
Abstract
Objective
This study aimed to determine the rate of achieving the target blood pressure (BP) defined by Japanese hypertension management guidelines and to examine factors associated with achieving the target BP.
Methods
This cross-sectional study, which was conducted between January 2012 and December 2015, examined the BP control status and associated factors among 9,016 Japanese community residents with hypertension. Residents were divided into the following six groups: G1, young, middle-aged, and early-phase elderly patients; G2, patients with cerebrovascular disease; G3, patients with coronary artery disease; G4, patients with chronic kidney disease with proteinuria; G5, patients with diabetes; and G6, patients with chronic kidney disease without proteinuria. BP target achievement rates were calculated for each group. A multivariate analysis identified factors associated with “therapeutic failure” of target BP.
Results
The target BP was achieved by 52.6% participants in G1, 84.3% in G2, 50.6% in G3, 45.6% in G4, 48.7% in G5, and 75.0% in G6. The body mass index and receiving antilipidemic medication were associated with therapeutic failure.
Conclusion
This study shows that achievement rates for treatment goals among Japanese patients with hypertension are still low. Body mass index and treatment of dyslipidemia may be associated with the control of BP.
Introduction
Hypertension is a major cause of cardiovascular events and a public health burden in developed and developing countries.1–6 The prevalence of a high blood pressure (BP) ranges between 30% and 50% in adults in many populations worldwide. 1 The number of people aged 30 to 79 years with hypertension doubled from 1990 to 2019, from 331 (95% credible interval 306–359) million women and 317 (292–344) million men in 1990 to 626 (584–668) million women and 652 (604—698) million men in 2019, despite a stable global age-standardized prevalence. 1 Approximately 54% of stroke and 47% of ischemic heart disease cases worldwide are attributable to a high BP. In addition, 7.6 million premature deaths (approximately 13.5% of the global total) and 92 million disability-adjusted life years (6.0% of the global total) worldwide have been attributed to a high BP. 5
Several decades previously, cerebrovascular disorders were the leading causes of hypertension-associated death in Japan, and death due to cerebrovascular disorders was markedly higher in the northern territory of Japan than in other territories. 7 In recent years, BP measurements among the Japanese general population have decreased because of a reduction of salt intake among other reasons. Nevertheless, an estimated 43 million Japanese people have hypertension, and the treatment target BP (<130/80 mmHg) achievement rate is only approximately 30%.7–9 Therefore, hypertension remains an important risk factor for cardiovascular diseases and poses a major public health challenge in Japan, as in other countries in other parts of the world. 7
A major earthquake (Great East Japan Earthquake), which spawned a devastating tsunami, damaged vast areas of the northeastern coast of Japan on 11 March 2011.10–12 Imbalanced nutrition, 11 and a lack of daily activities negatively affected people affected by the earthquake.10,11 To restore medical services and the health of residents in the affected regions of Miyagi and Iwate Prefectures, the Tohoku Medical Megabank (TMM) Project was established. The TMM Project was administered in these two prefectures by the Tohoku Medical Megabank Organization (ToMMo) and by the Iwate Tohoku Medical Megabank Organization. The ToMMo was established at Tohoku University in Miyagi Prefecture, and the Iwate Tohoku Medical Megabank Organization was established at Iwate Medical University in Iwate Prefecture. 12 Although several studies have examined health care services among residents in the affected areas, few studies have examined the achievement rates of target BP among affected residents with hypertension after the major earthquake in the areas.
This study aimed to determine the rate of target BP achievement and examine factors associated with achievement failure among Japanese community residents with hypertension who reside in areas affected by the Great East Japan Earthquake and tsunami.
Subjects and methods
Participants
Details regarding the TMM Project were previously reported. 12 This was a cross-sectional study that screened 66,874 Japanese community residents who underwent a voluntary health checkup conducted by the ToMMo between January 2012 and December 2015 in Miyagi and Iwate Prefectures, Japan. A total of 17,115 of study participants were receiving treatment with medication for hypertension, and 8099 were excluded owing to data missing for categorization.
Variables
Height, weight, body mass index (BMI), and waist circumference were measured with participants in the standing position. The BMI was calculated by dividing body weight (kg) by height in meters squared (m2). Mean systolic BP and diastolic BP were measured at the upper arm by a trained nurse in participants who had been seated for at least 5 minutes The HEM-9000AI electronic upper arm-cuff device (OMRON Corporation, Kyoto, Japan) was used for BP measurements. Blood pressure was measured once, and we used the first blood pressure measurements in the analysis.
