
Abstract
Objective
To evaluate a novel reverse dot blot assay for the simultaneous detection six types of common α-thalassaemia alleles (three deletional and three common non-deletional mutations) and 19 types of common β-thalassaemia alleles in a Chinese population.
Methods
Genomic DNA samples were collected from three hospitals in southern China. The novel thalassaemia gene assay involved one multiplex polymerase chain reaction amplification system and one round of hybridization. Each of the clinically validated DNA samples was re-tested using the new multiplex polymerase chain reaction/reverse dot blot assay II (M-PCR/RDB II) assay in a double-blind manner.
Results
A total of 1060 unrelated study participants, including 829 patients with thalassaemia and 231 healthy control subjects, were analysed. The whole PCR and RDB procedures were completed in 260 min. All the samples, including heterozygous thalassaemia, homozygous thalassaemia and compound heterozygous thalassaemia, were correctly genotyped, yielding 100% concordance with the reference assays. HKαα/--SEA and HKαα/−α4.2, which were not included in the detection panel, yielded a contradictory result with this new assay.
Conclusion
The novel M-PCR/RDB II assay was simple, rapid and accurate, suggesting that it could be used for the genetic screening and clinical diagnosis of common α-thalassaemia and β-thalassaemia variants in Chinese populations.
Introduction
The thalassaemia syndrome is the most common single gene mutation in humans.1,2 There are two main types of thalassaemia known as α-thalassaemia and β-thalassaemia: α-thalassaemia, arises from deletions or point mutations of the α-globin genes, leading to diminished or absent synthesis of the α-globin chain of haemoglobin (Hb); 3 and β-thalassaemia is characterized by mutations on the β-globin gene that leads either to a decrease or absent β-globin chain synthesis. 4
Thalassaemia is prevalent in tropical and subtropical areas such as the Mediterranean basin, Africa, the Middle East, the Indian subcontinent and Southeast Asia.5,6 Previous studies demonstrated a high prevalence of thalassaemia in southern China, especially in Guangxi, Guangdong and Hainan provinces.7–11 The --SEA deletion was the most frequent in α-thalassaemia in southern China, followed by -α3.7 and -α4.2; and the frequency of the CD41-42 (–TCTT) mutation was the highest in β-thalassaemia, followed by IVS-II-654 (C > T), –28 (A > G) and CD17.7–9,11 Patients in each ethnic population carry their own specific types of mutations, including a few very common ones and a variable number of rare ones.7–9,11
Several molecular methods for the diagnosis of thalassaemia mutations have been described, including next-generation sequencing, 12 amplification refractory mutation system,13,14 allele-specific oligonucleotide polymerase chain reaction, 15 denaturing high performance liquid chromatography (DHPLC), 16 reverse dot blot 17 and gap-polymerase chain reaction (Gap-PCR).2,5,7 However, the main drawbacks of these methods are that they are expensive, labour intensive and have limited resolution.12,17 Our previous study reported a multiplex PCR/reverse dot blot assay I (M-PCR/RDB I). 17 It is now widely used for clinical thalassaemia diagnosis in southern China. Nevertheless, M-PCR/RDB I involves two multiplex PCR amplification systems for α-thalassaemia and β-thalassaemia, so it is still technically time-consuming.
This current study describes the improvement of the M-PCR/RDB I assay. The new M-PCR/RDB II assay includes one multiplex PCR and one round of RDB, so that the procedure time is greatly reduced. Moreover, the Hb Westmead (Hb WS (αWSα), HBA2: c.369C > G) mutation was added into the new assay system. This new M-PCR/RDB II assay was designed to detect six types of common α-thalassaemia mutations and 19 types of common β-thalassaemia mutations simultaneously. This current study reports the diagnostic reliability of the new M-PCR/RDB II assay in patients from southern China.
Patients and methods
Study population
This study collected samples from patients with thalassaemia that had been previously genotyped using the reference method (RDB, Gap-PCR and PCR-Sanger sequencing) between January 2010 and December 2012 from Guangdong Women and Children Hospital, Hainan Women and Children Hospital and General Hospital of Guangzhou Military Command of PLA.9–11 The patients with thalassaemia were intentionally selected and the healthy controls were randomly selected from patients undergoing routine check-ups at the Guangdong Women and Children Hospital. In addition, patients with rare haemoglobin genotypes confirmed by Guangdong Hybribio Limited Corporation were also tested with this new kit. These samples were used to test the specificity and accuracy of the newly developed assay in a double-blind manner.
