
Abstract
Methyl bromide is a pre-plant soil fumigant that is widely used to control nematodes, insects, and fungi in farmlands. Methyl bromide enters the human body through dermal absorption or inhalation and can damage the respiratory, nervous, circulatory, urinary, and other systems. A 62-year-old man who had inhaled a large amount of methyl bromide was admitted to our department. He presented with respiratory failure and pink foamy sputum. He was started on dexamethasone, alanyl glutamine, sulbactam, furosemide, vitamin B1, mouse nerve growth factor, and other treatments, and mechanical ventilation and continuous venovenous hemodiafiltration (CVVHF) were performed daily. He subsequently developed coagulopathy because of the CVVHF, for which protamine, recombinant human brain natriuretic peptide, and albumin were administered intravenously. Notably, the patient developed sustained anuria and eventually died owing to multiple organ failure; specifically, failure of the brain, heart, lungs, and kidneys. This report presents the diagnosis, clinical course, management, and prognosis of a patient who was treated at our hospital for severe methyl bromide poisoning.
Keywords
Introduction
Methyl bromide is a colorless, odorless gas with a low boiling point (4.6°C), high vapor pressure (1824 mmHg at 25°C), and a density three times that of air. 1 Methyl bromide is an effective pre-plant soil fumigant that is widely used to control nematodes, insects, and fungi in farmlands, thereby providing a reliable return on investment. 2 Because it is effective in killing pests and increasing crop yields, methyl bromide is popular even though its use is banned in China. 3 However, cases of methyl bromide poisoning are rarely reported in the medical literature, especially cases of patients who die from multiple organ failure. In this report, we describe a case of methyl bromide poisoning in a patient who inhaled a large amount of methyl bromide, resulting in anuria and failure of the brain, heart, lungs, and kidneys.
Case report
A 62-year-old previously healthy man drank approximately 150 g of 42% ethanol at home at noon on 11 December 2021. At approximately 13:00, he went to the plastic greenhouse to get an oil barrel (3 days after the greenhouse was fumigated with methyl bromide). He experienced headache, dizziness, nausea, vomiting, dyspnea, and weakness of the lower limbs. Therefore, he left the greenhouse and called his family at 14:07. Fifteen minutes later, his family rushed to the field and quickly took him to the emergency department of a local hospital. On arrival at 15:23, his liver and kidney function were normal, and the levels of myocardial enzymes and electrolytes were within their respective reference ranges. Brain computed tomography (CT) showed normal findings; however, chest CT revealed bronchitis and fibrous nodules in both lungs. Additionally, patchy dense shadows were observed in the middle and lower lobes of the right lung and the lower lobe of the left lung, with coronary artery calcification. The diagnosis on admission was acute methyl bromide poisoning. Approximately 8 hours after admission, the patient developed oliguria. His laboratory test results were as follows: creatinine (Cr): 305 μmol/L and pro-N-terminal brain natriuretic peptide (BNP): 7126 ng/L; his heart rate was 92 beats/minute. Twenty-four hours after admission, he developed anuria, and he was then transferred to the intensive care unit. Hemofiltration was performed using continuous venovenous hemodiafiltration (CVVHF; Prismaflex ST100; Gambro Lundia AB, Lund, Sweden). On day 2, he coughed up pink foamy sputum, developed respiratory failure, and required mechanical ventilation. CVVHF was performed daily (8 h per day), thereafter. On day 8, the patient developed anuria and became comatose.
He was transferred to our department at 11:28 on 20 December 2021 for further medical treatment. On admission, his initial vital signs were as follows: blood pressure, 129/71 mmHg; pulse rate, 95 beats/minute; respiratory rate, 18 breaths/minute; and oxygen saturation with pulse oximetry under mechanical ventilation, 98% (fraction of inspired oxygen (FiO2), 36%). Physical examination yielded unremarkable findings, except for anuria. The laboratory test results obtained at our hospital were as follows: white blood cell (WBC) count, 21.33 × 109/L; Cr, 557 μmol/L; urea, 18.3 mmol/L; myoglobin (MYO), 16,898.2 µg/L (reference range, 0–70 µg/L); serum high-sensitivity cardiac troponin I (hs-cTnI), 1925.30 µg/L (reference value, <17.5 µg/L); and BNP, 31,341.0 ng/L. Test results for rheumatic factors were negative, and the electrocardiogram findings were normal. Bedside ultrasonography showed widening of the inferior vena cava (25 mm). The diagnoses on admission were acute methyl bromide poisoning, toxic encephalopathy, acute renal failure, acute respiratory failure, and acute heart failure. Dexamethasone (40 mg, once daily), alanyl glutamine (20 g, once daily), midazolam (0.02 mg/kg/h), and furosemide (100 mg, twice daily) were administered intravenously, and vitamin B1 (100 mg, once daily) and mouse nerve growth factor (30 μg, once daily) were administered intramuscularly.