The details of blood and urine sample collection and measurement of these samples were already described in a previous report. 13 The amount of blood collected was usually 34 mL. The measured blood consisted of 7 mL in an EDTA2Na blood tube, 5 mL in a sodium heparin blood tube, and two serum blood tubes containing 9 mL of blood for completing blood count tests (2 mL) and for a blood sugar or hemoglobin A1c (HbA1c) test (2 mL). With regard to urine collection, urine samples that were left over after measurements for specific health checkups were stored in urine centrifuge tubes. Serum concentrations of total cholesterol (TC; Ultra Violet-End method using cholesterol dehydrogenase), high-density lipoprotein cholesterol (HDL-C; direct method), low-density lipoprotein cholesterol (LDL-C), and triglycerides (enzymatic method) were also measured. LDL-C concentrations were estimated using the Friedewald equation ([TC] – [HDL-C] – [TGs/5]) for all participants. 14 HbA1c values were determined by Latex agglutination turbidimetry. Serum creatinine concentrations were measured by the enzymatic method. The estimated glomerular filtration rate (eGFR) was calculated using the Japanese GFR equation: eGFR (mL/minute/1.73 m2) = 194 ×creatinine−1.094 × age−0.287 (×0.739 if female sex). 15 Urine protein was also estimated by quantitative immunoturbidimetry. Proteinuria was estimated qualitatively as “−”, “+/−”, “+”, “++”, and “+++”. Among them, “+”, “++”, and “+++” were defined as proteinuria (positive).
Diabetes mellitus was defined as fasting plasma glucose concentrations ≥6.99 mmol/L or HbA1c values ≥6.5%, use of antidiabetes medications, or already diagnosed diabetes mellitus in accordance with the American Diabetes Association diagnostic criteria. 16 Dyslipidemia was defined as TG concentrations ≥1.69 mmol/L, LDL-C concentrations ≥3.62 mmol/L, HDL-C concentrations <1.03 mmol/L, or the use of antilipidemic medications. 17 Chronic kidney disease (CKD) was defined as an eGFR of <60 mL/minute/1.73 m2.
Participants were asked to complete a self-administered questionnaire that addressed healthy lifestyle characteristics (alcohol consumption and smoking behavior) and present medical history of comorbidities, such as hypertension, diabetes mellitus, dyslipidemia, cardiovascular disease, and cerebrovascular disease. Participants answering that they had any of these comorbidities were registered as having a present medical history from the results of the self-administered questionnaire. Data regarding a family history (hypertension, cardiovascular disease, and cerebrovascular disease) were also collected from the self-administered questionnaire.
Statistical analysis
The results are presented as the mean ± standard deviation (SD) for continuous variables or prevalence (%) for categorical variables. The participants were divided into six groups according to categories of the 2019 version of the Japanese Society of Hypertension Guidelines for Management of Hypertension (JSH2019), and success rates were calculated for each treatment goal as defined by the JSH2019 target values. The groups were as follows: (1) young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD (BP <130/80 mmHg); (2) patients with cerebrovascular disease (BP <140/90 mmHg); (3) patients with coronary artery disease (BP <130/80 mmHg); (4) patients with CKD with proteinuria (BP <130/80 mmHg); (5) patients with diabetes (BP <130/80 mmHg); and (6) patients with CKD without proteinuria (BP <140/90 mmHg). 7 To avoid any overlap between these groups as much as possible, patients with diabetes were selected among the eligible participants. Patients with CKD with proteinuria were then selected from the participants without diabetes mellitus. Following this, patients with coronary artery disease were selected among those without diabetes mellitus and CKD with proteinuria. Patients with cerebrovascular disease were then selected among those without diabetes mellitus, CKD with proteinuria, and coronary artery disease. Patients with CKD without proteinuria were then selected among those without diabetes mellitus, CKD with proteinuria, coronary artery disease, and cerebrovascular disease. Finally, young, middle-aged, and early-phase elderly patients were chosen from those without disease (diabetes mellitus or CKD).
The primary outcome was “therapeutic failure”, which was defined as not achieving the target BP. Achievement rates were calculated for each group.
To estimate the factors associated with therapeutic failure, a multivariate logistic regression analysis was performed using the following models. Model 1 was adjusted for age (years) and sex. Model 2 was adjusted for age (years), sex, alcohol consumption status (daily drinker), smoking behavior (current smoker), HbA1c, LDL cholesterol, triglycerides, and the eGFR. The odds ratio (OR) and 95% confidence interval (CI) were calculated for each item by the multivariate logistic regression analysis. P values were estimated by the two-tailed test, and P < 0.05 was considered statistically significant. All statistical analyses were performed using the Statistical Package for Social Sciences, version 22 (IBM SPSS Inc., Armonk, NY, USA).
This survey was conducted in compliance with the Ethical Guidelines for Epidemiological Studies established by the Japanese Government 18 and in accordance with the Declaration of Helsinki of 1975 (revised in 2000). 19 The research protocol was reviewed and approved by the Ethics Committee of Juntendo University (no. 2020026). The research protocol was also reviewed and approved by the Council of the ToMMo (no. 2019-0079). All participants in this study provided written informed consent.
Results
A total of 9016 eligible participants were included in the present study (men: 6059; women: 2957) (Figure 1). Table 1 shows the basic characteristics of the eligible participants. The mean age (SD) and male sex proportion were 60.5 (11.3) years and 67.2%, respectively. The frequencies of family histories of hypertension, cardiovascular disorders, and cerebrovascular disorders were 38.0%, 9.0%, and 26.4%, respectively.

Study flow chart.
Participants’ characteristics at the baseline survey (n = 9016).