The study was approved by the Ethics Committees of all three participating hospitals: Ethics Committee of Guangdong Women and Children Hospital (no. 2012042), approved in Guangzhou, 4 April 2012; Ethics Committee of Hainan Women and Children Hospital (no. 2011021), approved in Haikou, 9 September 2011; Ethics Committee of General Hospital of Guangzhou Military Command of PLA (no. 2011EC021, approved in Guangzhou, 8 December 2011). As the patient data were analysed anonymously and the blood samples in this study were used after the clinical diagnosis (i.e. routine blood samples), a waiver of the need for written consent was approved by the Ethics Committees of the three hospitals. The study is reported in accordance with the STROBE guidelines. 18 The patient details were de-identified so that the identity of any patient might not be ascertained in any way.
Genomic DNA sample preparation
Genomic DNA from the study participants was extracted from peripheral blood leukocytes using a DNA Prep Kit (Guangdong Hybribio Limited Corporation, Chaozhou, Guangdong Province, China). The DNA concentration was determined using a NanoDrop™ One/One C Microvolume UV-Vis Spectrophotometer (Thermo Fisher Scientific, Rockford, IL, USA) at a wavelength of 260 nm. The purity of the DNA was checked from the value of the 260/280 nm ratio. These DNA samples were used for the subsequent PCR analysis. Both the clinical test (the reference method of RDB, Gap-PCR and PCR-Sanger sequencing) and the validation test (M-PCR/RDB II) were performed in the clinical diagnosis laboratory of Guangdong Hybribio Limited Corporation, Chaozhou, Guangdong Province, China.
Design of primers and probes
The thalassaemia detection kit was designed and made by Guangdong Hybribio Limited Corporation. The detection kit included one PCR reaction system as follows. Five sets of primers of the M-PCR assay were designed to amplify three α-thalassaemia deletions (the Southeast Asian [−SEA], the rightward deletion [−α 3 . 7 ] and the leftward deletion [−α 4 . 2 ] on chromosome 16; the three α-globin gene mutations: Hb Constant Spring [Hb CS (αCSα) HBA2: c.427T > C], Hb Quong Sze [Hb QS (αQSα), HBA2: c.377T > C], Hb Westmead [Hb WS (αWSα), HBA2: c.369C > G]; and the 19 β-globin gene mutations [‒28 (A > G), HBB: c.‒78A > G; ‒29 (A > G), HBB: c.‒79A > G; Cap (−AAAC, A > C), HBB: c.−11_−8delAAAC, c.−50A > C; initiation codon ATG > AGG, HBB: c.2T > G; codons 14/15 (+G), HBB: c. 45_46insG; codon 17 (A > T), HBB: c.52A > T; codons 27/28 (+C), HBB: c. 84_85insC; codon 26 (G > A), HBB: c.79G > A; codon 31 (‒C), HBB: c.94delC; codons 41/42 (‒TCTT), HBB: c. 126_129delCTTT; codon 43 (G > T), HBB: c.130G > T; codons 71/72 (+A), HBB: c.216_217insA; IVS-I-1 (G > A, G > T), HBB: c.92 + 1G > A, c.92 + 1G > T; IVS-I-5 (G > C), HBB: c. 92 + 5G > C; IVS-II-654 (C > T), HBB: c.316-197C > T; ‒30 (T > C), HBB: c.‒80T > C; ‒32 (C > A), HBB: c.‒82C > A]. One 1800 base pair (bp) fragment of α-2 globin gene was amplified as a normal control (marked NP on the hybridization membrane). Oligo 6.31 (Molecular Biology Insights, Colorado Springs, CO, USA) software was used to design the primers and probes. Schematic representation of the six types of α-thalassaemia allele location in the α-gene cluster is shown in Figure 1a. All probes were immobilized on a nylon membrane. Their localization in the membrane is shown in Figure 1b. The detailed information of the primers and probes are presented in Tables 1 and 2.

