
Abstract
This case report introduces digital surgery-first approach orthognathic surgery assisted by three-dimensional virtual planning and combined with invisible orthodontic treatment for a 21-year-old female patient with a skeletal Class III high-angle gummy smile malocclusion. We explored the clinical significance of the widespread application of digital technology for rapid development of the orthodontic/orthognathic field. The regional acceleratory phenomenon and clear aligners were used to achieve fast and aesthetic tooth movement after surgery. The treatment lasted only 8 months, and the patient was satisfied with the aesthetic results. The results remained stable after 1 year of follow-up. This case report highlights the advantages of combining a digital design and a surgery-first approach to produce accurate, rapid, safe, stable, and fulfilling cosmetic results. The combination of the surgery-first approach and clear aligners can facilitate patient-oriented surgical orthodontic treatment.
Keywords
Introduction
The surgery-first approach (SFA), introduced in orthognathous surgery in recent years, has become popular among patients because of immediate improvements in the facial contour and shorter treatment times. Different from the traditional three-stage method, it can quickly correct the maxillomandibular position, providing a favorable environment for tooth movement.1–3 Previous studies have shown the regional acceleratory phenomenon (RAP) effect of the SFA,4,5 explaining why this new surgical method can achieve safe, rapid, and stable movement. Clear aligners are gaining popularity over traditional fixed orthodontics in the orthodontic market because of their transparency and comfort; hence, many clear aligner products have become available.6,7 The present case report introduces a treatment innovation for a patient with a skeletal class III gummy smile that combines the SFA and clear aligners, with the total treatment being completed within 8 months. The treatment process was designed digitally, which improved the accuracy of the treatment plan and the precision of surgical execution, thus improving the overall treatment outcome. Digital techniques will eventually supplant traditional techniques altogether, improving the quality of oral rehabilitation, the economics of dental practice, and the patients’ perceptions. 8
Case report
The reporting of this study conforms to the CARE guidelines. 9
This paper describes our evaluation and treatment of a 21-year-old female patient with a gummy smile, maxillary and mandibular protrusion, and mandibular angle asymmetry (Figure 1). This study was reviewed and approved by the Medical Ethics Committee of The Affiliated Hospital of Qingdao University (approval number: QYFYWZLL26977), and the patient provided verbal informed consent for publication of her information and images. The patient’s self-reported dental history was as follows. Five years previously, she had undergone fixed orthodontic treatment in another hospital for an open bite. Six months after the end of the treatment, her retainer was accidentally lost and she stopped maintenance treatment. Pretreatment facial evaluation at our hospital showed a hyperdivergent pattern of growth and asymmetrical mandibular angle, and intraoral photographs showed a gummy smile (Figure 1). Clinical examination revealed that both the maxillary and mandibular dental midlines were not coincident with the facial midline, instead deviating to the left. She had an overjet of 1.3 mm, an overbite of 0 mm, a Class I cuspid molar relationship on the right, a Class III cuspid relationship on the left, and a crossbite in the left premolar area. The patient also exhibited slight elongation in the lower third of the face and tension in the chin muscles when the lips were closed. A panoramic radiograph (Figure 2) showed that all teeth were present, including all four third molars. A lateral cephalometric radiograph analysis (Table 1) led to a diagnosis of skeletal Class III malocclusion (ANB = 0.9°, Wits = −4.9 mm) with a hyperdivergent growth pattern (Frankfort-mandibular plane angle = 31°).