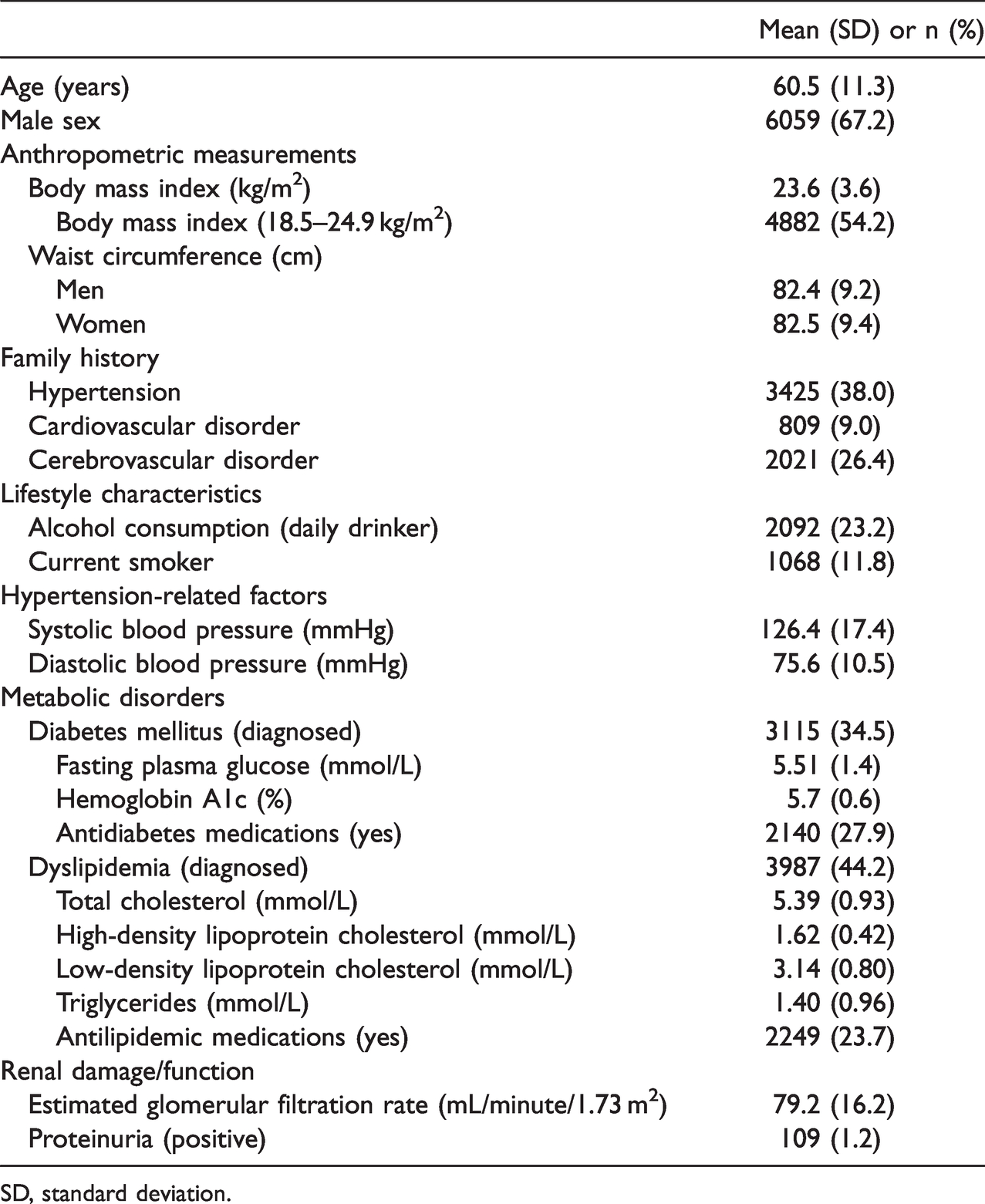
SD, standard deviation.
The mean BMI (SD) was 23.6 (3.6) kg/m2, and the proportion of participants with the ideal BMI (18.5–24.9 kg/m2) was 54.2%. The mean (SD) systolic BP and diastolic BP were 126.4 (17.4) and 75.6 (10.5) mmHg, respectively. The proportions of those who were treated with antidiabetic and antilipidemic medications were 27.9% and 23.7%, respectively.
Table 2 shows the mean BP and achievement rates for the target BP in each category. Among the groups of young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD, patients with coronary artery disease, patients with CKD and proteinuria, and patients with diabetes, the achievement rates were 52.6%, 50.6%, 45.6%, and 48.7%, respectively. Among the patients with cerebrovascular disease and those with CKD without proteinuria, the achievements rates were 84.3% and 75.0%, respectively.
Mean blood pressure and the rate of achieving the target blood pressure (n = 9016).

SD, standard deviation.
