
Abstract
Haematological diseases with pancreatic masses as the first symptom are clinically rare but should not be ignored. This case report describes a 60-year-old female patient with acute leukaemia that had a pancreatic mass as her first symptom. The patient was admitted and elastography combined with endoscopic ultrasound (EUS) guided fine needle aspiration biopsy (EUS-FNA) was used for diagnosis, treatment planning and determination of prognosis. The site selected for the EUS-FNA puncture was the caudal section of the pancreatic body and the posterior wall of the gastric body was used as the puncture point. The elastography view of the head of the pancreas was blue/green with predominant blue colour. A 19 G puncture needle with a slow-draw core and two stitches of micro-negative pressure were used. Cytology detected heterotypic cells, pancreatic puncture histopathology, the presence of pancreatic alveolar structures and heterotypic tumour cells in the interstitium. Immunohistochemistry of the pancreatic puncture tissue showed B-cell lymphoblast-derived tumours and bone marrow puncture indicated acute lymphoblastic leukaemia. The patient was diagnosed with acute lymphoblastic leukaemia invading the pancreas and was treated with chemotherapy. After treatment, her condition was stable. Follow-up is ongoing and there have been no signs of tumour recurrence or metastasis.
Introduction
Haematological cancers with pancreatic masses as the first symptom are rare in clinical practice.1,2Careful clinical attention should be paid when the mass is in the pancreas. Elastography combined with endoscopic ultrasound (EUS) guided fine needle aspiration biopsy (EUS-FNA) can be used to diagnose and obtain histopathology to guide diagnosis and treatment.3,4 The present case report describes a female patient that presented with abdominal pain as her main symptom. EUS played a key role in the diagnosis and treatment of this current case. In particular, the pathology obtained by EUS-FNA played a decisive role in the patient’s subsequent diagnosis of acute lymphoblastic leukaemia.
Case report
On 9 December 2020, a 60-year-old female patient was admitted to the Department of Gastroenterology, Binzhou Medical University Hospital, Binzhou, Shandong Province, China due to epigastric pain over the previous month. The abdominal pain was mainly localized under the xiphoid process, radiating to the lower back, accompanied by abdominal distension. An abdominal ultrasound examination performed at a local county hospital on 2 December 2020 suggested that the body of the pancreas was caudally occupied. Past, personal and family history were not specific. Her vital signs were normal. No yellowish staining of the skin or sclera were identified. No palpable enlargement of superficial lymph nodes was noted. Heart and lung examinations showed no obvious abnormal signs. The abdomen was flat and soft, there was mild tenderness under the xiphoid process with no rebound tenderness, the liver and spleen were not palpable, and Murphy’s sign was negative.
Laboratory tests on admission showed the following: white blood cell (WBC) count 8.2 × 109/l; red blood cell count 4.6 × 1012/l; platelet count 222 × 109/l; neutrophil percentage 55.1%; monocyte percentage 14.6% (normal range, 3–8%); erythrocyte sedimentation rate 50 mm/h. Routine urine and stool sample analyses were both negative. Biochemistry tests showed the following: amylase 390 U/l (normal range, 35–135 U/l); lactate dehydrogenase 346.0 U/l (normal range, 120–250 U/l); α-hydroxybutyrate dehydrogenase 237.0 U/l (normal range, 72–182 U/l). A haemagglutination assay showed the following: carbohydrate antigen (CA)199 (–), carcinoembryonic antigen (–), alpha-fetoprotein (–), CA125 (–), negative for antinuclear antibodies, nine immunity items and immunoglobulin G4. Chest computed tomography (CT) did not show any significant abnormalities. Upper abdominal contrast enhanced CT suggested pancreas fullness with round-like hypo-enhancing foci seen in the head and tail of the pancreas with poorly defined borders. Pancreatic occupancy was therefore considered and magnetic resonance imaging (MRI) was suggested. Upper abdominal MRI with contrast enhancement and magnetic resonance cholangiopancreatography showed hypo-enhancing irregular soft tissue masses in the head and tail of the pancreas with poorly defined borders (Figure 1). The common bile duct and pancreatic duct were dilated. The common bile duct was narrowed at the end and dilated above it with the pancreatic duct being slightly dilated. The imaging department reported that autoimmune inflammation was not excluded and recommended to combine these results with clinical signs. The patient’s diagnosis was unclear at this stage. Patient consent to treatment was obtained.
