
Abstract
Klebsiella pneumoniae invasion syndrome (KPIS) is a critical multi-site infection that is usually caused by highly virulent Klebsiella pneumonia. It is relatively common in Asian patients with diabetes and leads to sepsis, which has a high mortality rate. We report the case of a man in his early 40s who presented to the hospital with blurred vision in his left eye of 7 days’ duration and fever of 1 day’s duration. After a complete examination, he was diagnosed with KPIS on the basis of his liver abscessation, lung abscessation, endophthalmitis of the left eye and brain abscessation. After needle puncture and drainage of the left eye and liver abscess and anti-bacterial treatment with meropenem, the patient recovered well. When KPIS is suspected, attention should be paid to the sites of infection and the selection of the most appropriate antibiotics, but the most important aim should be to drain the lesions in a timely manner to improve the patient’s prognosis.
Keywords
Introduction
Klebsiella pneumoniae (Kp) is a gram-negative bacillus that is usually cultured from community-acquired infections. Kp infection can cause a combination of liver abscessation and metastatic infections, in the form of meningitis, brain abscessation, lung abscessation, endophthalmitis and/or necrotising fasciitis, and this is collectively referred to as Klebsiella pneumoniae invasive syndrome (KPIS).1–3 KPIS was first reported in Taiwan in the 1980s and usually occurs in Asian individuals with weakened immune systems. The associated mortality rate has been estimated as 3% to 42%, but in the presence of intracranial infection it can be as high as 38% to 91%.2–4 However, there is a lack of published guidelines for the diagnosis and treatment of Kp.
Characteristics of the patient
The patient was a man in his early forties who was admitted to the hospital on 30 April 2021 with blurred vision in the left eye of 7 days’ duration and fever of 1 day’s duration. The highest temperature recorded was 39°C, but he did not report chills, vision loss, cough, abdominal pain, vomiting, or headache. He attended a community hospital initially, where chest computed tomography (CT) was performed, and revealed multiple lung nodules, suggestive of tuberculosis (TB). He then attended our hospital for further treatment.
Clinical findings
The patient’s vital signs when they first attended our hospital were as follows: temperature 37.2°C, blood pressure 137/75 mmHg, heart rate 132 beats/min, respiratory rate 18 breaths/min, and blood glucose (Glu) concentration unmeasurably high (Accu-Chek Performa; Roche, Basel, Switzerland). No significant abnormalities were found on chest, abdomen, or nervous system examinations. The purified protein derivative and TB spot tests were both negative.
Diagnostic assessment
Laboratory testing, including arterial blood gas analysis, revealed the following: pH 7.12, PaCO2 11 mmHg, PaO2 120 mmHg, HCO3− 3.6 mmol/L, Glu 37.5 mmol/L, lactic acid 1.5 mmol/L and anion gap 33 mmol/L. A complete blood count revealed the following: white blood cell (WBC) count 5.8 × 109 /L, haemoglobin (HGB) 163.00 g/L, platelet (PLT) count 34.00 × 109 /L, and neutrophil (NEUT)% count 79.00%. The biochemical data were as follows: blood urea nitrogen (BUN) 17.5 mmol/L, creatinine (CRE) 108.8 µmol/L, C-reactive protein (CRP) 2.67 µmol/L, albumin (ALB) 316 µmol/L, glycosylated haemoglobin (HbA1c) 12.0% and procalcitonin (PCT) 32.06 ng/mL. The alanine aminotransferase (ALT) and aspartate aminotransferase (AST) activities and the total bilirubin (TBIL) and direct bilirubin (DBIL) concentrations were within their normal ranges. Routine dipstick urinalysis revealed ketones (KET) 4+, but no WBCs.