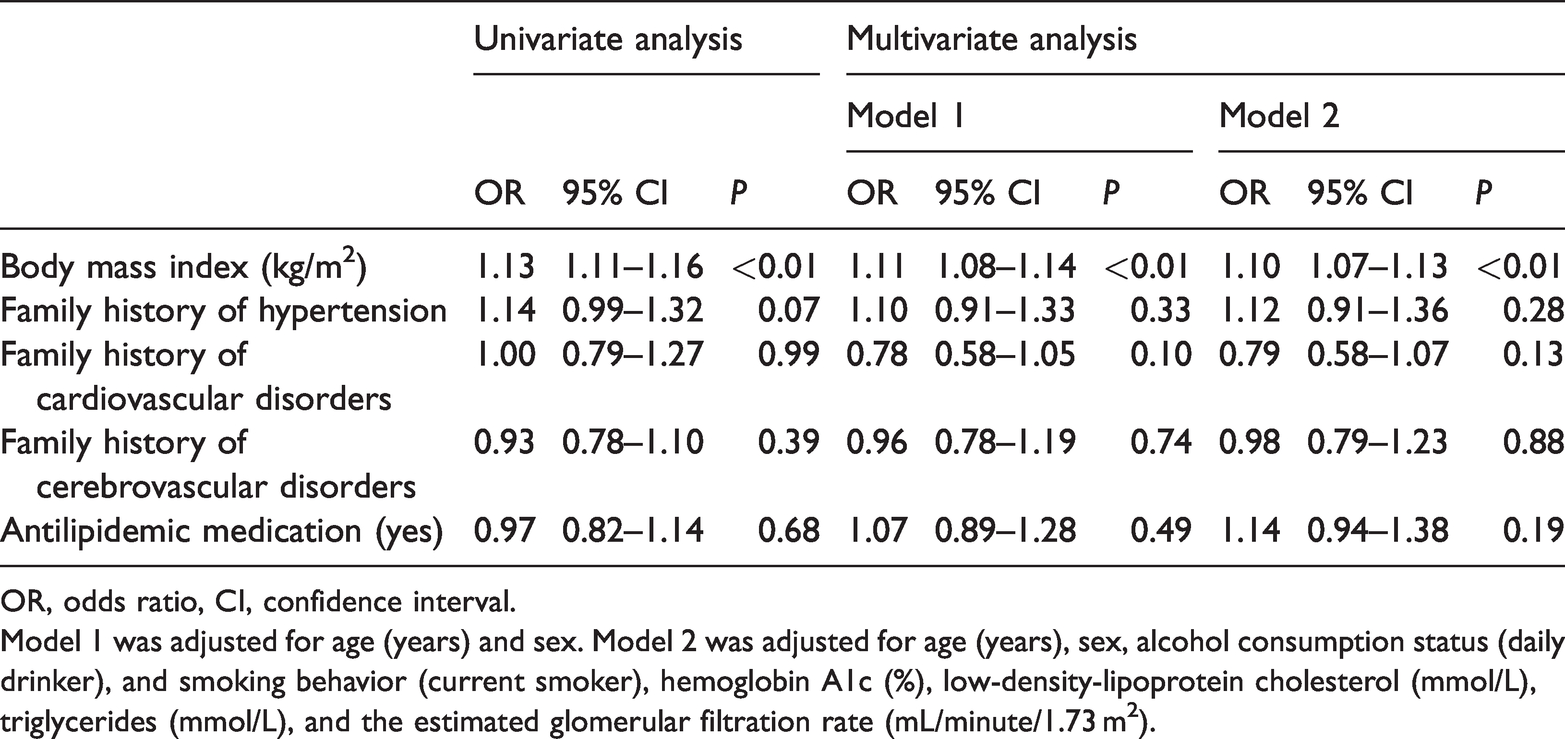
The results of logistic regression analyses are shown in Tables 3–8. The multivariate analysis showed that BMI was significantly associated with a failure to achieve treatment goals in the young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD group (AOR [adjusted odds ratio] = 1.14, 95% CI = 1.11–1.16, P < 0.01) (Table 3), patients with coronary artery disease group (AOR = 1.15, 95% CI = 1.08–1.23, P < 0.01) (Table 5), and patients with diabetes group (AOR = 1.10, 95% CI=1.07–1.13, P < 0.01) (Table 7). In addition, an inverse association between achievement failure and receiving antilipidemic medication was observed in the young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD group (AOR = 0.83, 95% CI = 0.71–0.97, P = 0.02) (Table 3). There were no significant associations of a failure to achieve treatment goals with BMI, a family history of hypertension, cardiovascular disorders, or cerebrovascular disorders, or use of antilipidemic medication in the patients with cerebrovascular disease and patients with chronic kidney disease and proteinuria groups (Tables 4 and 6).
Factors associated with therapeutic failure in young, middle-aged, and early-phase elderly patients without diabetes mellitus or chronic kidney disease (n = 4311).

OR, odds ratio, CI, confidence interval.
Model 1 was adjusted for age (years) and sex. Model 2 was adjusted for age (years), sex, alcohol consumption status (daily drinker), smoking behavior (current smoker), hemoglobin A1c (%), low-density-lipoprotein cholesterol (mmol/L), triglycerides (mmol/L), and the estimated glomerular filtration rate (mL/minute/1.73 m2).