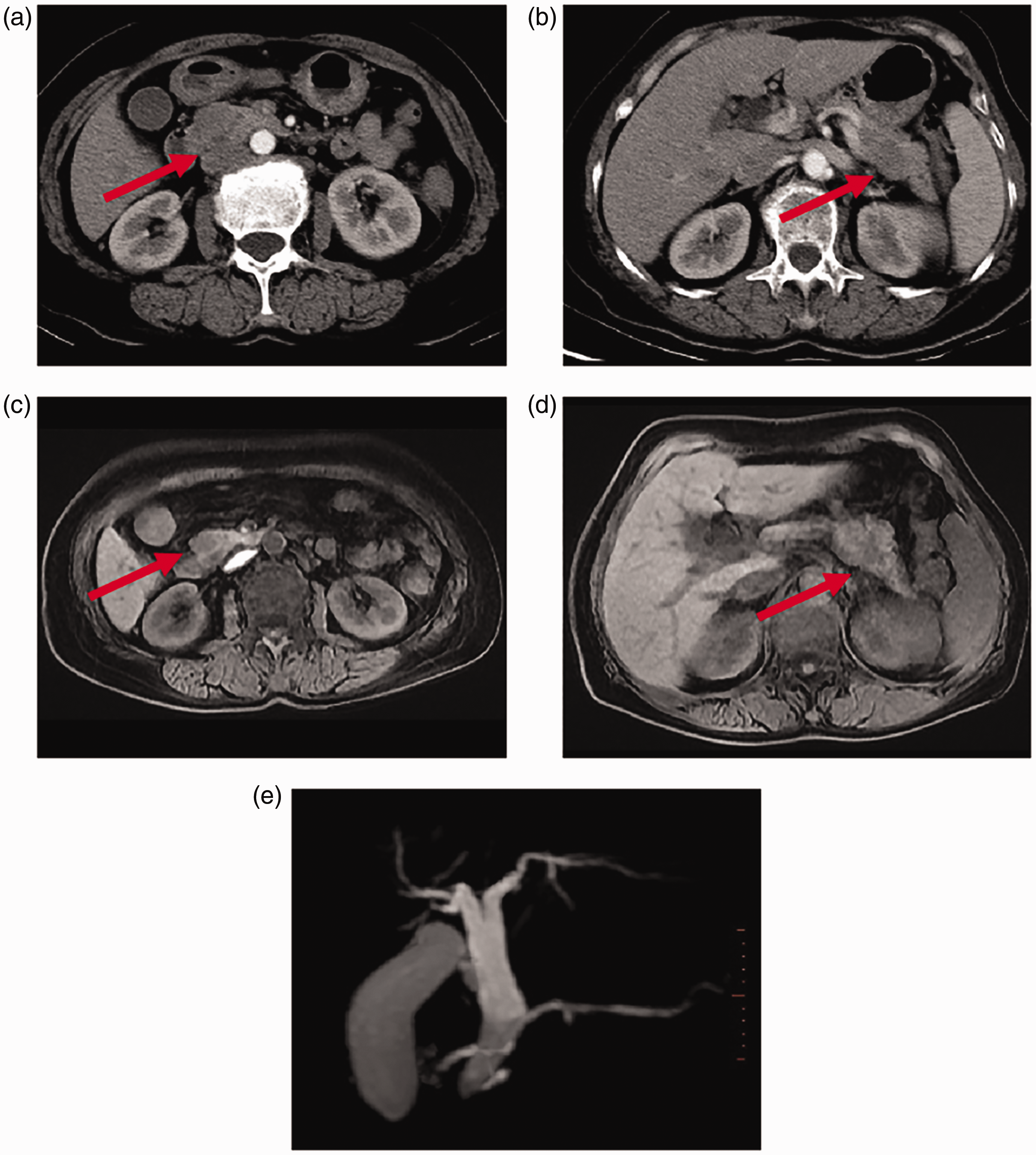
Representative images of a 60-year-old female patient that presented with epigastric pain for 1 month: (a & b) computed tomography (CT) of the head and body of the pancreas were markedly enlarged, and an irregular soft tissue mass was seen with hypo-enhancement (red arrows) in enhancement III; (c & d) CT of the head and tail of the pancreas were markedly enlarged and an irregular soft tissue mass with hypo-enhancement and poorly defined borders was seen (red arrows) and (e) magnetic resonance cholangiopancreatography showed a dilated common bile duct and pancreatic duct, narrowed end of the common bile duct, dilated middle and upper segments, and a slightly dilated pancreatic duct. The colour version of this figure is available at: http://imr.sagepub.com.