Mechanical ventilation (synchronous intermittent mandatory ventilation (SIMV) mode; f, 12 times/minute; FiO2, 40%) and CVVHF were continued daily. On day 3, the patient’s spontaneous respiratory rate was 16 breaths/minute, and the ventilator mode was changed to the continuous positive airway pressure (CPAP) mode. On day 4, 100% oxygen saturation was seen intermittently during weaning from the ventilator. On day 5, the patient was weaned from the ventilator, and oxygen by nasal tube was administered at a rate of 4 L/minute. On day 6, the patient developed respiratory failure and he remained comatose, with persistent anuria. A few moist rales were audible over both lung bases. His oxygen saturation level was 80% under high-flow oxygen, and his laboratory findings were as follows: pH, 7.19; partial pressure of carbon dioxide (PCO2), 4.0 kPa; partial pressure of oxygen (PO2), 6.5 kPa; lactate, 0.5 mmol/L; WBC count, 20.63 × 109/L; red blood cell (RBC) count, 2.24 × 1012/L; hemoglobin (Hb), 76.0 g/L; albumin, 29.4 g/L (reference range, 35–50 g/L); and Cr, 631 μmol/L. Mechanical ventilation was reinitiated, and dexamethasone was changed to methylprednisolone (40 mg, once daily). From day 7 onward, his daily urine volume was 100 mL.
On day 10, the patient coughed up pink foamy sputum (Figure 1). His vital signs were as follows: blood pressure, 108/57 mmHg; pulse rate, 98 beats/minute; spontaneous respiratory rate, 5 breaths/minute; and oxygen saturation under mechanical ventilation, 70%. Pulmonary auscultation revealed weakened pulmonary alveolar respiratory sounds with moist pulmonary rales; he also developed generalized edema. His laboratory findings were as follows: pH, 7.32; PCO2, 6.8 kPa; PO2, 10.4 kPa; WBC count, 41.46 × 09/L; RBC count, 1.44 × 1012/L; Hb, 46.0 g/L; albumin, 27 g/L; Cr, 414 μmol/L; MYO, 264.80 µg/L; hs-cTnI, 480.50 µg/L; BNP, 16,679.0 ng/L; and activated partial thromboplastin time (APTT), >180 s (reference range, 28.00–45.00 s). The patient’s oxygen saturation gradually decreased, and this was attributed to anemia, lung injury, and other conditions, and he received a blood transfusion. Moreover, notable abnormalities in coagulation function, related to CVVHF, were observed. Protamine (50 mg), and recombinant human BNP (0.0075 μg/kg/minute, micropump injection) and albumin (50 g, once daily) were administered intravenously. On day 12, his blood pressure was 90/37 mmHg, and his pulse rate was 115 beats/minute. Continuous renal replacement therapy (CRRT) was discontinued, and norepinephrine was administered intravenously to maintain blood pressure. At 11:36 on day 13, the patient showed no signs of spontaneous respiration. He then experienced cardiac arrest at 13:40 (details of the main examinations are shown in Table 1 and those of the changes in daily urine output are shown in Figure 2).

Image of the patient’s pink foaming sputum obtained on day 10 of admission.
Clinical laboratory results of the patient at admission to our department and on days 7 and 10.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; BNP, N-terminal brain natriuretic peptide; BUN, blood urea nitrogen; CK, creatine kinase; Cr, creatinine; Hb, hemoglobin; LDH, lactate dehydrogenase; PLT, platelets; RBC, red blood cells; WBC, white blood cells; CK-MB, creatine kinase-MB; hs-cTnI, high-sensitivity cardiac troponin I.