Factors associated with therapeutic failure in patients with cerebrovascular disease (n = 230).
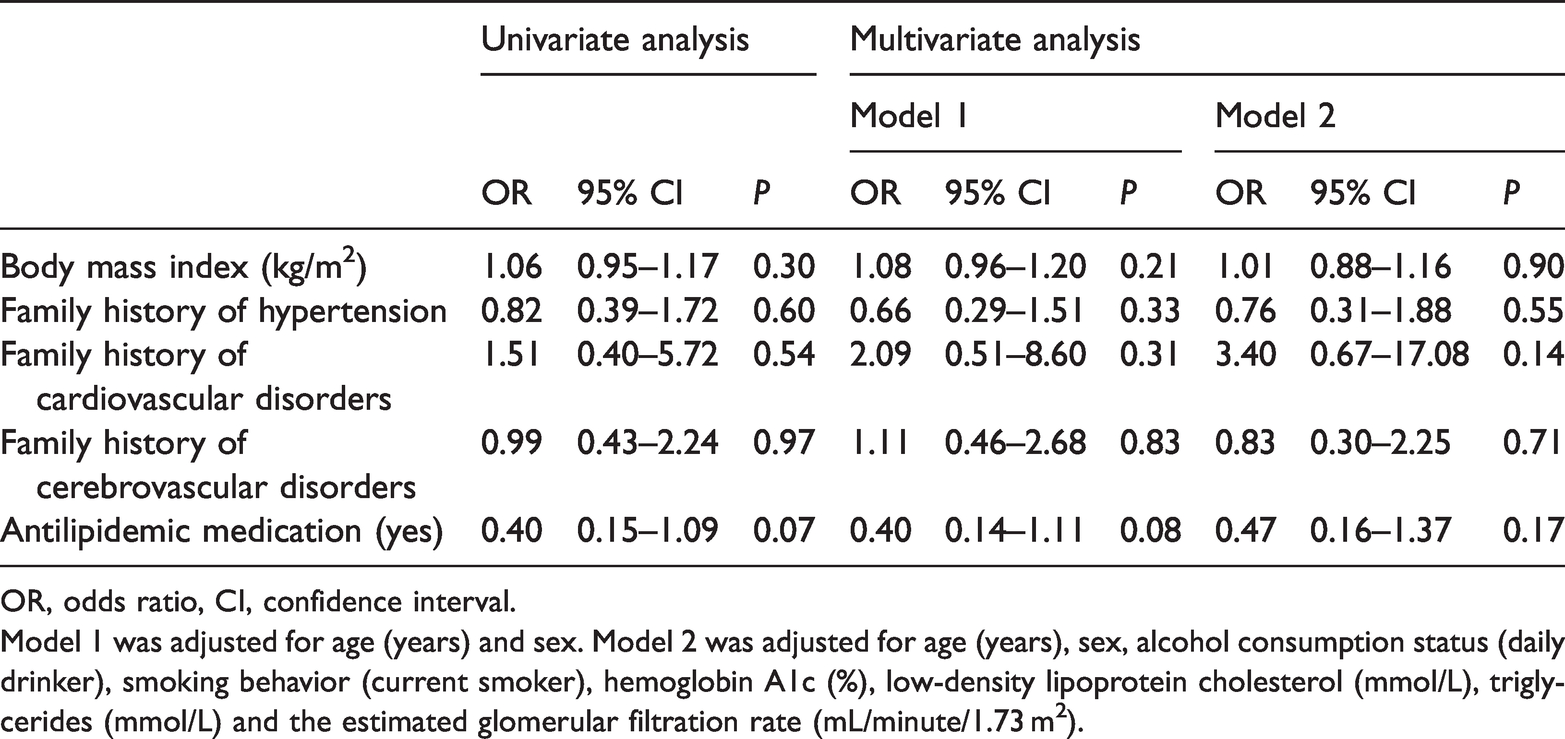
OR, odds ratio, CI, confidence interval.
Model 1 was adjusted for age (years) and sex. Model 2 was adjusted for age (years), sex, alcohol consumption status (daily drinker), smoking behavior (current smoker), hemoglobin A1c (%), low-density lipoprotein cholesterol (mmol/L), triglycerides (mmol/L) and the estimated glomerular filtration rate (mL/minute/1.73 m2).
Factors associated with therapeutic failure in patients with coronary artery disease (n = 872).
