentous injuries.27,28 The implantation of a RHA aims to remedy these shortcomings by restoring a functional, pain-free and stable elbow while avoiding failure of the implant. However, systematic reviews and meta-analyses have found that RHA has a failure rate at four years of 0–29% 10 and loosening has been observed in up to two thirds of the revisions.29,30 Therefore, the ideal design for an RHA is an on-going debate. Some surgeons recommend the use of a monopolar prosthesis, focusing on its superior ability to restore stability,31,32 while others recommend bipolar or intentionally loose stem prosthesis insertion because of their propensity to diminish the radio-capitellar stress related to their self-centring capacity. 33 Anatomic designs appear to be biomechanically superior,34,35 but also less forgiving, rendering their use controversial.36,37 When considering press-fit stems, long stems appear to perform better than short ones.38,39 However, findings from systematic reviews and meta-analyses are inconclusive. One meta-analysis found no difference between different designs in terms of revision rate, 40 while another found an increased risk of revision among cemented and press-fit stems but no difference in terms of functional outcomes. 41
At our centre, we used the DePuy Synthes Radial Head Prosthesis System™ to treat complex RH fractures in six patients. During patient follow up, osteolysis around the stem was noted in 83% of the cases and subsequent stem loosening occurred 6–12 months post-surgery. The reasons behind the early failure of this prosthesis are unclear. Osteolysis following arthroplasty is a known complication, and accounts for up to 75% of revisions in hip arthroplasty 42 and 30% of RHA. 43 Several causes have been suggested among which polyethylene wear, metal on metal reactions (i.e., aseptic lymphocyte-dominant vasculitis-associated lesion [ALVAL]) or modular neck prosthesis are the most common. 44 Among these complications, only one (i.e., modular neck design) was associated with the DePuy Synthes Radial Head Prosthesis SystemTM. However, most of the aforementioned causes take several years to develop. While a reaction to the implant metals (i.e., cobalt, chrome or titanium) could have been the cause, it is highly unlikely because these metals are commonly used for prostheses.
Early loosening suggests a failure of osteointegration. This prosthesis was designed to be press-fit in the radius for primary stability and to undergo bony ongrowth for secondary stability, a process that unfortunately failed. Non-integration has been reported to be caused by micro-motion at the prosthesis/bone interface, which results in the formation of fibrous tissue.45–47 A recognized cause of micro-motion is insufficient primary stability that can occur when an undersized stem has been used in the medullary canal. In the proximal radius, adequate press-fit creates an optimal stem/bone interface but this has been demonstrated to be close to the fracture threshold. 48 This can lead to apprehension by the surgeon of producing an intra operative fracture and may influence the selection of a slightly thinner stem than the optimal one. Importantly, a direct link between the ratio of stem within the canal to the total length of the RHA and primary stability has been reported. 38 This was confirmed by a retrospective study that found a lower loosening rate of longer stems when short vs long press-fit stems were compared. 39
Suboptimal design of the prosthesis leading to an increase in constraint level, has also been reported to cause micro-motion. 49 Non-physiological tracking of the RHA during elbow motion can cause increased levels of constraint. For example, native RHs are slightly elliptical,50–52 have an eccentric fovea radialis and an offset between the neck and the head. An RHA with a perfectly round head and centred concavity has been shown to be non-anatomical and prone to create a stress zone. 53 The lack of a compensatory mechanism can create eccentric loading of the RHA and varus/valgus constraint along the stem during pronation/supination (Figure 7). Varus/valgus stress on the prosthesis has been shown to create peak micro-motion at the bone/implant interface even under low axial loading conditions.48,54 Indeed, loosening of press-fit RHAs has been reported to create severe osteolysis of greater magnitude than caused by intentionally loose stems.55,56 One possible explanation for this could be carving of the medullar canal by the roughened surface of the loose stem after primary stability is lost and secondary stability has failed.

Toggling of the stem due to mismatch between the capitellar and radial head arthroplasty (RHA) centre of rotation during elbow motion.
Another cause of non-integration is related to the type of surface of the stem.57–61 A grit-blasted chemically etched surface, with a middle roughness, is considered the preferred type. 62 It provides a balance of primary stability and secondary osseointegration. The exact process used for the DePuy Synthes stem was not clearly specified by the manufacturer and so we cannot conclude definitively that this was the reason for its failure.
In summary, the DePuy Synthes Radial Head System™ may have failed because of its amalgamation of a non-anatomic head design with a short press-fit stem. This combination probably imposes high constraints on the stem during elbow motion, facilitating micro-motion at the implant/bone interface, and so preventing osseointegration. Despite the surprisingly high rate of loosening and poor survival of RHA in our case series, restoration of elbow stability was achieved and this permitted the removal of RHA in symptomatic patients. The four patients who had their RHA removed had significant reduction in pain which is consistent with the results of another study that found proximal radial forearm pain to be suggestive of mechanical loosening. 55
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221135881 - Supplemental material for Early aseptic loosening of a press-fit radial head prosthesis – A case series of 6 patients
Supplemental material, sj-pdf-1-imr-10.1177_03000605221135881 for Early aseptic loosening of a press-fit radial head prosthesis – A case series of 6 patients by Corbaz J, Barimani B and Vauclair F in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.