Pretreatment facial and intraoral photographs.
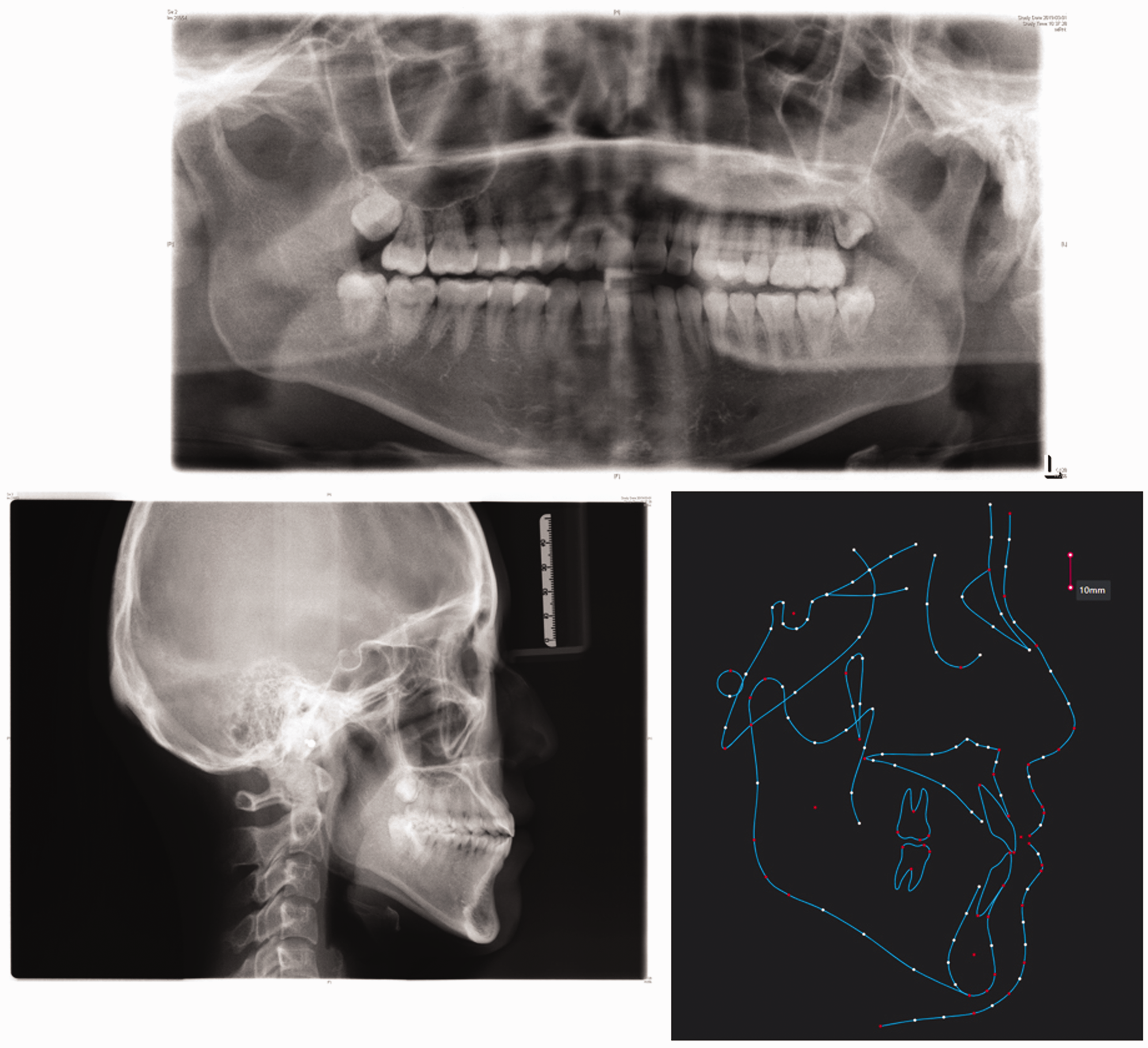
Pretreatment panoramic radiograph, lateral cephalometric radiograph, and cephalometric analysis.
Cephalometric measurements (Tweed analysis).

SD, standard deviation; FMA, Frankfort-mandibular plane angle; FH, Frankfort horizontal plane; MP, mandibular plane; AFH, anterior facial height; PFH, posterior facial height.
The treatment objectives were to (1) improve the skeletal Class III malocclusion and gummy smile and correct the mandibular asymmetry, (2) establish a skeletal and dental Class I relationship, and (3) coordinate the transverse width of the maxillary and mandibular arches and release the individual tooth position crossbite in the posterior region.
Because the patient was diagnosed with skeletal Class III malocclusion with mandibular angle asymmetry and an obvious gummy smile, orthodontic/orthognathic combined treatment was the first choice. The patient also had the option of using implant anchorage-assisted camouflage orthodontic treatment. We explained the advantages and limitations of each approach in detail to the patient before treatment began. Because of the relatively orderly arrangement of her teeth and high requirements for aesthetics and time, she chose digital design-assisted SFA combined with postoperative invisible correction. She provided informed consent regarding this choice of surgical method.
We completed the preoperative digital surgery design (Figure 3) followed by the digital invisible orthodontics design (Figure 4). A cranial and maxillofacial computed tomography scan was performed before surgery, and the computed tomography data were imported into Mimics 20.0 software to establish the original digital model. Hard tissue markers were determined for three-dimensional (3D) reconstruction and measurement, analysis, diagnosis, surgical design, and guide plate fabrication. The operation was completed according to the digital surgical design and involved LeFort I osteotomy, bilateral sagittal split ramus osteotomy, and gonioplasty. During the orthognathic surgery, LeFort I osteotomy with impaction of 3 mm improved the gummy smile. The bone was moved 0.5 mm to the right to align the tooth midline with the facial midline, with the upper central incisor serving as the rotation center. Clockwise rotation of 2.0° in the sagittal plane, anticlockwise rotation of 0.5° in the coronal plane, and clockwise rotation of 0.5° in the horizontal plane were performed to harmonize the 3D symmetry. During mandibular bilateral sagittal split ramus osteotomy, according to the terminal occlusion position, the Pg point was used as the reference, and the bone was lifted 4.4 mm and moved 0.7 mm forward. Gonioplasty was performed to coordinate the symmetry of both mandibular angles, and all four third molars were extracted. All procedures were performed by one surgeon.