(a) Schematic representation of the six types of α-thalassaemia allele location in the α-gene cluster. (b) The probe location in the gene chip. NP indicates a fragment for α2 gene, as the control for −SEA, −α3.7 and −α4.2; −28N: the control for −28M,−29M,−30M, and −32M; 41−42N: the control for 41−42M and 43M; 17N: the control for 17M and 14−15M; IVS-I-1N: the control for IVS-I-1M and IVS-I-5M; βEN, 654N, 71−72N, 27−28N, CSN, QSN, and WSN are the controls for βEM, 654M, 71−72M, 27−28M, CSM, QSM, and WSM, respectively. No control point for CapM, IntM and 31M.
Detailed information about the primers used in the novel polymerase chain reaction/reverse dot blot assay II assay.

Detailed information about the probes used in the thalassaemia gene chip.

N, normal control; M, mutation; NP, α-globin gene normal control; CSN, haemoglobin Constant Spring, QS, haemoglobin Quong Sze; WS, haemoglobin Westmead.
Multiplex PCR amplification
The assay was performed according to the manufacturer's protocol (Guangdong Hybribio Limited Corporation). Briefly, the α-thalassaemia and β-thalassaemia PCRs (i.e. the reaction system) were performed in a PCR appliance (GeneTouch; BIOER, Hangzhou, China), with a reaction volume of 50 μl containing 5 μl of DNA template, 2.5 U HotStart DNA polymerase and 44.5 μl PCR MIX (100 μmol/l Primer MIX: 1.25 μl, 25 mmol/l MgCl2; 3 μl, 10 × PCR buffer; 5 μl, 5 × PCR enhancer; 7 μl, 25 mmol/l dNTPs; 0.8 μl, H2O; 27.45 μl). The cycling programme involved preliminary denaturation at 95°C for 15 min, followed by 35 cycles of denaturation at 97°C for 50 s, annealing at 60°C for 60 s, and elongation at 72°C for 120 s, followed by a final elongation step at 72°C for 10 min. The amplicons of the reaction system (one tube) were subsequently denatured and subjected to hybridization.
Flow-through hybridization
Hybridization reactions were performed using a thalassaemia gene diagnostic kit and flow-through hybridization kit (Guangdong Hybribio Limited Corporation) as described previously. 17 The assay utilized flow-through hybridization technology (HB2012A; Guangdong Hybribio Limited Corporation). After hybridization, a blue-purple precipitate at the probe dot could be discerned. The results were interpreted by direct visualization.
Reference methods
For the reference methods, all of the thalassaemia alleles were characterized by a combination of techniques including M-PCR/RDB I, direct DNA sequencing, RDB and a two-round nested PCR strategy. Three types of α-thalassaemia deletion (−SEA, −α3.7 and −α4.2) and two types of α-thalassaemia mutation (Hb CS and Hb QS) were analysed by M-PCR/RDB I (Guangdong Hybribio Limited Corporation). 17 The α-thalassaemia mutations (Hb CS, Hb QS and Hb WS) were identified by the RDB assay (Decipher Bioscience Shenzhen, Shenzhen, China) as described previously. 19 The mutation of α-thalassaemia (Hb WS) was also amplified and sequenced using an ABI3700 automated sequencer (Applied Biosystems, Foster City, CA, USA) as described previously. 19 A two-round nested PCR strategy was carried out to detect the possible presence of HK αα, a rare α- thalassaemia mutation, which has been reported in southern Chinese subjects.20,21
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. The agreement between M-PCR/RDB II and the reference methods was determined by kappa statistics and McNemar’s χ -test. A P-value <0.05 was considered statistically significant.
Results
This study collected samples from 1060 unrelated study participants, including 829 patients with thalassaemia and 231 healthy control subjects as follows: Guangdong Women and Children Hospital (n = 400), Hainan Women and Children Hospital (n = 260) and General Hospital of Guangzhou Military Command of PLA (n = 400). A further 32 patients with rare genotypes of haemoglobin were also tested with the new kit, including 30 patients with Hong Kong αα (HKαα)/--SEA and two patients with of HKαα/−α4.2. The whole PCR and RDB procedure in the M-PCR/RDB II assay could be completed in 260 min.