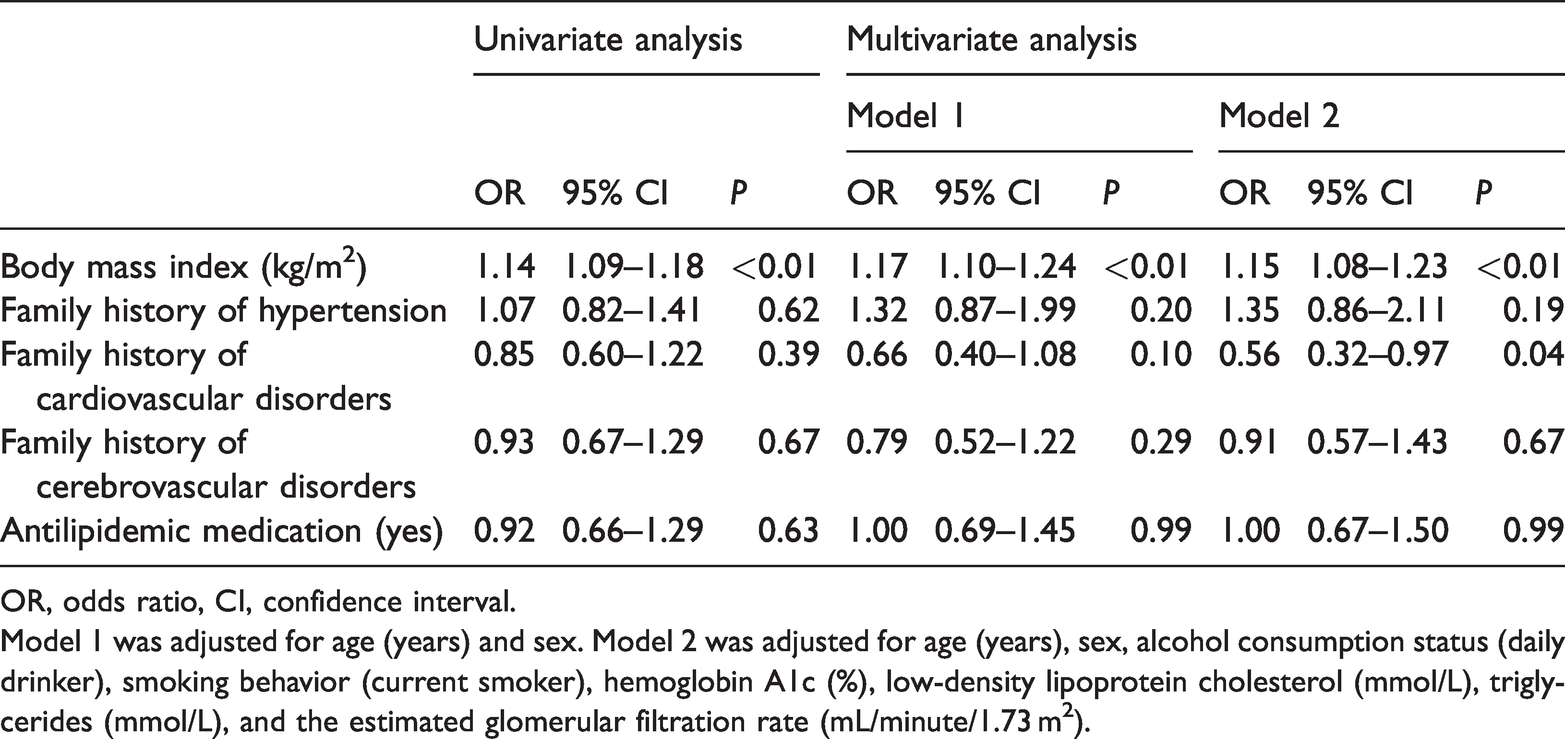
OR, odds ratio, CI, confidence interval.
Model 1 was adjusted for age (years) and sex. Model 2 was adjusted for age (years), sex, alcohol consumption status (daily drinker), smoking behavior (current smoker), hemoglobin A1c (%), low-density lipoprotein cholesterol (mmol/L), triglycerides (mmol/L), and the estimated glomerular filtration rate (mL/minute/1.73 m2).
Factors associated with therapeutic failure in patients with chronic kidney disease and proteinuria (n = 68).
OR, odds ratio, CI, confidence interval.
Model 1 was adjusted for age (years) and sex. Model 2 was adjusted for age (years), sex, alcohol consumption status (daily drinker), smoking behavior (current smoker), hemoglobin A1c (%), low-density lipoprotein cholesterol (mmol/L), triglycerides (mmol/L), and the estimated glomerular filtration rate (mL/minute/1.73 m2).
Factors associated with therapeutic failure in patients with diabetes (n = 3115).

OR, odds ratio, CI, confidence interval.
Model 1 was adjusted for age (years) and sex. Model 2 was adjusted for age (years), sex, alcohol consumption status (daily drinker), and smoking behavior (current smoker), hemoglobin A1c (%), low-density-lipoprotein cholesterol (mmol/L), triglycerides (mmol/L), and the estimated glomerular filtration rate (mL/minute/1.73 m2).
Factors associated with therapeutic failure in patients with chronic kidney disease without proteinuria (n = 420).

OR, odds ratio, CI, confidence interval.
Model 1 was adjusted for age (years) and sex. Model 2 was adjusted for age (years), sex, alcohol consumption status (daily drinker), smoking behavior (current smoker), hemoglobin A1c (%), low-density lipoprotein cholesterol (mmol/L), triglycerides (mmol/L), and the estimated glomerular filtration rate (mL/minute/1.73 m2).