Preoperative digital surgery design. (a) A 0.5-mm right shift was performed to align the midline of the tooth with the midline of the face. (a–c) With the upper central incisor as the center of rotation, the sagittal plane was rotated 2.0° obliquely, the coronal plane was counter-rotated by 0.5°, and the horizontal plane was counter-rotated by 0.5° to adjust the symmetry and (c) The bone was raised 3.0 mm to improve the gummy smile.

Digital invisible design. (a) Initial ClinCheck images and (b) Final ClinCheck images.
Intermaxillary fixation was performed for 14 days after surgery. Postoperative orthodontic procedures were initiated after the guide plate was removed and functional recovery was achieved, with a mouth-opening width of at least 40 mm and stabilization of occlusion. The time required for surgery was included in the total treatment time. Postoperative evaluation revealed improvements in the patient’s facial shape with normalization of the overjet, overbite, and bilateral posterior sagittal relationship. These improvements were then reinforced using fine adjustment and alignment with a clear aligner (Figure 5), allowing us to align, level, and compensate for these changes. This facilitated coordination of the dental arch width and maxillary and mandibular occlusion. The invisible aligner was designed in 26 steps, and application of the RAP following surgery allowed the patient to change her aligners every 5 days, greatly reducing the total treatment time (the clear aligner lasted only 130 days). The orthodontic treatment was determined to be complete when a stable occlusion, proper alignment of the teeth, and appropriate overjet and overbite had been obtained. Some scholars have suggested that increased tooth movement after orthognathic surgery may be caused by increased activity and metabolic changes of osteoclasts in the alveolar bone caused by the surgery. The postoperative orthodontic treatment should be started no later than the second week after surgery so that the postoperative RAP can be used to shorten the treatment time. 17

Facial and intraoral photographs after 4 months of treatment.
The treatment (Figure 6) produced a more desirable occlusion with ideal overbite and overjet. It also facilitated a Class I bilateral cuspid molar relationship, improving the overall facial shape. Lateral imaging revealed a straightened face shape, reducing the elongation of the lower third of the face and reducing the appearance of the gummy smile. The patient’s improved smile and smile arc were coincident with her lower lip curvature. The patient exhibited bilateral mandibular angle symmetry and coordination. The treatment aims were accomplished, the patient’s chief complaints were addressed, and good occlusal and aesthetic results were achieved. The patient was satisfied with the treatment outcome.

Facial and intraoral photographs after another 8 months of treatment (completion).
The retention phase, initiated after completion of the orthodontic treatment, was not included in the treatment time. The total treatment lasted for 8 months, application of the maxilla bonded wire from 12 to 22 months (Figure 7 (a), red arrow), and application of the mandible bonded wire from 33 to 43 months (Figure 7(a), blue arrow). Clear retainers were worn on both the maxilla and mandible at night only.

Post-treatment panoramic and lateral cephalometric radiograph.
Good root parallelism was obtained via panoramic radiography, and no alveolar bone loss or root resorption was observed (Figure 7(a)).
Cephalometric analysis revealed significant changes (Figure 7(b), (c); Table 1). The ANB increased considerably from 0.9° to 2.6° and Wits from −4.9 to −1.9 mm; these changes were partly due to the clockwise rotation of the mandible (Figure 7(d)), which was necessary to correct the skeletal Class III malocclusion and posterior crossbite. The mandible underwent clockwise rotation, changing the mandibular plane (Frankfort-mandibular plane angle) from 31.0° to 33.5° (Figure 7(b)).
After 12 months of retention (end of treatment), both the occlusion and the facial shape remained well (Figure 8). Three-stage lateral cephalographic overlaps demonstrated stability after treatment for 1 year (Figure 9). One limitation of this case, however, is that the follow-up was not long enough to determine the long-term stability of the treatment effect. Further observation is needed to obtain these data.

