
Abstract
Oesophageal rupture after pneumonectomy is very rare. Management remains a significant challenge. This current case report describes a patient that underwent right pneumonectomy for right central squamous cell carcinoma. On the third day after the operation, food residues were observed in the thoracic tube. Considering oesophageal rupture, surgery was performed. Intraoperative oesophageal rupture was observed and intermittent suture was performed. Unfortunately, an oesophageal pleural fistula developed. Anti-infection treatment, chest drainage, thoracic irrigation, nutrition support and stent implantation were used after the operation. The patient recovered smoothly and had no discomfort when eating. Oesophageal rupture after pneumonectomy is extremely rare and treatment is very difficult. In our opinion, surgical repair is the key to the treatment of oesophageal rupture. Once an oesophageal pleural fistula occurs, enhanced nutrition, adequate irrigation and drainage and stent implantation are critical factors.
Introduction
Causes of oesophageal rupture include trauma, foreign bodies, iatrogenic injury and spontaneous causes. Spontaneous oesophageal rupture, also known as Boerhaave syndrome, refers to a rupture of the whole layer of the wall of the oesophagus caused by nontrauma. 1 It was first reported by Hermann Boerhaave, a Dutch physician, in 1724. 1 The disease is mainly caused by severe vomiting, which is commonly seen after overeating. When vomiting, the annular pharyngeal muscle does not relax, and the oesophageal pressure increases sharply, resulting in oesophageal rupture. 2 Thus, it is also known as vomiting oesophageal rupture. 2 Early diagnosis of oesophageal rupture is delayed due to the lack of clinical manifestations, which may lead to mediastinal pleural contamination, systemic poisoning symptoms, septic shock and high mortality. The treatment difficulty lies in the early evaluation and monitoring of oesophageal rupture. Given that only half of the respiratory tract remains after pneumonectomy, it is more difficult to manage the respiratory tract after oesophageal rupture repair. This current case report describes oesophageal rupture after right pneumonectomy and provides a review the published literature.
Case report
In November 2016, a 66-year-old male patient was admitted to the Department of Cardiothoracic Surgery, Zhejiang University, Lishui Hospital, Lishui Municipal Central Hospital, Lishui, Zhejiang Province, China due to cough for 2 months and sputum with blood for 2 weeks. Chest computed tomography (CT) indicated a central right lung mass (Figure 1). Right central squamous cell carcinoma was confirmed by bronchoscopy. After the exclusion of contraindications, right pneumonectomy and mediastinal lymphadenectomy of the lymph nodes in groups 2, 4, 7, 10, 11 and 12 were performed under general anaesthesia on 14 November 2016. According to the Union for International Cancer Control 2009 lung cancer TNM staging system, the pathological stage was IIIA:T3N1M0. Soft food was given on the first day after surgery. On the third day after the operation, food residues were observed in the thoracic tube. Oesophageal rupture was considered. On 17 November 2016, oesophageal rupture repair was performed under general anaesthesia. During the operation, a 2.5-cm oesophageal rupture was found, which was located under the azygous vein. The food debris was aspirated, the chest cavity was washed and the oesophageal crevasse was sutured with intermittent full-thickness suture. Anti-infection, chest drainage, thoracic irrigation and nutrition support were provided. Oesophagography was performed on 21 December 2016, indicating an oesophagothoracic fistula (Figure 2). Considering that the infection was basically controlled and that the patient's condition tended to be stable, oesophageal stent implantation was performed under gastroscopy on 27 December 2016. On the first day after implantation, 500 ml 10% glucose solution was administered orally. The patient had no discomfort and the dosage was gradually increased. On 6 January 2017, the patient developed choking cough and chest radiography indicated that the stent had moved up. After discussion, another oesophageal stent was replaced under gastroscopy on 7 January 2017. After the second implantation (Figure 3), the patient recovered smoothly and had no discomfort when eating. On 25 October 2017, the patient's chest CT showed right pneumonectomy and oesophageal stent implantation (Figure 4).

Chest computed tomography indicated a central right lung mass (red arrow) in a 66-year-old male patient that presented with a cough for 2 months and sputum with blood for 2 weeks. The colour version of this figure is available at: http://imr.sagepub.com.

Oesophagogram of a 66-year-old male patient that underwent right pneumonectomy for right central squamous cell carcinoma revealed the formation of an oesophagopleural fistula with contrast extravasation (red arrow). The colour version of this figure is available at: http://imr.sagepub.com.