Discussion
The present cross-sectional study examined data from a large number of community-dwelling residents who underwent a health checkup. The main findings were that the rates of target BP achievement were relatively low (approximately 50%) in young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD, patients with coronary artery disease, patients with CKD and proteinuria, and patients with diabetes. In addition, our data suggested that BMI and receiving antilipidemic medication were associated with therapeutic failure in patients with hypertension.
We found that the achievement rates for the target BP (<130/80 mmHg) still remained low (approximately 50%) in young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD, those with coronary artery disease, and those with diabetes. A previous study, which was conducted before the Great East Japan Earthquake, also reported a low achievement status toward goal blood pressure levels, similar to our results. Fukushima Research of Hypertension, which was a cross-sectional analysis of 3,320 hypertensive patients in Fukushima Prefecture, reported that the success rate was 27% in patients with diabetes mellitus or renal disease (<130/80 mm Hg), 30% in those younger than 65 years (<130/85 mm Hg), and 66% in elderly people without diseases (<140/90 mm Hg). 20 Although our results are not lower than those in this previous report, the achievement rates may be relatively low compared with the recommendation of the treatment guideline. Therefore, possible explanations of the low achievement status for better BP management need to be determined.
The newly published JSH2019 guidelines modified BP targets, especially for young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD. 7 These guidelines emphasized that the BP goal for these hypertensive patients should be <130/80 mmHg. This was emphasized because the incidence of cerebrovascular and coronary artery disease had markedly decreased with well-controlled BP compared with the conventional BP goal of <140/90 mmHg as suggested in the Japanese Hypertension Treatment Guideline 2014 (JSH2014). 7 The different thresholds between 130/80 and 140/90 mmHg may lead to different achievement rates. A large-scale Japanese study that examined 20,153 subjects receiving antihypertensive agents reported that a BP <140/90 was achieved in 66.6% (13,426) of the treated subjects; however, only 30.7% (6,188) achieved a BP <130/80. 21 A European epidemiological survey evaluated the proportion of adult outpatients achieving office BP treatment targets recommended by current (2018, the European Society of Cardiology [ESC] and the European Society of Hypertension [ESH]) rather than previous (2013 ESC/ESH) hypertension guidelines. 22 This previous study reported that BP control was significantly lower in non-diabetic outpatients of all age groups (18–65 years: 13.1% vs. 42.9%, 65–79 years: 25.8% vs. 42.5%, and ≥80 years: 29.1% vs. 66.0%; all P < 0.001). Similar reductions were observed in outpatient with diabetes (18–65 years: 32.7% vs. 14.8%, 65–79 years: 37.3% vs. 24.7%, and ≥80 years: 47.1% vs. 27.9%; all P < 0.001). 22 Although reaching the newly established BP goals may be difficult, BP should be more strictly maintained on the basis of the hypertension treatment guidelines for primary and secondary prevention of atherosclerotic disorders.
Low achievement rates of the target BP were also observed in patients with diabetes mellitus, those with CKD and proteinuria, and those with coronary artery disease. There are several possible explanations for the low achievement rates for reasons other than the different thresholds. First, these patients often have difficulty controlling their BP to the strict target levels. A nationwide, cross-sectional epidemiological survey in Italy enrolled 47,217 volunteers. 23 This Italian study reported that individuals with diabetes had higher rates of hypertension (80% vs. 54.7%, P < 0.001), awareness (85.6% vs. 77.3%, P < 0.001), and treatment (85.8% vs. 76.7%, P < 0.001), but a lower hypertension control rate (36.1% vs. 39.6% according to the 2018 European guidelines, P < 0.001; 25.4% vs. 30.8% according to the 2017 US guidelines, P < 0.001) than individuals without diabetes. A cross-sectional survey that examined 39,525 Italian patients with hypertension who were followed up by general practitioners reported that BP control was inadequate in patients with CKD. 24 In this Italian study, only 44% of patients reached a BP target of <140/90 mmHg and 11% achieved <130/80 mmHg. These findings suggest the necessity of placing more focus on these patients and highlight the importance of aggressive management of the target BP to contribute to primary and secondary prevention. The second potential explanation for the low achievement rate of the target BP is a lower awareness of hypertension guidelines in primary care.25,26 A cross-sectional survey of 1,390 primary care physicians conducted in Spain showed that only 58% of physicians knew the contents of the guideline. 25 However, only 36% were using the guidelines in clinical practice. Additionally, a questionnaire survey of 1,382 randomly selected physicians that was conducted via face-to-face interviews showed that most physicians believed in the usefulness of guidelines, but only 56.9% were actually using a guideline. 26 Although the majority of physicians support the concept of guidelines, recommendations may vary by the degree of acceptance. Therefore, general physicians should be made more aware of treatment goals recommended by relevant guidelines and consider the risk factors for each patient. The third potential explanation for the low achievement rate of the target BP is a low treatment compliance and awareness of the normal range in BP, dietary and exercise recommendations, and smoking cessation.27,28 An observational cross-sectional study, which examined 342 Turkish subjects with hypertension, reported that the number of patients who had achieved their target BP and knew the normal range of blood pressure was significantly higher than those who did not know the normal range of blood pressure. 27 Additionally, treatment compliance was significantly associated with better control of hypertension. Another clinical study reported that smokers were more prevalent in the poorly controlled hypertension group than in the well-controlled hypertension group (P = 0.001). 28 In addition, the number of patients who adhered to dietary and exercise recommendations was greater in the well-controlled hypertension group than in the poorly controlled hypertension group (P < 0.001 for both). Therefore, improvement of compliance, awareness, and lifestyle modification are required for better management of BP.