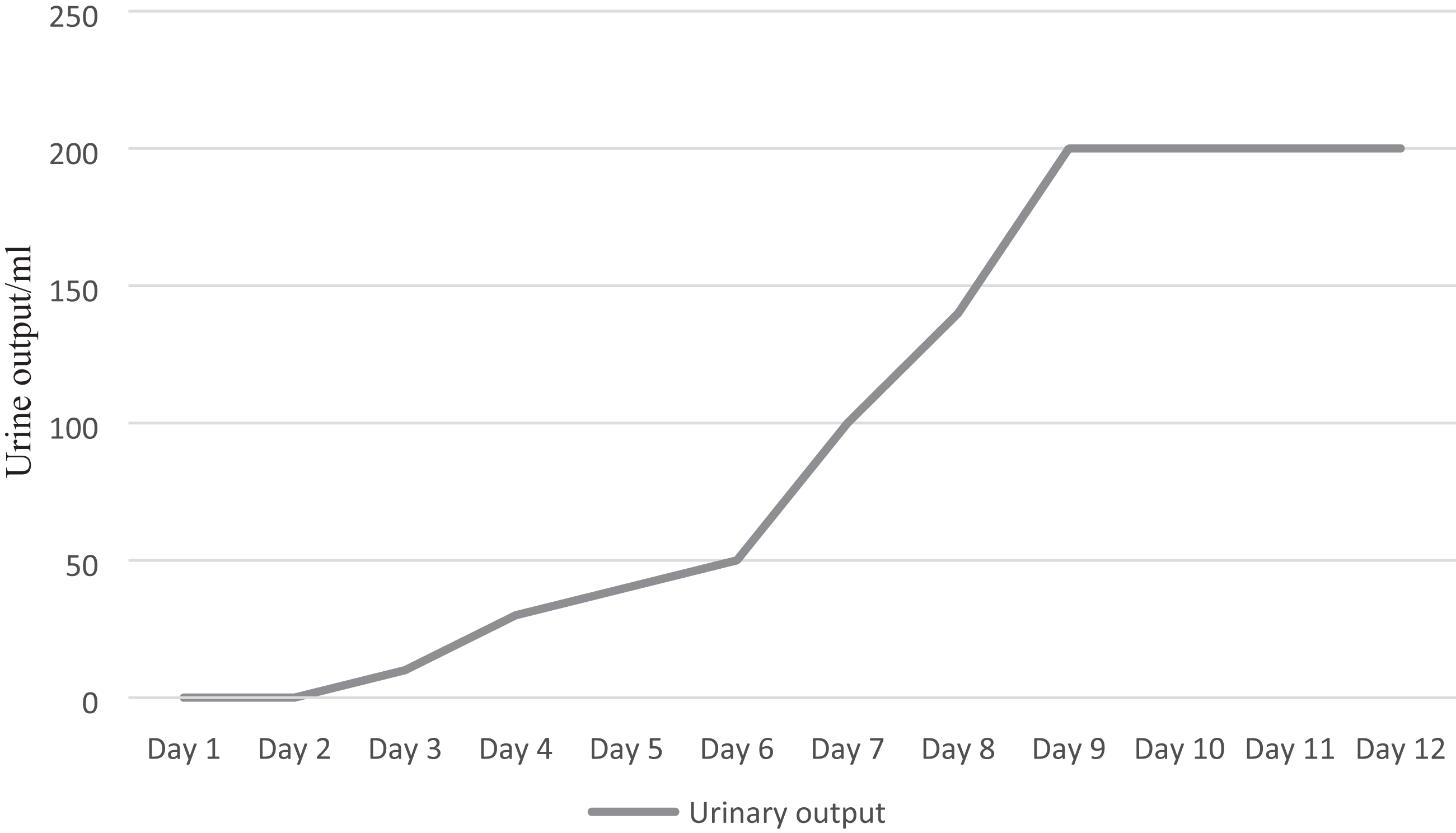
Changes in the patient’s daily urine output after admission to our department.
The poisoning incident had occurred 3 days after methyl bromide was injected into the soil. Professionals had used a soil sterilizer to inject five bottles (681 g/bottle, 24 bottles/box) of methyl bromide into 1667 square meters of soil. The soil was then sealed with a polythene film to reduce volatilization of the methyl bromide and increase its permeability into the soil. The patient had entered the greenhouse, which had no ventilation, to obtain an oil barrel, and he did not use protective equipment.