The results of imaging examinations were as follows. Abdominal ultrasonography revealed a hypoechoic mass of approximately 7.0 × 6.0 cm in the upper segment of the right posterior lobe of the liver ( Figure 1a ), and chest CT showed multiple cystic and solid lung lesions that were considered to be lung abscesses ( Figure 2a ). Abdominal enhanced CT was then performed to refine the diagnosis, and this revealed irregular, multilocular, cystic low-density shadows in the right posterior lobe of the liver. These shadows were approximately 62 mm × 47 mm × 67 mm in size, and a small amount of gas shadow could be seen. The enhanced scan showed differing thicknesses and separation enhancements of the lesions, and there was no obvious enhancement of the capsules ( Figure 3 ). Cranial CT showed multiple, bilateral, round low-density nodules within the grey matter junction of the brain parenchyma. Cranial magnetic resonance imaging (MRI) showed multiple plaques and circular or long signals on T1-weighted imaging, and signals in the cerebellar cortex, subcortex and white matter of the brain on T2-weighted imaging, indicative of multiple brain abscesses ( Figure 4a ). An ocular examination was performed by an ophthalmologist and revealed conjunctival hyperaemia, corneal oedema, a deep anterior chamber, empyema and no light perception in the left eye ( Figure 5a ), while the right eye was normal. Blood culture results revealed the presence of gram-negative bacilli, and the culture of Kp was reported the following day ( Figure 6 and Table 1 ). Sputum cultures yielded the same organism ( Table 1 ).

Results of abdominal ultrasonographic examinations. (a) An uneven echo of 6.94 × 5.94 cm in size was identified in the upper segment of the right posterior lobe of the liver. (b) A non-homogeneous zone was identified in the right posterior lobe of the liver, but the previous low-density foci were less marked than 6 weeks previously.

Chest computed tomography images. (a) Multiple cystic and solid lung lesions were identified. The differential diagnosis included a lung abscess. (b) The amount of exudation was less and the lung nodules were smaller than previously.

Abdominal enhanced computed tomography images. Irregular low-density shadows, consistent with multi-locular cysts, were identified in the right posterior lobe of the liver that were approximately 62 mm × 47 mm × 67 mm in size, and there was a small area of gas shadow. The enhanced scan revealed that the lesions were of differing thickness and separation enhancement, but there was no obvious enhancement in the capsules.
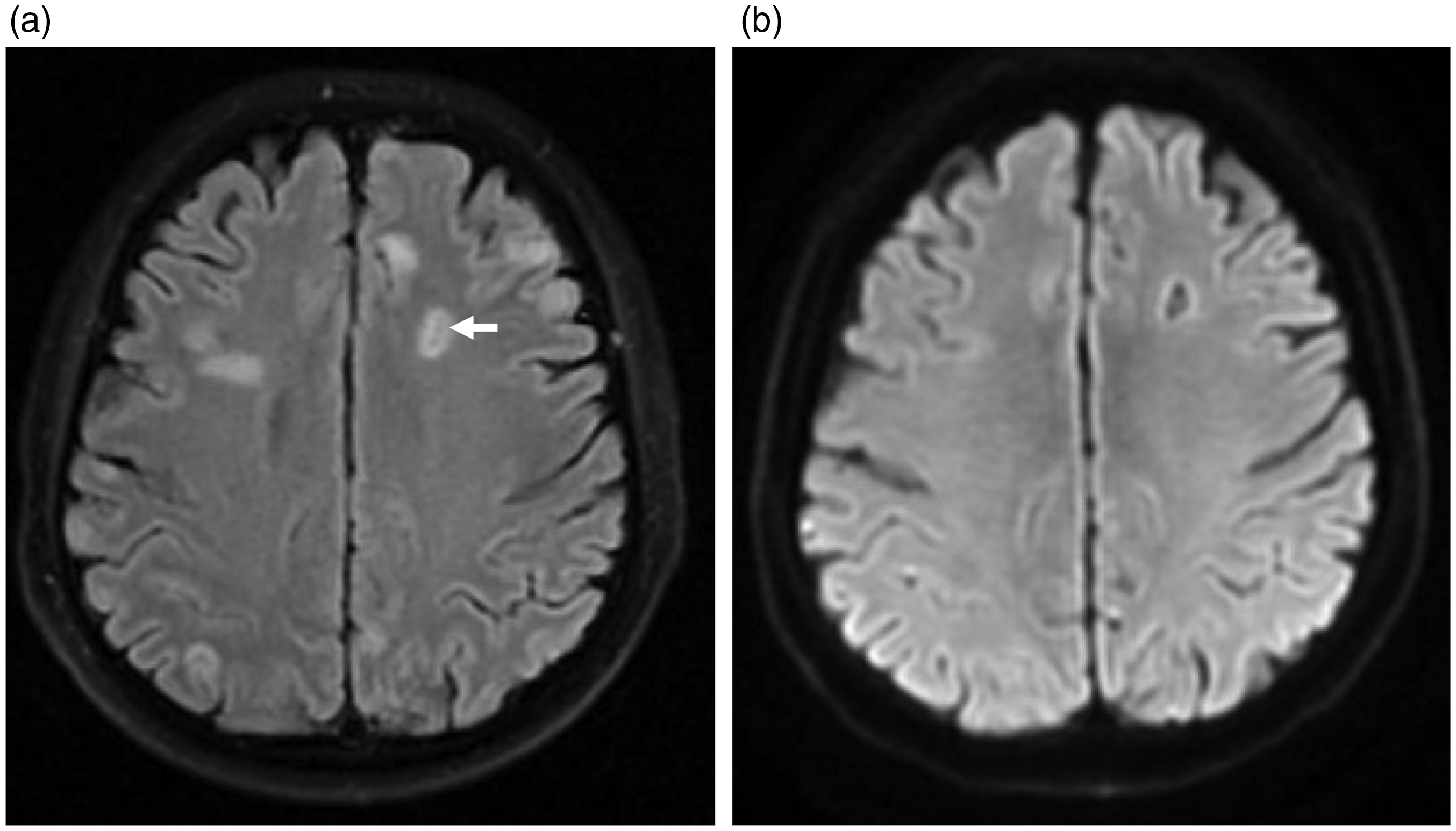