To clarify the diagnosis, EUS and EUS-FNA were performed (Figure 2). These investigations found that the pancreas was enlarged in volume and hypoechoic changes were seen in the head and tail of the pancreas with poorly defined borders. The bile duct and pancreatic duct were also dilated, and the end of the common bile duct was slightly narrowed. No significant abnormalities were seen in the walls of the bile duct or gallbladder. The site of puncture was chosen as the caudal part of the pancreatic body and the posterior wall of the gastric body was used as the puncture point. A Cook 19 G puncture needle with a slow-draw core and two stitches of micro-negative pressure were used to obtain satisfactory tissue strips (Figure 3). There was no bleeding from trauma after the puncture and no discomfort reported during or after the puncture. Post-puncture cytology detected heterotypic lymphocytes and pancreatic puncture histopathology suggested the presence of pancreatic alveolar structure. Heterotypic tumour cells were also seen in the interstitium (Figure 4). Concurrent immunohistochemistry results were as follows: cluster of differentiation (CD)20 (+), CD79a (+), Pax-5 (+), CD10 (+), Bcl-2 (+), c-myc (+), MUM-1 (–), p53 (+), CD30 (–), CD21 (–), CD23 (–), cyclin D1 (–), CD3 (–), CD5 (–), CD43 (+), Ki-67 (+), cytokeratin (CK) (–) and EBER (–), indicating a B-cell lymphoblast-derived tumour (Figures 5 and 6). A hospital-wide multidisciplinary consultation was organized, with additional immunohistochemistry for terminal deoxynucleotidyl transferase (TdT), CD34, and CD99 being recommended, and haematology-related indexes were reviewed. Routine blood tests showed a WBC count of 41.1 × 109/l and a platelet count of 80 × 109/l. Moreover, lymphocytes and monocytes could not be detected, resulting in the patient being referred to the Department of Haematology, Binzhou Medical University Hospital, Binzhou, Shandong Province, China. Bone marrow aspiration revealed obvious bone marrow hyperplasia and prolymphocytes of 79% (Figure 7). Bone marrow flow cytometry was consistent with an acute leukaemia immunophenotype. The bone marrow biopsy considered B lymphoblastic leukaemia/lymphoma with a t(9;22)(q34;q11.2) translocation. Bone marrow cell chromosome karyotype analysis showed the following: 46, XX, t(9:22)(q34:q11.2). Additional immunohistochemistry suggested TdT, CD34 and CD99 positivity. Ultimately, the patient was diagnosed with acute lymphoblastic leukaemia (B-cell) invading the pancreas and the patient was given a cycle of the vincristine, daunorubicin, cyclophosphamide and prednisone chemotherapy regimen as follows: 1.5 mg/m2 per day vincristine, once a day, by intravenous (i.v.) drip, on days 1, 8, 15, 22; 30–45 mg/m2 per day daunorubicin, once a day, by i.v. drip, on days 1–3 for the first week; 600 mg/m2 per day cyclophosphamide, once a day, by i.v. drip, on days 1–15; 40–60 mg/m2 per day prednisone, orally, once a day on days 1–14, with a gradual reduction in dose from days 15–28, stopping on day 28. This treatment resulted in significant improvements in blood count, pancreatic occupancy and bone marrow. The patient has now completed five cycles of chemotherapy and is in a stable condition. The reporting of this study conforms to CARE guidelines. 5 All information about the patient come from the Department of Gastroenterology, Binzhou Medical University Hospital. All of the patient details were de-identified. The patient provided written informed consent to publish this case.

Representative endoscopic ultrasound images of a 60-year-old female patient that presented with epigastric pain for 1 month: (a) hypoechoic occupancy with indistinct borders seen in the head of the pancreas (red arrows); (b) elastography view of the head of the pancreas: blue/green with predominant blue colour; (c) caudal pancreatic body was observed with hypoechoic occupancy with indistinct borders (yellow arrows) and (d) caudal pancreatic body elastography: blue/green with predominant blue colour. The colour version of this figure is available at: http://imr.sagepub.com.