One-year post-treatment follow-up facial and intraoral photographs.

Superimposition of cephalometric tracings. black, pretreatment; red, post-treatment; blue, 1-year follow-up.
Discussion
Traditionally, preoperative orthodontic treatment has been considered an important step to overcome postoperative occlusal instability and achieve a successful outcome of orthognathic surgery. 10 The standard three-stage model has been widely used and has achieved good results. However, this technique still has shortcomings such as the long treatment cycle and aesthetic impact. Different studies have shown that the average preoperative orthodontic time ranges from 15.4 to 25.0 months 11 and can even be as long as 47 months. During this process, the patient’s jaw malformation and occlusal disorder usually cannot be improved, and they become more serious after removal of the tooth compensation,12,13 which increases the patient’s psychological pressure. Preoperative orthodontics may also increase the patient’s chances of gingival regression, gingival hyperplasia, dental caries, root absorption, occlusal dysfunction, and chewing and speech discomfort and may reduce his or her quality of life and compliance. 13 With the higher pursuit of aesthetics and the continuous progress of orthognathic surgery, the SFA (i.e., orthognathic surgery before orthodontic treatment) has gradually shown advantages in improving the occlusion function and appearance at an early stage and shortening the treatment time, 12 thus attracting increasingly more attention.
The SFA not only eliminates preoperative orthodontic treatment but also speeds up postoperative orthodontic treatment by utilizing the RAP, thus further reducing the total time of treatment. The RAP was first proposed by Frost14,15 in 1989 and states that the rate of remodeling of adjacent bone tissue increases after trauma or surgery. Liou et al. 16 reported that the RAP is a complex physiological process, the main characteristics of which include accelerated bone remodeling activities and decreased bone mineral density in some regions. Studies have confirmed that the mobility of the upper and lower incisors and the serum level of C-terminal telopeptide of type I collagen are significantly increased from 1 week to 3 months after surgery and recover to the preoperative level in the fourth month after surgery. There is a significant correlation between the two changes. An increased concentration of C-terminal telopeptide of type I collagen indicates increased osteoclast activity and decreased bone mineral density. Therefore, the increased tooth movement after orthognathic surgery may be caused by increased activity and metabolic changes of osteoclasts in the alveolar bone caused by the surgery. Postoperative orthodontic treatment of patients should thus be started no later than the second week after surgery, allowing the postoperative RAP to shorten the treatment time. 17
Despite the obvious advantages of the SFA model, one difficulty is the need to overcome postoperative occlusal instability. This not only challenges the status quo but also constitutes a new model of cranio-maxillofacial surgery. There are two main ways to address this obstacle. First, Korean researchers seem to have taken advantage of the fact that surgery is performed in the same direction as postoperative orthodontic treatment. 18 Second, Japanese researchers rely heavily on aggressive preoperative and postoperative tooth management, including the use of cusp grinding and miniature screws, to compensate for surgical errors or skeletal relapse. 19
It should be noted that the SFA still has limitations and disadvantages. One is its unclear stability. Comparison of the therapeutic effect and stability between the SFA and traditional treatment is still controversial in the academic circle, but it is generally believed that the therapeutic effect and stability are not significantly different between the two. Seifi et al. 20 reported that there was no significant difference between the two treatment modes in the stability of the jaw and teeth after treatment for patients with Class III malocclusion. Jeong et al.21,22 compared the long-term anteroposterior and vertical stability of the mandible in patients with Class III malocclusion undergoing the SFA or traditional treatment mode and found no significant difference. Several reviews have described the therapeutic effect and stability of the SFA in patients with skeletal Class III malocclusion.
Huang et al. 23 reported that the SFA could achieve the same or better long-term treatment effect compared with the “orthodontic-orthognathic-orthodontic” treatment model for patients with skeletal Class III malocclusion, including transverse, vertical, and sagittal stability of the jaw and teeth. Peiro-Guijarro et al. 4 found that the SFA is a stable and predictable treatment for patients with skeletal Class III malocclusion but that its stability is not as good as that of traditional treatment. It should be emphasized that analysis of the treatment efficacy and stability is susceptible to a variety of confounding factors, such as differences in indications, surgical procedures, 22 and orthodontic and orthognathic surgeons’ skill levels. Because of the large clinical heterogeneity of the literature to date, a meta-analysis cannot be conducted, and the level of evidence provided is very limited. Moreover, most existing reports describe retrospective studies; thus, prospective studies with a sufficient sample size are still needed to provide more precise evidence for evaluation of the therapeutic effect and stability. Another limitation in terms of the indications for the SFA is that this technique is not suitable for patients with crowded dentition, steep curve of Spee, or large inclination of the upper incisors; for this group of patients, preoperative orthodontic compensation is still required. 23