Cranial magnetic resonance images. (a) Multiple circular or long plaques were identified on T1-weighted imaging, long plaques were identified on T2-weighted imaging, and high-intensity signals were present bilaterally within the cerebellar cortex, subcortex and white matter of the brain on diffusion-weighted imaging. The presence of localised high-intensity signals in the left frontal lobe implied the presence of multiple brain abscesses. (b) Low-density nodules were identified in the skull, but these were significantly smaller than previously.

Results of ocular examinations. (a) Examination of the left eye by an ophthalmologist revealed no light perception, conjunctival hyperaemia, corneal oedema, a deep anterior chamber and empyema. (b) The conjunctival hyperaemia had improved and there was no purulent exudate in the anterior chamber, but corneal oedema and a deep anterior chamber remained.

Positive string test for the Klebsiella pneumoniae isolated from the present patient.
Antibiogram for the Klebsiella pneumoniae isolated from the present patient.

S, sensitive; MIC, minimum inhibitory concentration.
The initial diagnosis was KPIS (on the basis of liver abscessation, lung abscessation, endophthalmitis of the left eye and brain abscessation), sepsis and diabetic ketoacidosis.
Therapeutic intervention
The patient was administered antibiotic therapy via a pump, consisting of meropenem 2 g over 3 hours every 8 hours, fluid therapy, volume expansion therapy, blood glucose control therapy and ofloxacin eye drops every 8 hours. For glucose control, an insulin infusion (6–8 U/h) and 3,000 mL saline was administered intravenously, then when a glucose concentration of 11.1 mmol/L was achieved, the insulin infusion was reduced to 3–6 U/h and an intravenous infusion of glucose/saline was administered. When urine ketones became negative, subcutaneous insulin treatment was instituted. One day after admission, the patient’s pH, HCO3−, CRE, BUN and urine KET were normal, and his concentrations of glucose were approximately 7 mmol/L when fasting and 10 mmol/L post-prandially.
After 3 days of antibiotic treatment, the patient still had a fever, with a temperature of 40°C. His laboratory results were as follows: WBC count 8.28 × 109/L, PLT count 12.00 × 109/L, NEUT% 83.60%, PCT 41.05 ng/mL, ALB 18 g/L and positivity for Kp on blood culture. Considering his poor response to treatment, transconjunctival vitrectomy was performed. The left vitreous body and retina were grey, with white purulent ulcers, and a large amount of dense purulent exudate was identified sub-retinally during surgery. In addition, puncture and drainage of the liver abscess were performed under ultrasonographic guidance. Bacteriological analysis of the liver abscess and vitreous revealed the presence of Kp ( Table 1 ). Following these procedures, the patient’s temperature returned to normal; his WBC count, CRP and PCT substantially decreased and his PLT count began to increase ( Table 2 ). His blood culture became negative after 2 days, and 1 week later, all the tested parameters were within the normal ranges ( Table 2 ).