In a verification test, a total of 1060 genomic DNA pre-characterized samples (829 patients with thalassaemia and 231 healthy control subjects) were analysed with the M-PCR/RDB II assay in a double-blind manner. Valid hybridization results were obtained for all samples. The hybridization results of the M-PCR/RDB II assay are presented in Table 3, which included heterozygous thalassaemia, homozygous thalassaemia and compound heterozygous thalassaemia (Figure 2).
Results of a verification test that analysed genomic DNA pre-characterized samples from 829 patients with thalassaemia using the novel polymerase chain reaction/reverse dot blot assay II assay in a double-blind manner.

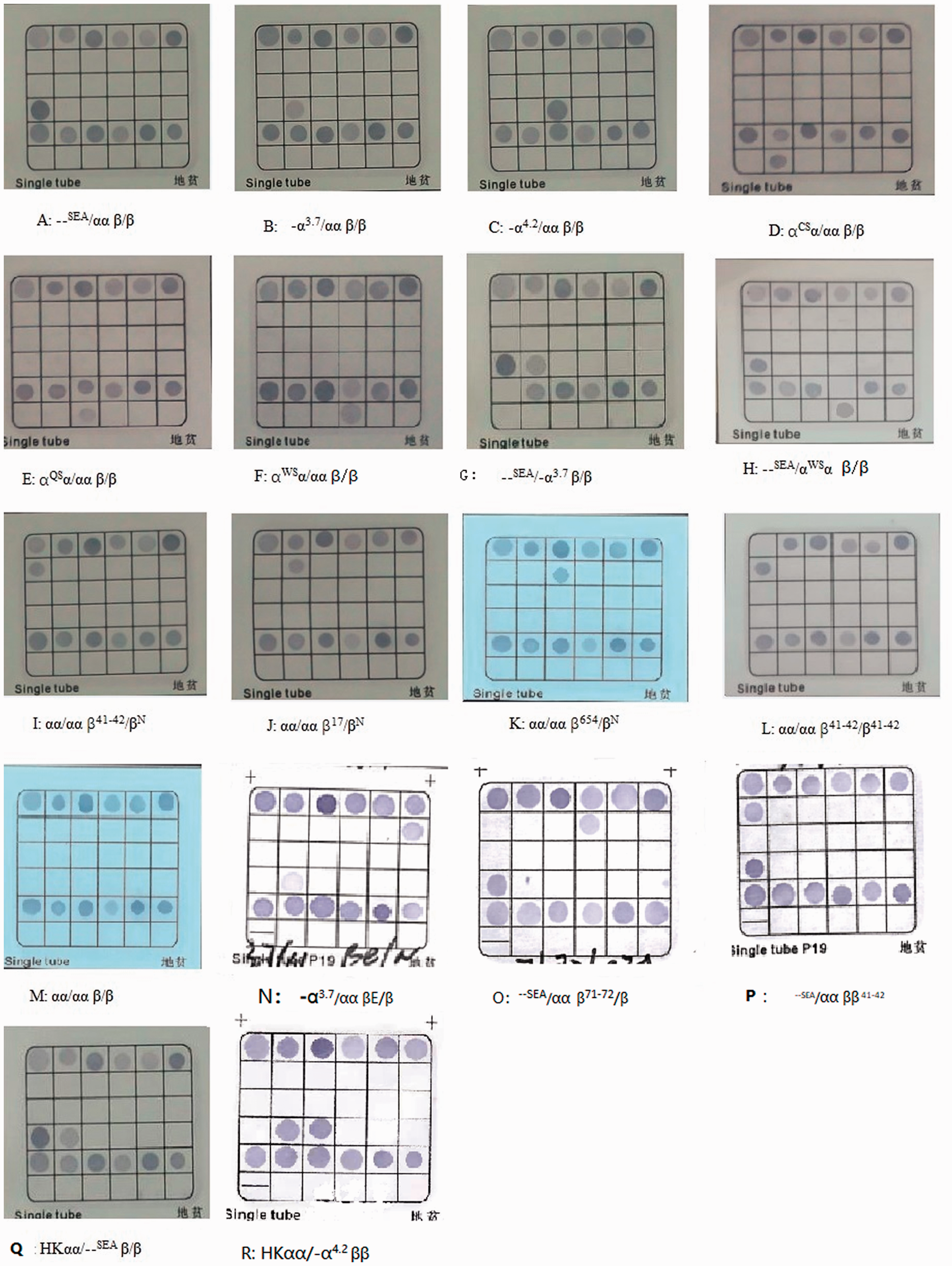
Hybridization results of the novel polymerase chain reaction/reverse dot blot assay II assay. (a) --SEA/αα βN/βN; (b) −α3.7/αα βN/βN; (c) −α4.2/αα βN/βN; (d) αCSα/αα βN/βN; (e) αQSα/αα βN/βN; (f) αWSα/αα βN/βN; (g) --SEA/−α3.7 βN/βN; (h) --SEA/αWSα βN/βN; (i) αα/αα β41–42/βN; (j) αα/αα β17/βN; (k) αα/αα β654/βN; (l) αα/αα β41–42/β41–42; (m) αα/αα βN/βN; (n) −α3.7/αα βN/βE; (o) --SEA/αα β71–72/βN; (p) --SEA/αα β41–42/βN; (q) HKαα/--SEA βN/βN; (r) HKαα/−α4.2 βN/βN.
Agreement between the M-PCR/RDB II assay and the reference methods were in absolute concordance (kappa = 1, P <0.001) for detection of the three α-globin deletions (−SEA, −α3.7, −α4.2), two α-globin mutations (CS, QS) and 19 types of β-thalassaemia mutations [−30(T-C), −32(C–A), −28(A-G), −29(A-G), Cap(−AAAC, A-C), Int(T-G), CD14/15(+G), CD17(A-T), CD27/28(+C), βE(G-A), CD31(−C) CD41/42 (−TCTT), CD43(G-T), CD71/72(+A), IVS-I-1(G-T, G-A), IVS-I-5(G-C), IVS-II-654(C-T)]. The Hb WS were also successfully identified using M-PCR/RDB II assay and the results showed 100% concordance with the direct sequence analysis (Table 3, Figure 2).