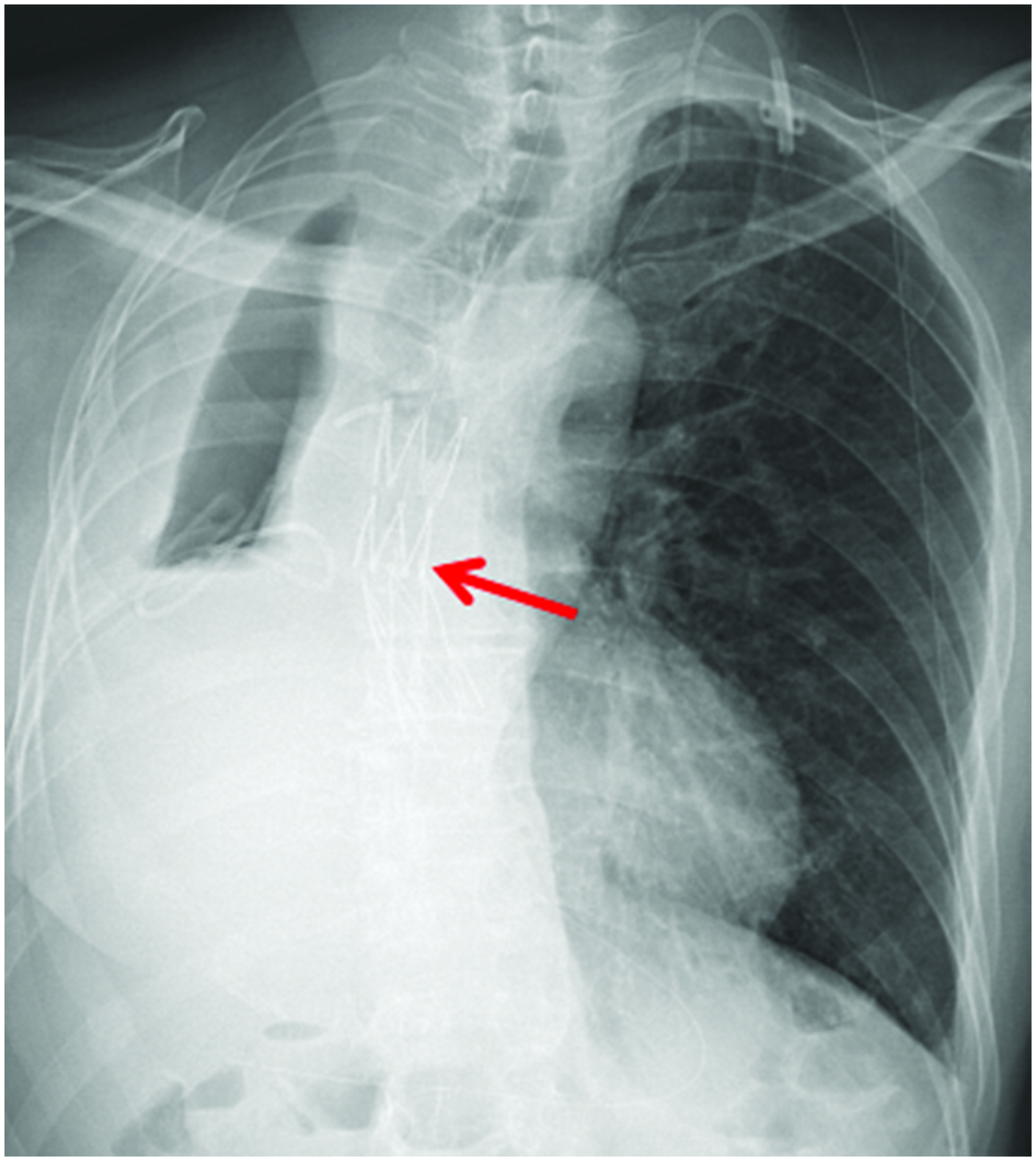
Chest X-ray of a 66-year-old male patient that underwent right pneumonectomy for right central squamous cell carcinoma indicated that the position of the oesophageal stent was good after a second implantation (red arrow). The colour version of this figure is available at: http://imr.sagepub.com.

Chest computed tomography showing right pneumonectomy and oesophageal stent implantation in a 66-year-old male patient that underwent right pneumonectomy for right central squamous cell carcinoma.
The reporting of this study conforms to the CARE guidelines. 3 The publication of this case report and all accompanying images was approved by the Ethics Committee for Clinical Research of Lishui Municipal Central Hospital (no. 2022360). Written informed consent was obtained from the patient for the publication of this case report.