In the present study, BMI was associated with a failure to achieve treatment goals. Obesity is a classic risk factor for elevated BP and also an important risk factor for several lifestyle-related disorders.29–32 A single-center, prospective, cohort study examined 4,766 individuals with hypertension and reported that BMI was negatively and independently associated with predefined BP goals for all types of BP measurements. 30 A multicenter, randomized, clinical trial examined the efficacy of lifestyle interventions for reducing BP over 3 to 4 years in the intervention group (n = 595) and the usual care control group (n = 596). 31 This trial reported that BP was significantly lower in the intervention group than in the control group at 6, 18, and 36 months. The risk ratio for hypertension in the intervention group was 0.58 (95% CI = 0.36–0.94) at 6 months, 0.78 (95% CI = 0.62–1.00) at 18 months, and 0.81 (95% CI = 0.70–0.95) at 36 months. Therefore, achieving the ideal body weight is necessary to maintain better BP control.
Interestingly, our results indicate that a history of taking dyslipidemia medication was associated with a protective effect against failure to achieve BP treatment goals in the young, middle-aged, and early-phase elderly patients without diabetes mellitus or CKD. While this result appears contradictory, one potential explanation may be the association between BP and the pharmacological effects of dyslipidemia medications, especially statins.33–35 A previous survey evaluated the association between the effects of statins on night-time BP in 5,634 adults. 33 This previous study reported that statin use was independently associated with 24-hour (OR [95% CI]: 1.513 [1.295–1.767]; P < 0.001) and night-time (OR [95% CI]: 1.357 [1.161–1.587]; P < 0.001) BP control recommendations of European guidelines, even after adjustment. A retrospective, observational study of 1,827 consecutive patients with essential hypertension reported that those on statin therapy showed better ambulatory BP control, even after adjustment for confounding factors. 35 In addition, analyses of groups derived from propensity score matching (369 patients in each group) confirmed these results (OR = 1.8 for 24-hour BP control; OR = 1.6 for daytime BP control; OR = .7 for night-time BP control, all P < 0.001). There are several possible explanations for these previous findings. In addition to the well-known effects driven primarily by the statin-mediated reduction in circulating LDL-C concentrations, statin therapy is associated with further vascular benefits, such as reduction in free oxygen radicals and inflammatory cytokines, and an improvement in endothelial function.36,37 Better management of lipid concentrations may also help maintain target BP. Accordingly, comprehensive management including lipid concentrations may be required to ensure better treatment of hypertension.
Our study has several limitations worth noting. First, selection bias may have been present because the participants comprised only those who underwent a voluntary health checkup in Miyagi and Iwate Prefectures, Japan. As such, these participants may have been inherently more aware of health behaviors relative to residents who did not participate in the health checkup. Further analyses involving more diverse cohorts are necessary. Second, some important data were not collected, such as information on details of medications taken for treating hypertension and adherence to treatment. In addition, details of specific medication regarding diabetes mellitus and cardiocerebrovascular disorders were unknown. These medications might have modified the results. Further analyses with collection of the details of these specific medications are necessary. Third, data were collected from 2013 to 2015, but the draft of the JSH2019 was introduced in 2018 and published in 2019. However, despite this lag, the threshold for patients with diabetes mellitus and CKD was similar to that of the JSH2009. Therefore, our results may still be applicable. Further studies examining data collected after 2019 are required for an actual evaluation. Fourth, some lifestyle-related criteria were vague because this information was collected from existing questionnaires. Further studies using a questionnaire focused on lifestyle characteristics are required. Fifth, half of the participants were excluded because of missing data in the study. Our results might have been modified if all participants were analyzed. Further analyses involving all participants are necessary. Sixth, a family history was not associated with failure to achieve the target BP in this study. However, several previous studies have reported an association between a family history and BP control. 38 The family history was collected using a self-administrated questionnaire, and this information might not have been collected accurately. An accurate method of collecting the family history needs to be determined.
Conclusion
This study shows that the rate of achieving BP treatment goals recommended by the treatment guideline in hypertensive patients in our study population in Japan is still low, especially in patients with CKD and diabetes mellitus. Body mass index and treatment of dyslipidemia may be associated with the control of BP. Our data indicate the importance of realizing BP goals. Better management of obesity and dyslipidemia may prevent future cardiovascular disorders by ensuring better BP control.
Footnotes
Acknowledgements
The authors thank all participants who underwent the voluntary medical checkups and the data collection staff of the TMM Project.
Author contributions
HY, MS, NA, and YS participated in the design of the study. HY and YS participated in data collection and revised the manuscript. HY, MS, NA, and YS conceived the study, participated in its design, and revised the manuscript. HY participated in analysis of the data and revised the manuscript. TN checked the results. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.