The current study also tested 30 patients with HKαα/--SEA and two patients with HKαα/-α4.2 using the M-PCR/RDB II assay. The NP (α-globin gene normal control), −α3.7 and --SEA dots were positive on the chip for the HKαα/--SEA patients (n = 30) (Figure 2q); and the NP, -α3.7 and -α4.2 dots on the chip were positive for two patients with HKαα/-α4.2 (Figure 2r), which was not in conformity with the principle of the kit that NP on the chip should be negative when homozygote or compound heterozygotes of -α3.7, α4.2 and --SEA were detected.
Discussion
Thalassaemia is a common genetic disease in southern China, which has a large impact on the public health burden in these epidemic areas.7,8,11,22 A screening test, comprising complete blood count, haemoglobin quantification by capillary electrophoresis and high performance liquid chromatography, may not be able to screen out all the thalassaemia diseases. Laboratory diagnosis of thalassaemia requires molecular analysis. With the advance of molecular diagnosis, the genetic diagnosis of thalassaemia can be easily performed by direct analysis of the affected globin genes. It is becoming an important tool in the prevention and control programme of thalassaemia in China. However, most of the current clinically used molecular diagnostic methods for thalassaemia are still technically time-consuming.12,17
This current study describes the further development of an earlier first-generation kit for thalassaemia detection (M-PCR/RDB I). 17 The earlier kit involved two multiplex PCR amplification systems for α- thalassaemia and β-thalassaemia and it has been shown to be an accurate and sensitive method for the identification of thalassaemia genotypes, with it subsequently becoming widely used in the clinic for the molecular diagnosis of thalassaemia. 17 This improved M-PCR/RDB II kit sees the number of PCRs reduced from two to one.