Blood parameters for the present patient.

A-Day, day following surgery; T, highest temperature recorded each day; WBC, white blood cell; CRP, C-reactive protein; PCT, procalcitonin; PLT, platelet.
Antibiotic treatment was continued with meropenem 2 g via pump for nearly 3 hours every 8 hours for 6 weeks after surgery, and chest CT at the end of this period showed that the volume of lung exudate was significantly less than before ( Figure 2b ). Abdominal ultrasonography showed that the liver abscess had decreased in size ( Figure 1b ) and cranial MRI showed a similar change in the brain abscess ( Figure 4b ). Ocular examination revealed corneal oedema and a deep anterior chamber, but no purulent exudate in the anterior chamber and an amelioration of the conjunctival hyperaemia ( Figure 5b ). After continuing meropenem treatment for a further 2 weeks, no obvious hypoechoic regions were apparent on abdominal ultrasonography, and cranial MRI showed no low-density areas, implying that the abscess had been totally reabsorbed. Therefore, the patient was discharged on ceftriaxone 2 g once daily for 1 week.
Follow-up and outcomes
A further 2 weeks later, there were no signs of recurrence on chest CT, abdominal ultrasonography or cranial MRI and the patient had recovered well.
Discussion
Kp is commonly cultured from community-acquired infections and exists as multiple serological types: capsule (K antigen type, mainly K1 and K2), mucoviscosity-associated gene A (magA, viscosity-related genes), regulator of mucoid phenotype A gene (rmpA) and aerobactin serotypes.5,6 The K1 and K2 capsule serotypes and rmpA contribute to hypermucoviscosity,6–8 which is a known virulence factor for Kp and is confirmed using a string test, in which positivity is defined as the formation of >5-mm-long viscous strings when colonies on an agar plate are stretched ( Figure 6 ). Previous studies have shown that the accuracy of the identification of highly virulent Klebsiella pneumoniae (hvKP) using the positive string test is as high as 90%, 9 while others have shown that the accuracy of identification of highly virulent gram-negative bacilli in the lung using the string test is 50%. 10 However, the identification of serotypes is time-consuming and complicated, and hvKP can be strongly suspected on the basis of string testing in clinical practice.
KPIS is usually caused by hvKP and often occurs in people with immune deficiency, such as that caused by diabetes, alcohol abuse, malignant tumours or chronic obstructive pulmonary disease (COPD); and is common in patients undergoing glucocorticoid therapy, especially those with diabetes.11,12 The explanation for this may not only be related to immunodeficiency in patients with diabetes, but also to greater vascular permeability, which is conducive to bacterial invasion. With regard to the ethnicity of patents with KPIS, they are typically Asian. In the study by Abdallah et al., 69% of the participants experienced liver abscessation because of Kp infection, and in the US and Europe, 41% and <6% of patients, respectively, had a pyogenic liver abscess because of Kp. In addition, Kp was more common in Asian patients than in non-Asian patients (50% vs. 27%, respectively). 13 The rate of detection of Kp in the faeces is significantly higher in Asia than in Europe or the US (75% vs. 10%, respectively). The higher prevalence and colonisation rate of Kp in the intestines of Asian people may account for the higher incidence in such populations.14–16
An analysis of 11 cases ( Table 3 ) showed that the symptoms of KPIS are varied, but fever is common. Some patients present with an altered state of consciousness, and they may be in a more critical state. The vital signs of patients at the time of admission indicate that most have quick sequential organ failure assessment (qSOFA) scores 17 of >2 points, which implies a tendency toward sepsis, and the mortality rate associated with the condition is high (up to 36%). The qSOFA score of the present patient was <2 points and there were no positive signs on physical examination, but sepsis was identified on the basis of blood testing. Thus, we can conclude that even patients with KPIS who have atypical symptoms are likely to have sepsis.
List of cases of Klebsiella pneumoniae invasion syndrome reported between 2016 and 2020.

Year, year of admission of the patient to hospital; Sepsis, defined using a qSOFA ≥2 (yes or no).