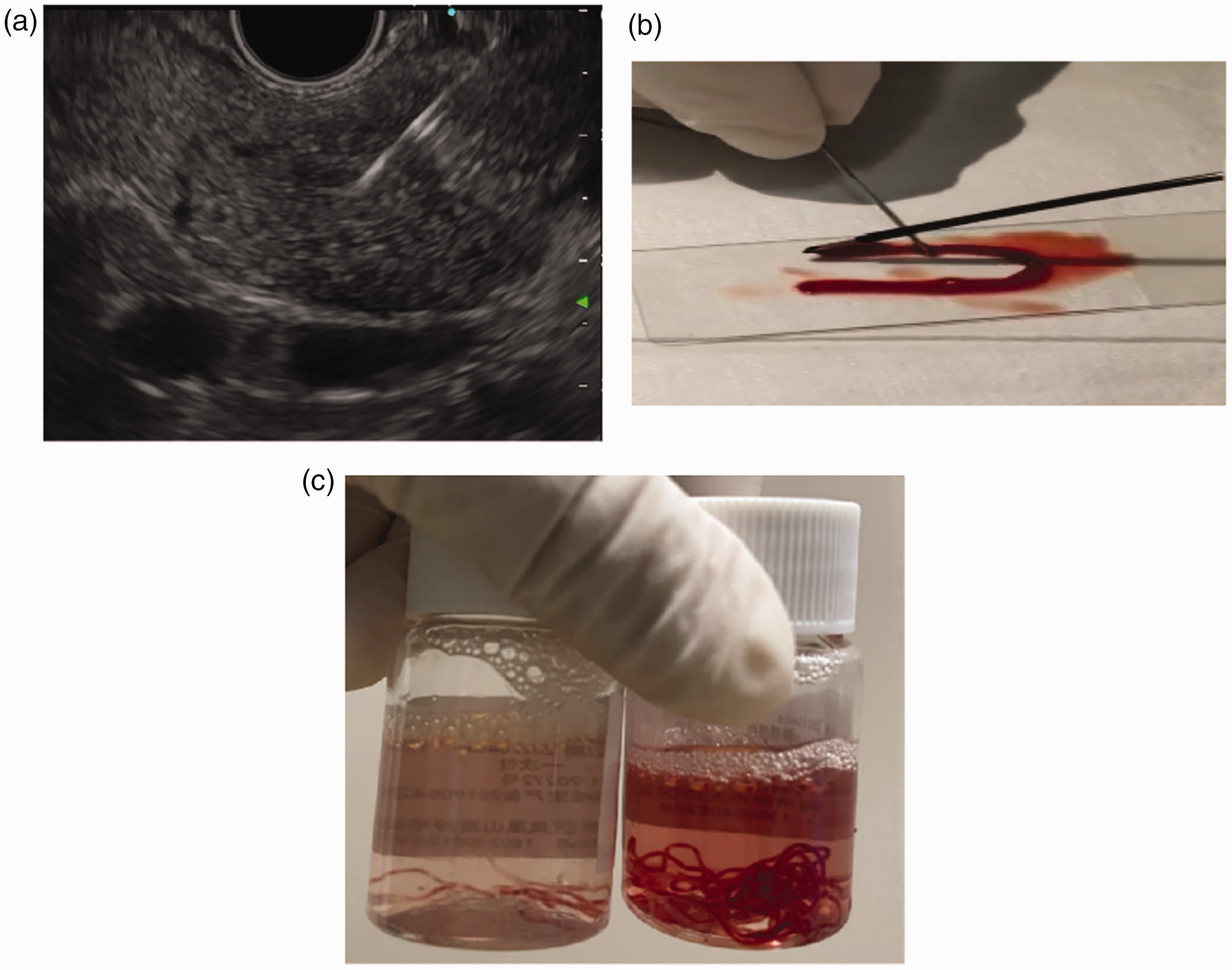
Endoscopic ultrasound images of a 60-year-old female patient that presented with epigastric pain for 1 month showing the 19 G puncture needle in the caudal part of the body of the pancreas (a). (b) Processing the puncture specimen and (c) The puncture specimen. The colour version of this figure is available at: http://imr.sagepub.com.