Discussion
Many complications can occur after pneumonectomy, including arrhythmia, respiratory failure, pulmonary oedema and infection. Oesophageal rupture is a very rare complication. The main clinical manifestations are acute chest pain, severe vomiting, persistent fever and food debris drainage from the chest cavity. It is thought that spontaneous oesophageal rupture after pneumonectomy is related to surgery, abscess, inflammation and diverticula. 4 Early oesophageal rupture may be caused by direct damage to the oesophagus during surgery, especially if a tumour is dissected from the wall of the esophagus.5,6 After mediastinal lymphadenectomy, oesophageal rupture or excessive electrocautery can also lead to indirect oesophageal injury.6,7 Advanced oesophageal rupture is usually caused by tumour recurrence or chronic infection.4–6
Surgery for oesophageal rupture following pneumonectomy is challenging and includes tissue adhesives, stent implantation, occlusion and thoracoplasty, and gastrointestinal reconstructive surgery. 4 A previous report described a patient treated with a new surgical technique for spontaneous oesophageal rupture after pneumonectomy. 4 The patient underwent left cervical esophagogastrostomy via a presternal subcutaneous route using thoracic oesophageal mucosal stripping. 4 In this current case, due to total pneumonectomy, the thoracic cavity space was too large to be completely filled with a muscle flap, so oesophageal rupture was repaired intraoperatively. Unfortunately, postoperative oesophageal pleural fistula still occurred. Anti-infection treatments, chest drainage, thoracic irrigation, nutrition support and stent implantation were provided after the operation. The patient recovered smoothly and had no discomfort in eating.
Postoperative management remains a significant challenge. Hypoxia, infection, imbalance of water and electrolytes and surgical trauma are the main causes of postoperative complications. First, the induction of arrhythmia should be eliminated and satisfactory oxygen supply should be maintained. Effective cough sputum, avoiding mediastinum swing, airway humidification, atomization inhalation and back-breaking sputum drainage can effectively promote sputum drainage, improve pulmonary ventilation and avoid pulmonary infection. The infusion speed and infusion volume must be strictly controlled to avoid the occurrence of pulmonary oedema. The current patient's daily intake and outflow volume and urine volume were calculated to maintain a basic balance. Secondly, because of the oesophageal fistula, chest infection cannot be avoided. In addition to antibiotic use according to drug sensitivity tests, adequate drainage and irrigation are also essential. This current case was alternately rinsed with 0.9% sodium chloride and 1% diluted iodophor solution. Thirdly, nutrition is the key factor to ensure fistula healing. Intravenous nutrition was used in the early stage and adequate nutrition was improved by a nasogastric tube or jejunal fistula in the later stage in the current case. Fourthly, stent implantation is particularly important for long-term nonhealing of oesophageal fistula. Over time, stent implantation not only blocks infection but also improves the likelihood of fistula healing. Fifthly, postoperative pain is an important factor that causes arrhythmia and exacerbation of pulmonary infection. Timely and effective analgesia, including postoperative analgesic pumps and intravenous analgesics, should be used to reduce pain, relieve psychological pressure, ease mood and relieve anxiety. Therefore, timely surgical intervention and specialized care should be used to help patients safely survive the crisis. The clinical manifestations of spontaneous oesophageal rupture should be fully understood. Timely detection and early intervention should be performed, and an individualized and refined whole-course nursing plan should be formulated to avoid the occurrence of adverse events and promote the early recovery of patients.
In conclusion, oesophageal rupture after pneumonectomy is extremely rare with atypical clinical symptoms. If it is not actively treated, the prognosis will be poor and mortality will be very high. This current case report presents a rare case of oesophageal rupture after pneumonectomy, which may provide valuable information for the future management of similar patients. Once it occurs, surgical repair, infection control, effective irrigation and drainage, nutritional support and stent implantation may represent key factors in the treatment of oesophageal rupture.
Supplemental Material
sj-jpg-1-imr-10.1177_03000605221133982 - Supplemental material for Oesophageal rupture after right pneumonectomy: A case report
Supplemental material, sj-jpg-1-imr-10.1177_03000605221133982 for Oesophageal rupture after right pneumonectomy: A case report by Jianmin Lv, Fangbiao Zhang, Shaosong Tu and Yan Wu in Journal of International Medical Research
Footnotes
Acknowledgement
We would like to acknowledge the patient for allowing this case report to be published.
Author contributions
J.M.L. and F.B.Z. drafted the manuscript. S.S.T., F.B.Z. and J.M.L. performed the surgery. Y.W. collected and analysed the clinical and physiological data. Y.W. and F.B.Z. performed critical revisions of the manuscript for important intellectual content. J.M.L. and Y.W. edited the manuscript. J.M.L., F.B.Z., S.S.T. and Y.W. reviewed the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.