The described M-PCR/RDB II has several advantages over the previously developed M-PCR/RDB I and any other methods currently applied clinically. The process of sample preparation is simpler because the new M-PCR/RDB II assay only involves one multiplex PCR amplification system (i.e. one tube), which makes it more convenient. In addition, Hb WS was added into the new M-PCR/RDB II assay and it was successfully detected. Traditionally, the RDB analysis and a single-tube multiplex PCR was used to detect non-deletion mutations of the α-globin gene and β-globin mutations, so this needed two PCR reactions. α-globin gene deletions are often diagnosed by gap-PCR,2,5,7 but this is time-consuming because its conventional method requires post-PCR work. The new M-PCR/RDB II assay combines three PCRs (two for mutations of the α-globin gene and β-globin mutations; and one for α-globin gene deletions) into one PCR in a single tube; and the improved RDB-based technology made the analysis process simpler.
It is acknowledged that the new M-PCR/RDB II assay has some limitations. For example, a rare α-thalassaemia mutation −HKαα genotype, which was observed in previous reports in China,20,21,23,24 showed conflicting results when the M-PCR/RDB II assay was used, although a single carrier of the HKαα allele is unlikely to suffer any deleterious effects.23,24 The HKαα allele is an unusual rearrangement of the α-globin gene cluster containing both the −α3.7 (rightward) and αααanti 4.2 crossover deletion/duplication. 25 Clinically, HKαα/αα and HKαα/−α3.7 were often mistakenly identified as αα/−α3.7 by the M-PCR/RDB II assay and the earlier version M-PCR/RDB I assay; while HKαα/--SEA presented with −α3.7 and --SEA hybridization dots and one α-globin gene normal control dot, but this presentation is theoretically impossible for an α-thalassaemia genotype. This contradictory gene chip result meant that the current study had to refer to other methods for a final diagnosis. Therefore, during the clinical application of this novel M-PCR/RDB II assay, it will be necessary to be cautious if only the positive result of α2 and -α3.7 (or α2 and -α4.2) are observed, because the actual genotype might be αα/-α3.7 (or αα/-α4.2), αα/HKαα or HKαα/-α3.7 (or HKαα/-α4.2). Further confirmation will be necessary using 2-round nested PCR analysis or by pedigree analysis. 20 In Chinese carriers of silent deletional α-thalassaemia the frequencies of the HKαα and anti-HKαα alleles were 2.27% and 0.35% in -α3.7 and -α4.2 carriers, respectively. 20 Given the rarity of the HKαα and anti-HKαα alleles, a routine screening for these two rearrangements is not necessary on most occasions. 20
In the clinical situation where a couple requests prenatal diagnosis for thalassaemia, if one of the parents was diagnosed with αα/-α3.7 and the other parent carried a normal α-globin gene, then the fetus would not need further gene diagnosis. If one of the parents was diagnosed with αα/-α3.7 using the new M-PCR/RDB II assay, and the other parent carried an α0 (such as --SEA) thalassaemia gene, then the fetus should be further screened because they could possibly be a HKαα carrier. The levels of Hb, mean corpuscular volume and mean corpuscular haemoglobin of HKαα/αα carries are similar to those of -α3.7/αα and HKαα/--SEA carriers and Hb is usually over 100 g/l. 22,23 But --SEA/-α3.7 presents as haemoglobin H disease, usually with Hb <100 g/l. 24
In conclusion, the simplicity and the universality of this improved single-tube multiplex-PCR-based RDB assay could significantly reduce the time and the complexity of screening for the common genotypes of α-thalassaemia and β-thalassaemia. It is especially suitable for routine clinical diagnosis of thalassaemia in Chinese populations.
Footnotes
Author contributions
L.Y.Y. and L.X.X. conceptualized and designed the study, coordinated and supervised data collection, and reviewed and revised the manuscript. H.F.L., L.Y.Y., X.B.Z. and H.Y. analysed the data, drafted the initial manuscript and revised the manuscript. M.L., L.J.L. and Y.Y.G. collected the data, did the molecular analysis and carried out the initial analysis. M.L., Y.Y.G., L.J.L., F.L. and X.B.Z. participated in the sample and data collection. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was partially supported by the Natural Science Foundation of Guangdong Province (grant no. 2016A030307035). The funders had no role in the study design and data analysis, decision to publish or submission of the manuscript.