Representative photomicrographs of biopsy samples from of a 60-year-old female patient that presented with epigastric pain for 1 month showing heterotypic cells within the pancreatic tissue (yellow arrows) (haematoxylin and eosin, scale bar 100 µm) (a). Pancreatic puncture histopathology suggested the presence of pancreatic alveolar structures (yellow arrows) and heterotypic tumour cells were seen in the interstitium (haematoxylin and eosin, scale bar 100 µm) (b). The colour version of this figure is available at: http://imr.sagepub.com.

Representative photomicrographs of the immunohistochemical analysis of pancreatic puncture samples from of a 60-year-old female patient that presented with epigastric pain for 1 month showing the results for cluster of differentiation (CD)20, Pax-5, CD34 and terminal deoxynucleotidyl transferase (TdT) (scale bar 100 µm). The colour version of this figure is available at: http://imr.sagepub.com.

Representative photomicrographs of the immunohistochemical analysis of pancreatic puncture samples from of a 60-year-old female patient that presented with epigastric pain for 1 month showing the results for cytokeratin (CK), cluster of differentiation (CD)3, CD5 and Ki-67 (scale bar 100 µm). The colour version of this figure is available at: http://imr.sagepub.com.

Bone marrow aspiration from of a 60-year-old female patient that presented with epigastric pain for 1 month suggested markedly active myeloproliferation and a bone marrow biopsy suggested leukaemia. Prolymphocytes accounted for 79% of cells (haematoxylin and eosin, magnification × 1000). The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
A previous retrospective analysis of 157 patients with surgical resection of the pancreas between 1965 and 2012 found that 42 of these cases were associated with haematological lesions, of which 27 (64%) were clinically suspected of haematological origins; and of the remaining 15, four cases were misdiagnosed and underwent radical resection of pancreatic cancer. 6 The most common type of haematological disease that involved the pancreas in this study was diffuse large B-cell lymphoma, followed by follicular lymphoma, and then granulocytic leukaemia. 6 Further, acute lymphoblastic leukaemia (ALL) involving the pancreas did not appear in this previous study. 6 Haematological malignancies can involve the pancreas, but in rare cases, they can present as an isolated pancreatic mass.1,2 The acinar defect in Shwachman-Diamond Syndrome may be generalized to pancreatic and parotid glands. 7 The pancreas is an uncommon site to be involved. There has been a report in the literature of a case of pancreatic myeloid sarcoma presenting with symptoms of acute pancreatitis including epigastric pain associated with nausea and vomiting, with imaging findings (abdominal CT) suggestive of pancreatic carcinoma, both presenting as hypoattenuating mass. 8 Marrow dysfunction in the setting of other causes of pancreatic dysfunction, such as Pearson marrow-pancreas syndrome or cystic fibrosis, should be considered. A recent analysis of 1514 patients transplanted for Shwachman-Diamond Syndrome demonstrated 4% of young adults harboured compound heterozygote mutations in the Shwachman-Diamond Syndrome gene with concurrent TP53 gene mutations and a poor prognosis. 9 Regarding prognostic factors for ALL outcome, age at diagnosis (>35 years) is an important factor in B-ALL. 10 In addition, white blood cell counts (>30,000/μl), the presence of the t(9;22) or t(4;11) translocations, and therapeutic response to induction therapy have been reported to be prognostic factors. 11 Of these factors, age >35 years at diagnosis, the presence of the t(9;22) translocation and white blood cell counts >30,000/μl were factors in this reported case.
Pancreatic mass lesions are clinically common and their treatment and prognosis are closely related to the nature of the lesion, which is difficult to characterize with low sensitivity and specificity in conventional imaging diagnosis. 12 Aspiration pathology is particularly important for diagnosis. With the advent of linear array EUS, EUS-FNA can directly obtain pancreatic occupying tissue cells, make pathological diagnoses of pancreatic masses, as well as guiding treatment and assessing prognosis, which greatly improves the diagnoses of pancreatic masses. 13 EUS played a key role in the treatment of this current case. In particular, the pathology obtained by EUS-FNA played a decisive role in the subsequent diagnosis and treatment.