When KPIS is suspected, the identification of all the sites of infection is essential. The lungs and liver are the most common sites of infection. 1 Bacteria enter the liver from the enterohepatic circulation and cause liver abscesses, then access the pulmonary circulatory system and invade remote sites. However, the condition of the patients is more critical and the mortality rate is higher when there is intracranial infection. CT examination of the head, chest and abdomen are recommended in the first instance, and the use of these techniques can reduce the duration of infection and the risk of its dissemination, as well as improving the diagnostic accuracy. The present patient underwent chest and head CT examinations, enhanced abdominal CT, and cranial MRI examination. When the results of a cranial CT examination are suggestive of brain abscessation, a diagnosis can be confirmed using MRI. In addition, enhanced CT of the abdomen can assist with the differentiation of abscesses from tumours with central necrosis. Because most patients are immunodeficient and chest CTs usually show cavitation or necrosis, these lesions must be differentiated from those caused by TB. The present patient was initially diagnosed as having TB, but the purified protein derivative and TB spot tests were both negative, and sputum culture indicated Kp infection.
HvKP is usually sensitive to β-lactam antibiotics, and meropenem is typically administered ( Table 3 ). The patient we admitted was treated with meropenem for the following reasons: 1) he was in a critical state, with sepsis and bacteraemia; 2) he was hypoproteinaemic, and meropenem has low protein-binding affinity; and 3) he had multiple sites of infection, including the liver, lungs and brain. Meropenem is able to achieve effective therapeutic concentrations in all these tissues and has been shown not to be significantly neurotoxic. The route of administration was a continuous pump, which provides an appropriate duration of action of meropenem.18–19 The patient was administered meropenem 2 g every 8 hours via a pump over nearly 3 hours on each occasion, to maximise its efficacy in the brain, as previously described. 20 However, the prevalence of antibiotic resistance in Kp has increased in recent years. 8 Therefore, the sensitivity of the cultured bacteria to a range of anti-bacterial agents should be assessed and pharmacokinetic and pharmacodynamic factors should also be taken into consideration.
The present patient recovered quickly after puncture drainage, implying that this is an effective method of treatment, especially for patients with endophthalmitis, and may be necessary because most antibiotics are only found in the vitreous at low concentrations. Thus, vitrectomy should be performed as soon as possible in patients who respond poorly to antibiotic treatment or who are critically ill. The present patient responded poorly to drug treatment alone, but his symptoms and blood parameters improved significantly after vitrectomy and drainage of the liver abscess ( Table 2 ). In addition, it has previously been recommended that a 6- to 8-week course of antibiotics should be administered,3,4,7,8 but whereas the present patient’s lung abscess had been almost completely reabsorbed after approximately 6 weeks, the intrahepatic and intracranial lesions were smaller but still remained after 8 weeks. However, the abscesses could not be identified after a further 2 weeks of antibacterial treatment. Therefore, the duration of antibiotic administration should depend on the results of imaging in individual patients.
KPIS is common in Asian people with diabetes and the incidence of sepsis is high5,6. Therefore, patients should be thoroughly examined to identify all the sites of infection. In patients with hypoproteinaemia and multiple sites of severe infection, meropenem administration via pump is recommended as the first-line treatment, but the duration of antibiotic treatment should depend on the results of laboratory testing and imaging. Puncture and drainage of lesions can significantly improve the prognosis of patients and should be performed in a timely manner, especially in those who meet the indications and are in a critical condition. However, because only one patient has been reported herein and he was not followed up long term, our conclusions may not be universally applicable.
Conclusion
KPIS is a critical multi-site infectious condition that is usually caused by hvKP. It is common in Asian patients with diabetes and results in sepsis, which is associated with a high mortality rate. When KPIS is suspected, attention should be paid to the identification of all the sites of infection and the selection of the most appropriate antibiotics. However, it is even more important to perform drainage via puncture in a timely manner to improve the prognosis of the patient.
Footnotes
Ethics statement
This was a retrospective study that was approved for publication by the Institutional Review Board of Beijing Tsinghua Changgung Hospital. We obtained the patient’s consent for treatment, but have de-identified the patient data presented herein; therefore, the requirement for consent for publication was waived. The datasets analysed during the present study are available from the author on reasonable request. This reporting of the case followed the CARE guidelines. 21
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
C-GZ contributed to manuscript writing and was responsible for the patient. YW and MD contributed to the analysis of data. X-YZ and X-YC were responsible for the revision of the manuscript. All the authors approved the submitted version of the manuscript.