Traditional orthognathic surgical design is based on two-dimensional X-ray images, 24 such as cephalometric tracings and plaster casts. There are inevitably deviations in the steps of dental cast making, face bow transferring, and model surgery; it is difficult to predict exactly what movement is required, and prediction of the postoperative facial appearance is not intuitive enough. However, patients undergoing orthognathic surgery often have higher aesthetic and functional requirements than patients undergoing other types of surgery, and planning requires a high degree of accuracy, meaning that even small deviations can result in suboptimal results. Digital orthognathic planning can obtain more accurate cranio-maxillofacial features of patients through 3D reconstruction and matching of the patients’ craniomaxillofacial CT, 3D photography, dentition model scanning, and other digital imaging data to achieve more accurate measurement, diagnosis, virtual design, guide plate creation, and postoperative effect evaluation. 25 The virtual surgical plan can determine the optimal position of the osteotomy line and rigid fixation with the help of a surgical guide.26,27 Using 3D virtual orthodontic simulation, orthodontists can accurately predict the tooth movement required for the final occlusion. 17 All of these techniques improve the accuracy of the treatment plan and the precision of surgical execution, thus improving the overall treatment outcome.26,28 Given the continuing development of related software, the future of digital design will become simpler and more accurate and facilitate better surgical and aesthetic outcomes for these patients.
The invisible aligner system is a new type of orthodontic treatment technology that was first introduced in the United States in the late 1990s. It uses image processing and computer-aided design and fabrication technology with rapid prototyping technology to assist in orthodontic treatment. 29 This technology enables the design of tooth movement by 3D visualization and involves the processing and fabrication of a series of transparent, non-bracket, elastic plastic aligners that control the magnitude and direction of orthodontic forces, thus achieving the goal of realistic, visualized orthodontic treatment. 29 Compared with traditional fixed orthodontic devices, invisible orthodontic devices have the characteristics of beauty, comfort, and convenience for the patient. In recent years, clear aligners have been widely used in clinical practice and are favored by the majority of patients; thus, they are gradually occupying a larger place in the field of orthodontics. The clear aligner needs to be worn for >22 hours per day to achieve a satisfactory orthodontic effect, and treatment compliance is high. 30 Invisible orthodontic technology can also be used to predict the results of orthodontic treatment by digital 3D reconstruction, allowing the patients to directly watch the a dynamic simulation video of the process and results of their orthodontic treatment; this is convenient for doctor–patient communication. After design and machining, the orthodontic teeth can be moved to the final position, avoiding the round-trip tooth movement during fixed orthodontic treatment and reducing the risk of root absorption. 31 In addition, the time interval between return visits in patients with clear aligners is longer, which can effectively decrease the treatment time and improve the effect. 29 Thus, clear aligners are of great significance in the development of orthodontic technology and are worthy of widespread clinical application.
With the recent remarkable improvements in people’s material and spiritual lives, the demand for beauty is constantly increasing. Facial attractiveness plays a crucial role in social interactions. 32 Therefore, it is not surprising that an increasing number of people are seeking orthodontic treatment to improve the aesthetics of their smile. A “gummy smile” is defined as exposure of more than 3.0 mm of gingival tissue during a forced smile. 33 This not only negatively affects smile aesthetics but can even influence self-esteem and social relationships. 32 In the present case, one of the patient’s chief complaints was a gummy smile. Her initial smile was obviously gummy with a larger buccal gallery area on both sides, resulting in a less full smile; she also had a too-straight dental arch, unattractive smile arc, and several other aesthetic problems. However, we were able to combine digital design, surgical adjustment of the jaw position, and postoperative fine adjustment to improve the aesthetic attractiveness of the patient’s smile, and her smile was filled out to produce a more youthful look. The components of a smile also influence each other, making it necessary for orthodontists to understand the complex relationship between these components to achieve ideal smile aesthetics following orthodontic treatment and achieve overall facial harmony.33,34
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221094524 - Supplemental material for Combining a digital design-mediated surgery-first approach and clear aligners to treat a skeletal Class III defect for aesthetic purposes: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605221094524 for Combining a digital design-mediated surgery-first approach and clear aligners to treat a skeletal Class III defect for aesthetic purposes: a case report by Lei Kong, Xinqiang Liu and Jie Zhang in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.