Discussion
This report presents a case of methyl bromide poisoning that led to multiple organ failure and anuria, which occurred early after the poisoning. Bromomethane can greatly improve the biological activity of soil, and rapidly kills most pests at very low concentrations; it is used on farms, and in warehouses, transportation, and buildings.2 Methyl bromide enters the human body via skin absorption or by inhalation, and most cases of methyl bromide poisoning are owing to inhalation. 4 Inhalation of a small amount of methyl bromide can cause headache, dizziness, visual disturbance, nausea and vomiting, and other adverse effects; it can also have fatal consequences, such as seizures, coma, respiratory or circulatory failure, pulmonary edema, and pulmonary hemorrhage. 4 Animal studies have shown that when methyl bromide is inhaled, it is rapidly absorbed in the lower respiratory tract and distributed to various tissues.5,6 The lungs, liver, and kidneys are the main organs to which methyl bromide is distributed. 6 In previous studies, neurotoxicity was evident in rats exposed to concentrations below 260 ppm, and lung congestion and edema were observed after exposure to 260 to 5200 ppm methyl bromide.7 Kidney lesions were observed grossly at concentrations above 900 ppm, and liver congestion and hemorrhage were observed at 1200 ppm. 8 Our patient had inhaled a large amount of methyl bromide, and he rapidly developed acute renal failure and anuria accompanied by damage to the lungs, liver, and central nervous system. Our patient may have been exposed to a high concentration of methyl bromide that ultimately led to multiple organ failure and death.
Chronic exposure to methyl bromide is characterized by disorders of the nervous system; however, cases of persistent anuria owing to acute methyl bromide inhalation have been reported rarely. Acute poisoning can cause damage to the respiratory, nervous, circulatory, urinary, and other systems. 9 Many reports of methyl bromide poisoning have been published. In 1996, Yamano et al. 10 reported that methyl bromide fumigation of grain depots damaged the nervous and respiratory systems of those in close proximity to the depots. In 2013, Stromberg et al. 9 published their report of a 22-year-old woman who rapidly developed respiratory and neurological symptoms after opening a tank of compressed methyl bromide in her car. In 2013, de Souza et al. 11 reported that long-term exposure to methyl bromide affected the dentate nucleus of the cerebellum, brainstem, and splenium of the corpus callosum. In 2017, Sue et al. 12 reported a case of chemical burns caused by methyl bromide.
Previous studies13–15 have shown that the mechanism of toxicity of methyl bromide is related to its alkylation ability, as follows: (i) the direct methylation of key biomolecules by methyl bromide leads to toxicity and (ii) after initial methylation of endogenous molecules, the active metabolites generate toxic substances. The following causes of death have been reported: (i) lack of reliable warning features, delayed symptom onset, and high soil temperature causing the volatilization of methyl bromide, 16 (ii) lack of an antidote, (iii) mechanisms of injury being unknown; and (iv) multiple organ failure. We did not estimate the serum bromide levels of our patient because he was not transferred to our department until the eighth day, and methyl bromide is rapidly metabolized in the body after exposure.
Currently, there is no specific antidote for methyl bromide poisoning, and comprehensive treatment is the only option. 17 Glucocorticoids have rapid, powerful, and nonspecific anti-inflammatory effects. 18 CVVHF can reduce the serum levels of methyl bromide 11 and improve kidney function; however, there is no evidence that dialysis affects patient outcomes.
Methyl bromide poisoning involves multiple organs, such as the brain, heart, lungs, and kidneys. In severe cases, methyl bromide poisoning can lead to early acute renal failure and anuria; there is no specific antidote. Further studies are needed to find ways to control organ injury caused by methyl bromide.
Footnotes
Author contributions
XDJ, YQL, and GCY conceptualized the report. ZXW supervised the data collection. YQL, LKS, and LWZ drafted the report, and all authors contributed substantially to its revision. YQL, WJW, and XDJ take responsibility for the report as a whole.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
This report conforms to the CARE guidelines. 19 Ethics approval was obtained from the Qilu Hospital Ethics Committee for Human Research (approval number: KYLL-202107-806). Written informed consent was obtained from the patient’s legal representatives for treatment and publication of the case details and accompanying figures.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.